Introduction
The importance of sagittal alignment has been recognized in degenerative lumbar disease surgery. Restoration of sagittal plane balance is associated closely with favorable patient outcomes in spinal deformity surgeries, including reduced pain, minimal disability, and better quality of life [1,2]. Due to the well documented prominence of spinopelvic sagittal balance, lumbar lordosis (LL), correlated with pelvic incidence (PI), is considered a requirement for a balanced sagittal posture [3]. Adequate LL followed by sufficient thoracic kyphosis (TK) could lead to harmonious global sagittal balance, resulting in favorable clinical and radiologic outcomes [4]. Though the importance of sagittal balance restoration in short-level degenerative lumbar fusion surgery was underestimated previously, progress in research on global sagittal balance has thrust sagittal balance restoration into the spotlight. Lack of adequate LL achieved following fusion surgery can accelerate degeneration of adjacent segments [5,6], potentially resulting in a poor quality of life and overall function [2]. Consequently, lumbar hypolordosis following previous posterior fusion surgery has become a growing problem in recent years [7].
Though short-level lumbar interbody fusion surgery is known to improve local sagittal alignment, its effects on regional LL and global sagittal alignment remain unclear [8]. Lateral lumbar interbody fusion (LLIF) is an alternative technique to conventional anterior and posterior lumbar interbody fusion (PLIF) for managing various pathologies of degenerative lumbar diseases [9,10]. LLIF is a minimally invasive surgical method that permits the placement of interbody cages that are larger in size than those placed using PLIF [9-11]. This alternative method might provide a better radiologic restoration and sufficient correction of local and regional LL or may somewhat restore global sagittal alignment.
However, there is a paucity of data on postoperative changes in regional LL and global sagittal parameters following short-level PLIF and LLIF. Additionally, the lack of studies that compare the impact of radiographic changes yielded by the two surgical techniques warranted the conduct of the current study to compare the radiographic impact of LLIF and PLIF on local and global sagittal alignments.
Materials and Methods
1. Study design
After obtaining approval from Konan Kosei Hospital ethics comittees (IRB approved no., 25-022[0174]), we prospectively enrolled and retrospectively reviewed the radiographic records of consecutive patients who underwent PLIF between 2009 and 2013, and who underwent LLIF between 2013 and 2016. The following were the exclusion criteria: (1) revision surgery, (2) ≥4-level involvement, (3) L5–S fusion surgery, (4) decompression surgery at another level, (5) ≥grade 2 osteotomy on the Schwab classification [12], (6) a coronal Cobb angle >20°, (7) <2 years of follow-up, (8) additional spine surgery during the follow-up period, and (9) other disease entities, such as tumors, traumas, or infections. Finally, 245 patients were included in this study: 144 consecutive patients who had undergone PLIF (average age, 67.19±11.90 years; male, 68; female, 76) and 101 consecutive patients who had undergone LLIF (average age, 70.95±6.24 years; male, 47; female, 54).
