Introduction
Patients with adult spinal deformity (ASD), especially the elderly patients, experience several symptoms that seriously compromise their quality of life. Several studies have proposed target values for corrective surgery, and many surgeons perform corrective surgery using a long construct and various osteotomies to achieve optimal alignment in patients with a severe deformity [1,2]. However, corrective surgery for ASD patients remains challenging owing to many perioperative complications and future reoperations [3,4].
Rod breakage is the most serious implant-related complication that leads to severe back pain, loss of correction, and need for revision surgery in most cases [5,6]. We previously reported 54 cases of rod fracture (18%) after corrective fusion surgery in 304 ASD patients, 36 (66.7%) of whom required revision surgery [7]. We have observed several cases of rod fracture; therefore, we decided to attach additional rods to the two main rods to prevent rod fracture after ASD surgery with pelvic fixation. Several authors also recommend multi-rod constructs for the prevention of rod fracture and pseudarthrosis [8-10]. However, the stronger construct seems to concentrate the mechanical force on the junctional segments, and limited information is available regarding the clinical effects of long-segment fusion using a multi-rod construct on such junctional segments.
We previously reported a relatively high incidence (28%) of iliac screw loosening after ASD surgery, with at least 2 years of follow-up [11]. Moreover, patients with iliac screw loosening showed worse sagittal alignment and clinical outcome than those without screw loosening. Thus, iliac screw loosening may be an indicator of distal junctional instability and poor prognosis.
To the best of our knowledge, this is the first study to compare the incidence of iliac screw loosening between patients who underwent surgery with a standard two-rod construct and those with a multi-rod construct; we also examined the influence of iliac screw loosening on clinical and radiographic outcomes after ASD surgery.
Materials and Methods
1. Patient enrollment
All study participants provided informed consent, and the study design was approved by the appropriate ethics review boards in Hamamatsu University School of Medicine (research approval no., 14-306). ASD patients who underwent corrective fusion surgery using long constructs from the lower thoracic spine (T7–12) to the pelvis with bilateral iliac screws from April 2011 to February 2017 at our department with at least 1 year of follow-up were enrolled. We excluded patients who required more than two iliac screws and those with upper thoracic fusion or iliac screw misplacement that could influence iliac screw loosening.
2. Surgical procedure for iliac screw insertion
Surgeries were performed by one of six board-certified spine surgeons. We inserted iliac screws freehand from the posterior superior iliac spine (PSIS) without separate skin incision. The PSIS was exposed via periosteal dissection of the soft tissue, and the tips of the PSIS were removed using a rongeur. A blunt probe was gently and carefully inserted into the cancellous bone of the ilium, taking care to avoid penetration of the table. Lateral and sagittal angles of the screw were determined using preoperative computed tomography (CT) and intraoperative lateral spinopelvic radiography, respectively. A screw (7.5 mm in diameter and 75–80 mm in length) was adopted and commonly used. The screw was inserted to considerable depth to prevent a prominent screw head. All the patients underwent posterior bone grafting using local bone, with or without L5/S interbody fusion.
3. Rod construct
We attempted to place additional rods for posterior corrective fusion in 2013 after observing several cases of rod fractures in patients with the use of conventional two-rod constructs. The period from 2013–2015 was a transitional period, and the surgeon determined the type of rod construct after considering several factors, such as spinal stability, closure of the osteotomy site, bone fragility, and their own experience with rod fracture. From 2016, multi-rod constructs were used in all cases. Additional rods were constructed on the inside from one or both sides of a conventional rod using three or four side-by-side connectors. A commercially pure titanium rod (φ6.0 mm or φ6.35 mm) was mainly used for less mechanical stress and prevention of screw pulling out.
4. Clinical assessment
The following demographic and clinical data were extracted from medical records for retrospective analysis: age, sex, and bone mineral density (BMD) of the proximal femur assessed using dual-energy X-ray absorptiometry. Furthermore, the following operative data were extracted: upper instrumented vertebra (UIV), presence or absence of high-grade osteotomy (pedicle subtraction osteotomy [PSO] or vertebral column resection [VCR]), and enforcement of L5/S interbody fusion. The Oswestry Disability Index (ODI) score was assessed preoperatively and at the 1-year follow-up to determine the health-related quality of life.
