Introduction
In terms of simultaneous anterior reconstruction and high union rate, posterior lumbar interbody fusion (PLIF) has many advantages over posterolateral fusion (PLF) [1234]. However, at the same time, it has more complications. Surgical site infections (SSIs) develop more often in PLIF, with varying types. Spondylitis around interbody cages and grafted bone were frequent in our cases. It is more difficult to decide whether to preserve or remove the implant in those situations because cage removal is technically demanding and results in total segmental instability and neurological compromise. As far as we know, there has been no study about specific treatments for SSIs in PLIF. We have classified different SSIs in PLIF and analyzed results according to the respective types and treatment methods. Furthermore, risk factors of implant removal were studied.
Materials and Methods
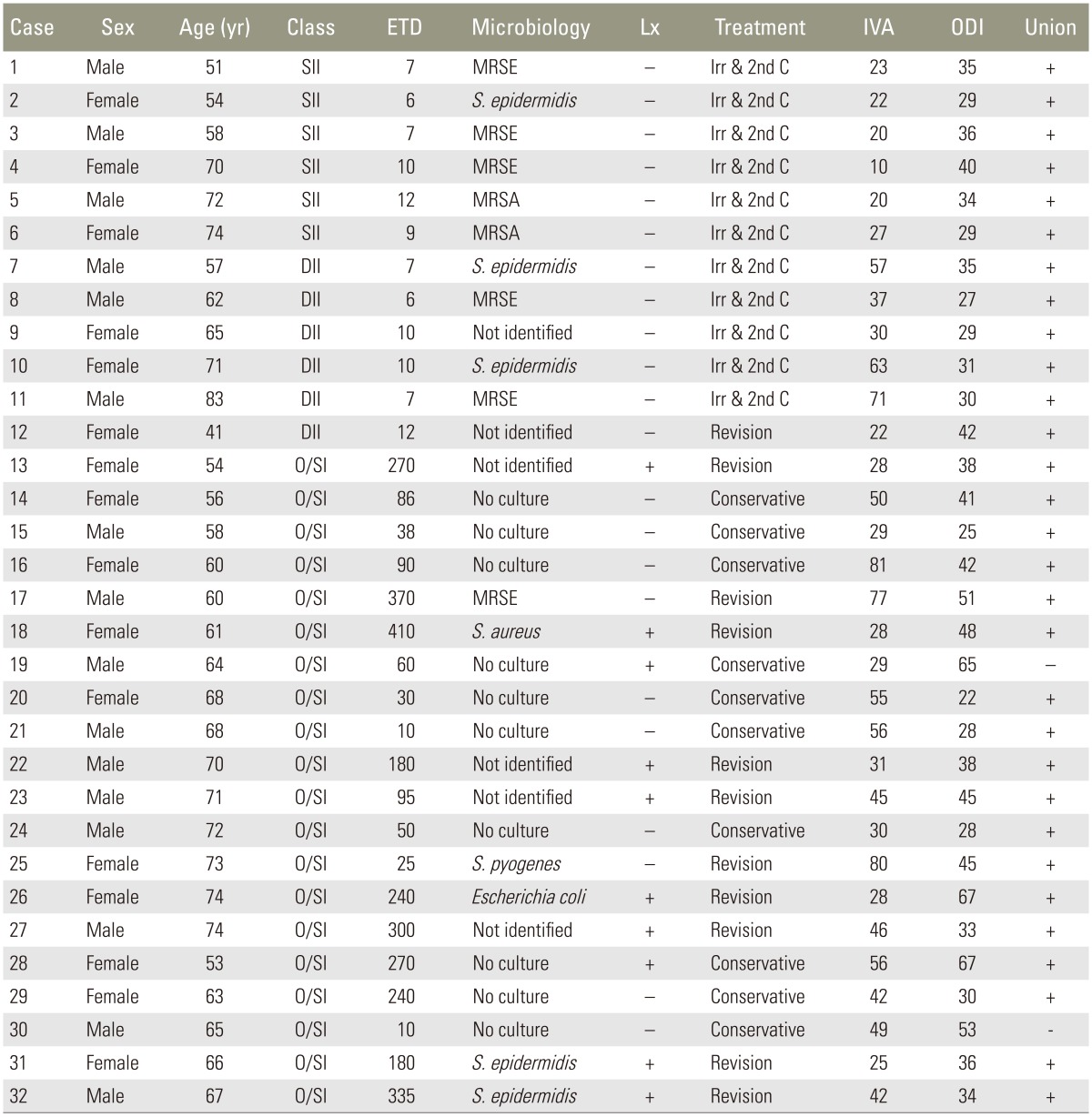
We performed a retrospective observational and case control study in which those who were treated for SSI after PLIF in our institute between 2005 and 2012 and follow for at least 12 months were included. Diagnosis and classification followed the criteria of Center for Disease Control and Prevention (CDC) of the United States. In multi-segment surgeries, PLIF segments that were the same or more than half were regarded as PLIF. Demography, elapsed time to diagnosis (ETD), causative microorganisms, methods of treatment, and their results were investigated and compared according to the classification. The time of diagnosis was defined as when exudate from a surgical incision was found in superficial and deep incisional infections (SII and DII, respectively) and when antibiotics were administered because of laboratory and image findings that suggested organ/space infection (O/SI). In the treatment, the duration of intravenous antibiotics administration and elapsed time to a secondary closure were investigated. Intravenous antibiotics were continued to the time of two consecutive normal range measurements of C-reactive protein (CRP). A secondary closure was implemented when the wound was clear on a visual examination and microorganisms were not identified on a microbiological exam. Risk factors of implant removal were investigated, including age, sex, diabetes mellitus, ETD, and radiological implant loosening. Successful treatment was defined as no more clinical, laboratory, and image finding of infection. Bone union state and functional state using the Oswestry disability index (ODI) were investigated and the differences according to the types and influencing factors were analyzed. For the statistical analysis, T tests, Fisher's exact tests and analysis of variance were used to prove the difference among the types and a logistic regression test was used for the risk factors of implant removal. Significance was defined as pŌēż0.05 and SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA) package was used for all analyses.
Results
There were 32 cases of SSI. Thirty out of 1,381 cases (1.6%) developed at author's hospital and two cases were transferred in from other hospitals. The average age of patients was 64 years (range, 41-91 years) and there were 16 males and 16 females. The number of fusion segments was 1 in 21 cases (65.6%), 2 in 9 cases (28.1%) and 3 in 2 cases (6.3%). Diabetes mellitus was present in 8 cases (25%). According to the CDC classification, there were 6 cases (18.8%) of SII, 6 cases (18.8%) of DII, and 20 cases (62.5%) of O/SI. All O/SIs were spondylitis. The incidence of each type was significantly different (p=0.002). Ten cases (31%) had implant loosening with both pedicle screws and cages at the time of diagnosis. Ten cases did not have microbiological exams. Among the 22 cases that did undergo microbiological exams, 6 cases showed no growth. There were 6 cases of methicillin-resistant Staphylococcus epidermidis (MRSE), 5 cases of methicillin-sensitive Staphylococcus epidermidis (MSSE), 2 cases of methicillin-resistant Staphylococcus aureus (MRSA), and 1 case each of Escherichia coli, methicillin-sensitive Staphylococcus aureus (MSSA), and Staphylococcus pyogenes. All SSIs (6/6) and 5/6 DIIs were treated by repeated irrigation and a secondary closure. The remaining DII underwent vacuum dressing and a secondary