2. Radiographic analysis
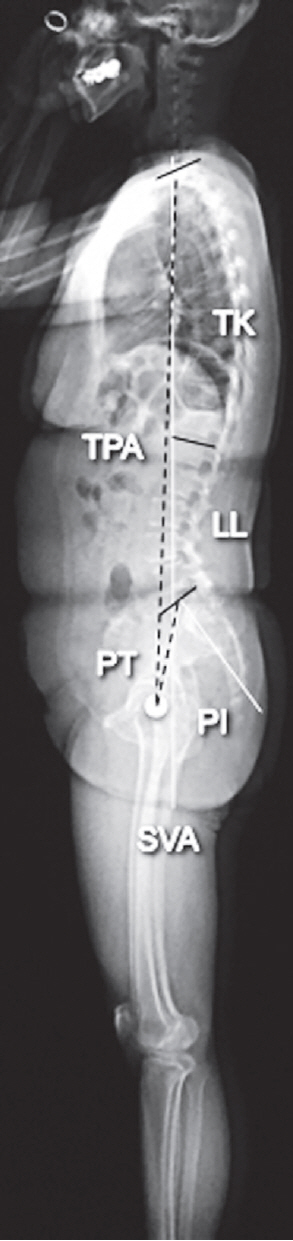
Preoperative and 2-year postoperative anteroposterior and lateral radiographs of the lumbar spine and whole-spine acquired with the subjects in an upright standing position were obtained. The radiologic parameters included the following (Fig. 1): (1) segmental lordotic angle (Cobb angle between the upper and lower endplates of each fused segment), (2) disk height (the mean shortest distance between the lower and upper endplates at the anterior and posterior borders), (3) LL (Cobb angle between the upper endplates of both L1 and S1), (4) pelvic tilt (PT; angle between the line joining the midpoint of the upper endplate of S1 with the center of the hip joint and a vertical line), (5) PI (angle between the line linking the midpoint of the upper endplate of S1 with the center of the hip joint and a line vertical to the upper endplate of the sacrum), (6) C7 sagittal vertical axis (SVA; distance between the posterosuperior corner of S1 and a vertical line from the C7 body center), (7) TK (Cobb angle between the upper endplate of T1 and the lower endplate of T12), and (8) T1 pelvic angle (angle between the line from the femoral head axis to the centroid of T1, and the line from the femoral head axis to the middle of the S1 superior endplate) [13].
3. Surgical procedure for posterior lumbar interbody fusion
The general technique for PLIF has been described previously [14,15]. Briefly, after bilateral pedicle screw insertion, an intervertebral space was created using an intervertebral distractor. Total discectomy was performed after connecting pedicle screws using a rod, and two interbody cages were inserted. The cage height and angle ranged from 7 mm to 11 mm and 0° to 12°, respectively. The bone graft was packed around the cages, and the pedicle screws were disconnected from the rod to relieve the distraction force and, then, reconnected.
4. Surgical procedure for lateral lumbar interbody fusion
The general technique for LLIF has been described previously [9,16]. Briefly, extremely lateral lumbar fusion using Coroent cages (NuVasive Inc., San Diego, CA, USA) of the 10° lordotic type was performed in all cases. The cage width, height, and length ranged from 45 to 55 mm, 8 to 12 mm, and 18 to 22 mm, respectively. All the patients underwent bilateral pedicle screw fixation after LLIF, avoiding strong any compression force on the pedicle screws.
Results
Of the 144 patients who underwent PLIF (193 fused levels), 109, 21, and 14 patients underwent 1-, 2-, and 3-level fusions, respectively. In comparison, of 101 patients who underwent LLIF (159 fused levels), 58, 28, and 15 patients underwent 1-, 2-, and 3-level fusions, respectively. Patients’ backgrounds and preoperative radiographic parameters for any level of fusion did not differ significantly between PLIF and LLIF procedures (Table 1). The L4–L5 level was the most frequently involved level (206/352, 58.5%), followed by L3–L4 (113/352, 32.1%) and L2–L3 (33/352, 9.4%).
The LLIF group exhibited significantly greater changes at 1-level fusion compared to the PLIF group in the parameters of segmental lordotic angle (5.1°±5.8° versus 2.1°±5.0°, p<0.001), disk height (4.2±2.3 mm versus 2.2±2.0 mm, p<0.001), LL (7.8°±7.6° versus 3.9°±8.6°, p=0.004), and PI–LL (−6.9°±6.8° versus −3.6°±10.1°, p=0.03) (Table 1), but not of others.
Similarly, the LLIF group exhibited significantly greater changes at 2-level fusion compared to the PLIF group in the parameters of segmental lordotic angle (4.8°±4.0° versus 2.6°±3.2°, p=0.04), disk height (4.0±1.5 mm versus 2.4±1.9 mm, p=0.002), LL (8.4°±7.0° versus 2.1°±6.7°, p=0.003), and PI–LL (−9.0°±7.3° versus −3.4°±7.4°, p=0.001) (Table 2).