5. Radiographic assessment
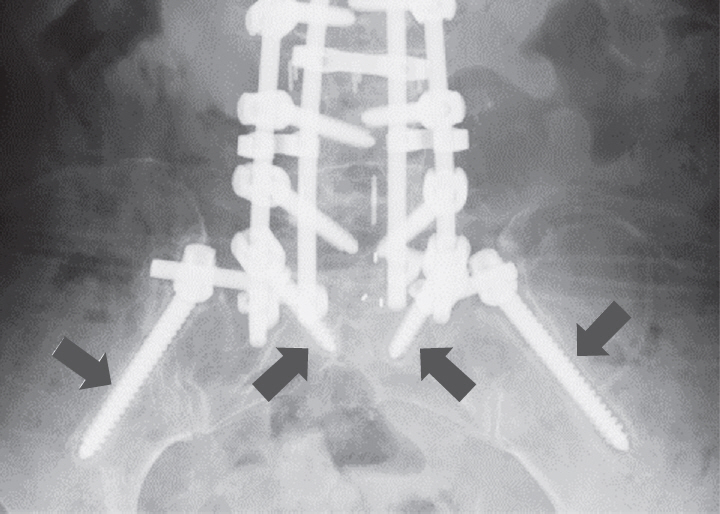
Iliac, S1, and UIV screw loosening was assessed using anteroposterior radiography at the 1-year follow-up. Screw loosening was defined as a circumferential radiolucent area ≥1 mm around the screw observed by more than two observers (Fig. 1) [12,13]. In case of any ambiguity, CT was used for determination of loosening. The incidence of rod fracture and proximal junctional kyphosis (PJK) was also assessed during the postoperative follow-up period. The following radiographic parameters were measured using whole-spine radiography preoperatively, early postoperatively, and 1-year postoperatively: sagittal vertical axis (SVA), T1-pelvic angle (TPA), pelvic tilt (PT), pelvic incidence (PI), L1–S1 lumbar lordosis (LL), and proximal junctional angle (PJA). Radiographic views were obtained with 1.5 m between the X-ray tube and the radiograph. A standing posture for lateral whole-spine radiography was standardized: subjects were asked to relax their heads while looking straight ahead, without pulling in the chin, and with their hands on their clavicle.
6. Statistical analyses
Patients were divided into two groups as per the type of rod construct used for them: conventional two-rod or multi-rod (three or four rods) (Fig. 2). Age, sex, BMD, fusion level, rate of high-grade osteotomy, rate of L5/S interbody fusion, rate of screw loosening (UIV, S1, and iliac), rate of rod fracture, spinopelvic parameters (SVA, PT, PI, LL, and PJA), and ODI score of the two groups were compared. Moreover, patients in the multi-rod group were divided into two groups as per the presence or absence of iliac screw loosening and compared. Student t-test, Mann–Whitney U-test, chi-square test, and Fisher’s exact test were used to evaluate the differences between the groups. Moreover, factors that contributed to iliac screw loosening were calculated using logistic regression with age, sex, BMD, fusion level, presence of high-grade osteotomy, enforcement of L5/S interbody fusion, and rod number (two-rod or multi-rod) as explanatory variables, and the presence of iliac screw loosening as a free variable. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA).
Results
Among 460 eligible patients identified over the study period, 106 (24 men and 82 women; age range, 37–83 years; mean age, 68 years) were included. The mean follow-up period was 42 months (range, 13–83 months). Fifty-five patients underwent corrective fusion surgery using a conventional two-rod construct, while 51 patients underwent surgery with a multi-rod construct (three rods in 16 patients, four rods in 35 patients). BMD measurement was performed in 66 cases, with a mean T score at the femoral neck of -1.5±1.1. High-grade osteotomies were performed in 38 patients (PSO in 23 patients, VCR in 15 patients) [14]. The mean number of fused levels was 8.5 segments, with a UIV of T7 in four patients, T8 in 10 patients, T9 in 27 patients, T10 in 63 patients, T11 in one patient, and T12 in one patient. All the patients underwent sacroiliac fusion using bilateral S1 and iliac screws. L5/S interbody fusion was performed in 83 patients (78%). Iliac and UIV screw loosening was observed in 24 patients (21%) and 35 patients (33%), respectively. Among the 24 patients with iliac screw loosening, seven (7%) also showed S1 screw loosening. During the follow-up, rod fracture and PJK occurred in 24 patients (21%) and 27 patients (25%), respectively (Table 1). Iliac screw removal was only required for one patient because of a prominent screw head, while none required revision surgery for L5/S pseudarthrosis. Sixteen patients underwent revision surgery; three because of PJK and 13 because of rod breakage.
Comparing the two-rod and multi-rod groups, the incidence of iliac screw loosening (37% versus 9%, p<0.001) and UIV screw loosening (43% versus 23%, p=0.033) was significantly higher in the multi-rod group. In contrast, the incidence of rod fracture was significantly lower in the multi-rod group (10% versus 35%, p=0.002), while no intergroup differences were observed in terms of age, sex, BMD, fusion level, high-grade osteotomy, L5/S interbody fusion, or PJK (Table 1). Multiple logistic regression analysis indicated that BMD and multi-rod construct considerably affected the incidence of iliac screw loosening (odds ratio [OR], 2.6; 95% confidence interval [CI], 1.2–5.9; p=0.019; and OR, 33.6; 95% CI, 3.4–329.3; p=0.003, respectively), while age, sex, fusion level, high-grade osteotomies, and L5/S interbody fusion were not statistically associated with iliac screw loosening (Table 2).