closure. Ten out of 20 (50%) cases of O/SI were treated conservatively (Fig. 1) and 10/20 (50%) cases received revision surgeries. When four weeks of intravenous antibiotics did not show any response, or when neurological symptoms developed due to instability or cage retropulsion or epidural abscess, surgery was performed. The elapsed time to secondary closure was 9 days (range, 8-13 days) in SII and 26 days (range, 10-46 days) in DII. The difference was significant (p=0.033). The duration of intravenous antibiotics was 20 days (range, 10-27 days) days in SII, 45 days (range, 11-71 days) in DII, and 45 days (range, 23-81 days) in O/SI. The difference between SII and DII (p=0.030) and between SII and O/SI (p=0.009) was significant, but the difference between DII and O/SI was not significant (p=0.985). In the subgroup analysis of O/SI, the difference was not significant (p=0.987) between the conservative treatment group (48 days; range, 29-81 days) and the revision group (43 days; range, 25-80 days) (Table 1). In the revision group, 9/10 cases underwent posterior one stage simultaneous revision (POSSR). All implants including cages were removed. All infected tissues were excised and the interbody space was irrigated copiously. Bi-cortical auto-iliac bone blocks were grafted in the interbody space. Re-implantation was performed. Widened pedicle holes were charged with fresh frozen allograft bone chips and fusion segments were extended if needed. However, there was one case of a posterior cage removal failure. In that case, auto-iliac bone chips were grafted while leaving the cage (Fig. 2). One case underwent anterior cage removal and tricortical auto-iliac bone was grafted while preserving the posterior instrumentation and a hip spica cast was applied for 6 weeks. In the final analysis, all cases were cured of their respective infections. SII and DII were cured without implant removal. Two out of 10 O/SI that were treated conservatively ended up with nonunion. One of them showed retropulsion of the cage; however, the patient did not develop neurological symptoms and showed normalized laboratory findings. All revision cases (10/10) had bone union. Ultimately, 22 cases preserved their implants while 10 cases failed to do so. Risk factors of implant removal included the implant loosening and an ETD longer than 3 months in univariable analysis. However, in a multivariable logistic regression test, only ETD longer than 3 months was recognized as a risk factor (p=0.023, OR=32.592) (Table 2). Three months was determined by an ROC curve as the time that resulted in the widest area under the curve. Functional results as measured by ODI were improved from pre-treatment levels of 53.1% to 38.5% as a whole (p<0.001). SII improved from 47.3% to 33.8% (p=0.028), DII improved from 55.0% to 32.3% (p=0.043), and O/SI improved from 53.4% to 43.5% (p=0.003). The ODI of O/SI was lower, but it was not statistically significant (p=0.175). In the subgroup analysis of O/SI, there was no difference of ODI between the conservative and revision groups, which were 40.1% and 43.5%, respectively (p=0.344). There was a correlation between the ETD and final ODI while considering the confounding effect of preoperative ODI (r=0.374, p=0.038).
Discussion
The most prominent feature of SSI in PLIF was high incidence of O/SI. O/SI is known to have a long ETD. According to the definition of the CDC, O/SI is defined as an SSI which involves any part of anatomy which was opened and manipulated during an operation other than the incision itself [5]. The common features of SII and DII were not so different from other types of posterior instrumented surgery. However O/SI, i.e., spondylitis without incisional infection, has a range of different features from diagnosis to treatment. In the case of incisional infections, implant removal was not necessary. They were all diagnosed early and, consequently, local management began as soon as possible. Wound exploration and repeated irrigation was considered effective to prevent the infection's extension to deeper structures. Fortunately, there was no bone extension from incisional infections. Many authors have recommended the retention of implants in acute infections [678910]. However, in other studies, implant removal was frequently requested in DII [11121314]. In particular, late onset infections and Propionibacterium acne (PA) infections were found to be risk factors [13]. There was no late onset infection in the incisional infections in our cases. This is a possible reason why we were able to preserve all implants in the incisional infections. O/SI was not easily diagnosed because of its vague symptoms and an absence of local findings. Therefore, the ETD was further delayed after the true onset of infection in those cases. The O/SI almost always began from the interbody space as a spondylitis around the cages and grafted bone. It was difficult to presume that bacteria contaminated the interbody space only. Rather, it would be more plausible to presume that contaminated bacteria located in the interbody space were not easily removed by irrigation and adhered to disc remnants or foreign materials, and they gradually developed a late infection. If the contaminated bacteria were highly virulent, it is presumed that a more aggressive and acute onset infection would develop. In our cases, half of them did not undergo microbiological exams because they were managed conservatively. Intravenous antibiotics were started when laboratory and clinical manifestations strongly suggested infection. Cefolactam (Samjin Pharm, Seoul, Korea) that was comprised of cefoperazone and sulbactam was used as the intravenous antibiotic. Antibiotics were switched once the causative microorganism was determined from the sensitivity test. Among the 10 cases which underwent revision surgeries, there were no highly virulent microorganisms. Four cases showed no growth. There have been many studies that noted disc space infections after discectomy by anaerobic bacteria, especially PA [1516171819], and the late infection in instrumented spinal surgeries by PA [132021]. Disc space contamination by PA has been proven through other studies [2223]. We did not perform anaerobic culturing at first and did perform it later on. PA was not identified in any case; however, some of the cases might have been PA infections. The remaining cases were also not highly virulent infections. At first, we could not appropriately diagnose O/SI. After we became aware of its clinical manifestations, the ETD was shortened. Furthermore, we realized that conservative treatment was possible if an early diagnosis was made. Maruo and Berven [13] also noted that a late infection, in other words, late diagnosis, was a risk factor for treatment failure. The preservation of implants seriously matters in O/SI because cage removal is technically difficult [12]. Furthermore the index segment would lose stability entirely and neurological symptoms could develop after implant removal. If staged operations were performed, patients had to stay on bed rest during the interval. That is why we could not prevent performing POSSR. As far as we have researched, there is no agreement for the treatment for infections such as O/SI. Carmouche and Molinari [11] tried to preserve the cages but ultimately ended up removing the cages and achieved spinal fusion by posterolatral bone grafts. Ha and Kim [12] concluded that all implants should be removed to counter any spondylitis around the cages and that the anterior approach was feasible to remove them. Sierra-Hoffman et al. [14] and Hedequist et el. [24] determined that, in cases caught early, the implants could be preserved, but that late cases necessitated implant removal. There are many presumptive risk factors of implant removal. However, an ETD longer than 3 months was the only independent risk factor in our study. All revision cases had implant loosening. In an image test; however, two of them appeared not having loosening. For that reason, radiological implant loosening was not counted as an independent risk factor. Therefore, a keen suspicion is the first and most important step for the successful diagnosis of an SSI, which is directly related to successful treatment. In revision surgeries, all screws and cages were loosened and grafted bone chips were already sequestrated. Cage removal is a demanding procedure, but it is not impossible. Before cage removal, all screws and rods were removed and widened holes were charged with fresh frozen allograft bone chips and bigger screws were inserted. The interbody space was distracted