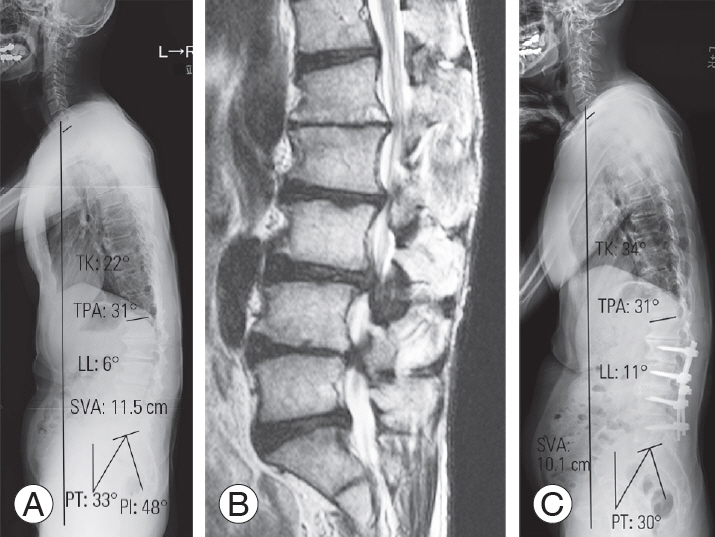
In contrast, while changes in the LLIF group did not differ significantly from that in the PLIF group at 3-level fusion in the parameters of segmental lordotic angle (4.8°±3.3° versus 2.6°±3.2°, p=0.08) and disk height (4.1±2.1 mm versus 2.9±1.1 mm, p=0.07) (Table 3), significantly greater changes were observed in LL (12.1°±11.1° versus 4.2°±9.1°, p=0.047) and PI–LL (−11.2°±11.3° versus −3.0°±9.3°, p=0.043) (Figs. 2, 3). Additionally, significantly greater changes were observed in the LLIF group regarding PT (−6.4°±4.9° versus −2.5°±5.3°, p=0.049) and TK (7.8°±11.8° versus −0.3°±9.7°, p=0.047) (Table 3).
Discussion
To our knowledge, this is the first study that compared sagittal realignment after PLIF and LLIF in short-level spinal fusion surgeries. Compared to conventional PLIF, we found that LLIF can provide better local lordotic angle, disk height, and LL after 1- and 2-level fusion. Furthermore, the degree of correction of spinopelvic alignment as assessed using PT, as well as TK were significantly greater with 3-level fusion using LLIF. Overall, LLIF has a greater potential than PLIF to correct sagittal alignment even after short-level lumbar interbody fusion.
LLIF was introduced as a treatment for axial low back pain by Ozgur et al. [9], and subsequently used by Oliveira et al. [10], for treating central canal or foraminal stenosis. Compared with conventional open procedures, minimally invasive lumbar interbody fusion using LLIF is more effective at achieving spinal fusion with lower morbidity [10]. Other advantages of the LLIF procedure include gaining better access to the disk space than posterior approaches which permits maximal disk excision, endplate preparation, and use of larger bone grafts [9]. Furthermore, the interbody cage used in LLIF provides an extension-distraction moment to the anterior and middle columns of the lumbar spine, effectively permitting the enlargement of the interbody space and neuroforaminal height [11,17]. When combined with posterior fixation, LLIF facilitates sufficient correction of both coronal and sagittal deformities in patients with degenerative scoliosis, with smaller blood loss and lower morbidity than PLIF [17,18]. However, regarding the effects on global alignment in short-level spinal fusion surgeries, in contrast to PLIF, LLIF is less well understood. Furthermore, the lack of comparative studies between LLIF and PLIF on radiographic outcomes in the context of sagittal balance in patients with degenerative lumbar diseases requiring short-level spinal fusion surgeries warranted the current investigation.
Increase in disc height and segmental lordosis with LLIF is not without precedence [19]. Local sagittal alignment changes after LLIF were demonstrated by Oliveira et al. [10], who reported increases of 41.9% and 13.5%, and Alimi et al. [20] who showed increases of 83% and 26% in the intervertebral disc and foraminal height, respectively. Anand et al. [21], evaluated acquired segmental lordosis after LLIF, and reported that using a 10° cage can provide an 8.1° increase in segmental lordosis in adults with spinal deformity. A similar 10° lordotic cage in the current study provided a 5° increase without posterior column osteotomy in patients with degenerative lumbar diseases requiring short-level spinal fusion surgeries. Therefore, it can be postulated that the background of the patient determines the acquired segmental lordotic angle, which may be greater in patients with deformity and preoperative sagittal imbalance [8]. Correspondingly, the smaller the lordotic cage angle, the smaller is the acquired segmental lordotic angle. Acosta et al. [22] investigated changes in spinal alignment following LLIF with 6° lordotic cages (mean fusion level, 1.8 levels) in 36 patients; they reported that the mean segmental lordosis had increased (5.3 preoperatively versus 8.2 postoperatively, p<0.0001). Additionally, Shiga et al. [23] investigated segmental lordosis after LLIF using 6° lordotic cages in 80 patients (mean fusion level, 1.5 levels), reporting that the average correction angle was 3.8°. Thus, angles of the inserted cages affect the local radiographic outcome.
Although an increase in segmental lordosis has been reported following PLIF, the magnitude of change was smaller than that after LLIF. Cho et al. [8] reported changes in the segmental angle of 0.1°–4.7° in patients with and without sagittal imbalance after 1- or 2-level PLIF using a 4° lordotic cage. While changes in segmental lordosis were not observed with PLIF using 0° cages, modest increase of 0.1° [24], or even a decrease in segmental lordosis from 14.0° to 12.8° [25], after PLIF have been noted. In the conventional PLIF approach, the difficulty associated with inserting hyperlordotic cages to create adequate segmental lordosis, justifies the need for invasive spinal osteotomy [25,26].
We found significant changes in LL; however, global sagittal alignment did not change dramatically after short-level spinal fusion surgeries, indicating a lack of consensus regarding postoperative changes after short-level lumbar interbody fusion. In general, acquired LL could be affected by segmental lordosis at the surgically targeted levels easily; however, there are several compensatory mechanisms in global sagittal alignment. Cho et al. [8] noticed improvement in global sagittal balance after 1- or 2-level PLIF only in patients with preoperative sagittal imbalance. The lack of a significant change in global sagittal alignment, including SVA after either PLIF or LLIF in the present study could be attributed to the fact that most patients did not exhibit preoperative sagittal imbalance.
A few limitations of the current study should be acknowledged. First, as this was a retrospective analysis, the angles of the utilized cages inevitably varied among patients who underwent PLIF. The results cannot necessarily be interpreted as derived from a specific cage design, and may be attributed to the ‘conventional standard’ PLIF although these variations could affect postoperative sagittal alignment. Second, the exclusion of a number of patients who underwent 2- or 3-level fusion affected the statistical power of these cases and calculation of sample size is warranted for future prospective studies to validate our results. Last, despite attempting to insert LLIF cages into the anterior one-third of the disc space, the exact location of interbody cages as demonstrated previously [23], was not investigated in this study. As the results of local lordosis and LL may differ depending on cage locations, this may be a limitation of the current study.
Conclusions
LLIF provided better segmental lordosis and LL than conventional standard PLIF in cases of short-level spinal fusion surgeries. In patients undergoing multilevel interbody fusion surgery, PT and TK were significantly altered after LLIF, and spinopelvic harmony was enhanced, even after short-level LLIF. Thus, LLIF was demonstrated to be a useful lumbar interbody fusion technique, constituting a powerful tool for achieving sagittal realignment with minimal surgical invasiveness.