to make a space for the cage removal. However, we failed to remove the cage in one case. In that case, we displaced it to the opposite side and grafted an auto-iliac bone. At the final assessment, the patient achieved solid interbody fusion and the cage was embedded in the bone mass. There have been many reports stating that titanium cages can be used in the surgical treatment of spondylitis [25262728]. We are unsure if titanium cages are safe to use in spondylitis or not. Furthermore, the titanium cage would be different from the initially applied cage because it was presumed to be covered by a biofilm of microorganisms. Though our case cannot be generalized, the meticulous debridement and copious irrigation with a pulsatile irrigator of the interbody space and auto-iliac bone grafts were considered more important than the titanium cage removal itself. While all revision cases achieved interbody fusion, two cases of spondylitis that underwent conservative treatment resulted in a nonunion state. One patient was asymptomatic, while the other had discomfort and back pain aggravated by motion but refused to receive a revision. If the causative bacteria were highly virulent, the treatment options would have been different. Tokuhashi et al. [29] reported the successful treatment of spondylitis around cages without surgical intervention, though there was already an epidural abscess and explained it was possible because the causative bacteria were lowly virulent. POSSR might have been dangerous if the SSI was caused by highly virulent bacteria. POSSR has several drawbacks. Posterior interbody debridement might be incomplete and bicortical auto-iliac bone from the posterior iliac crest is not as strong as tricortical bone from the anterior iliac crest. It has, however, many advantages. Through a posterior approach, all implants and infected tissues in the epidural and interbody spaces could be removed. Furthermore, stability could be attained under the same anesthesia and without positional changes, minimizing neurological injury and reducing the patient's inconvenience which would result from a longer duration bed rest. At first, we thought the widened pedicle holes should be charged with auto-iliac bone. But the amount of auto-iliac bone was not enough to cover both the interbody space and the pedicle holes. Furthermore, it did not have sufficient structural hardness, due to osteoporosis. So, we cautiously used fresh frozen allogeneic bone from the bone bank of author's institute. Fortunately, there have been no adverse effects so far. Functional results were improved after treatment of the SSIs in general. Though functional improvements were not as strong in O/SI, it did not reach statistical significance. O/SI was influenced by ETD. We could say SII and DII had better functional results than O/SI; however, the early diagnosed O/SI was not inferior to SII or DII. Therefore, an early diagnosis was the key to averting implant removal and attaining a better functional result. There were several limitations in our study. As a general limitation of observational studies, the results of our case series could not represent every specific situation. In particular, our cases were mainly caused by low virulent microorganisms. A more precautious strategy would be necessary for the highly virulent aggressive SSI.
Conclusions
The incidence of SSI in PLIF was 1.6%. O/SI was the most common type. In SII and DII, implant removal was not necessary and early wound exploration and repeated irrigation followed by secondary closure was an effective treatment regimen. In O/SI, however, 50% of patients needed implant removal, though the early diagnosed cases could be treated conservatively. ETDs longer than 3 months conspicuously increased the risk of implant removal. POSSR, from implant removal to re-implantation, was effective for the spondylitis around interbody cages. It minimized patients' discomfort by avoiding a staged operation or dual approaches. Functional results were improved as compared to the pre-treatment state, but were not distinguishable from type to type. However, a long ETD made it worse. Therefore, a keen suspicion to detect vague clues and an early diagnosis followed by prompt and appropriate treatments were the most important in treating SSI in PLIF.