Regarding spinopelvic parameters and ODI score, although these values were significantly improved postoperatively, no significant differences were observed between the two-rod and multi-rod groups at any time point (Table 3).
When patients in the multi-rod group were divided as per the presence of iliac screw loosening, those with screw loosening showed a lower BMD (T score: -1.9 versus -1.0, p=0.005), higher rate of a four-rod construct (44% versus 11%, p=0.015), UIV screw loosening (68% versus 28%, p=0.005), and S1 screw loosening (26% versus 0%, p=0.005); however, there were no significant differences in the age, sex, fusion level, high-grade osteotomy, L5/S interbody fusion, rod fracture, or PJK (Table 4). Furthermore, no significant intergroup differences were observed in the spinopelvic parameters or ODI at any time point (Table 5). However, when the patient with and without S1 screw loosening were compared, those with screw loosening had significantly worse SVA and TPA at 1-year postoperatively (Table 6).
Discussion
To our knowledge, this is the first study to compare the incidence of iliac screw loosening between patients who underwent surgery with a standard two-rod construct versus those who underwent surgery with a multi-rod construct and evaluate the influence of iliac screw loosening on the clinical and radiographic outcomes following ASD surgery. Our findings revealed that the use of a multi-rod construct for long-segment fusion surgery is associated with a higher incidence of junctional screw loosening, especially in patients with osteoporosis. Furthermore, iliac screw loosening did not affect sagittal alignment or clinical outcomes in the short term.
In ASD patients, aggravation of clinical symptoms is specifically associated with loss of sagittal alignment. Thus, a principal goal of corrective surgery is the restoration of proper sagittal spinopelvic alignment using rigid instrumented fixation [1,15,16]. In patients with severe rigid spinal deformity, several osteotomies and a long construct are useful for the restoration of spinal alignment and improvement in clinical outcomes. However, these procedures and greater correction of spinal alignment cause mechanical stress on the construct and involve the risk of rod fracture [17]. Multi-rod constructs are reportedly useful in preventing rod fracture [8-10]. Kelly et al. [10] compared a four-rod and a conventional two-rod construct for lumbopelvic fixation in a biomechanical study. They revealed that the four-rod construct provided significantly greater fixation stability than the conventional two-rod construct. Clinically, Hyun et al. [8] compared the radiographic outcomes using a standard two-rod and a multi-rod construct across three-column osteotomy sites in a matched cohort. The use of a multi-rod construct provided increased stability and was significantly more efficient in preventing implant failure and symptomatic pseudarthrosis as compared to a standard two-rod construct. In our study, consistent with previous reports, the multi-rod group showed a significantly lower incidence of rod fracture than the two-rod group. In contrast, the multi-rod group showed a higher incidence of iliac screw loosening although there were no intergroup differences in the reported risk factors for iliac screw loosening: BMD, fusion level, high-grade osteotomy, L5/S interbody fusion, and spinopelvic parameters [11,18,19] (Tables 1, 3). Moreover, using multiple regression analysis, we found that the use of the multi-rod construct had the greatest effect on iliac screw loosening (Table 2). These results indicate that stronger fixation by a multi-rod construct can cause concentration of mechanical stress on the distal junctional segments. Considering that no revision surgery was required for iliac screw loosening and that there is a high revision rate (54%) for rod fracture in patients with corrective fusion using iliac screw fixation, it is preferable to use multi-rod constructs for reducing the need for revision surgery. Moreover, for the proximal junctional segments, the multi-rod group had a higher incidence of UIV screw loosening, although no intergroup differences were observed in PJK or PJA. This suggests that the multi-rod construct did not contribute to PJK development. The causes of PJK are not fully understood and are reported to be multifactorial [20]; further, UIV screw loosening may not be a risk factor.
Patients with screw loosening had a significantly lower BMD, higher rate of a four-rod construct, and higher prevalence of UIV and S1 screw loosening (Table 4). Many of our elderly ASD patients also had osteoporosis. Implant-related complications and adjacent vertebral fracture frequently occur in osteoporosis patients [21,22]. Osteoporosis has also been reported as a risk factor for pedicle screw loosening [18,19]. In a biomechanical study, Weiser et al. [23] showed that pedicle screw stability is highly correlated with BMD. Therefore, patients with severe osteoporosis are at a higher risk of screw loosening when they undergo corrective fusion surgery using a multi-rod construct.
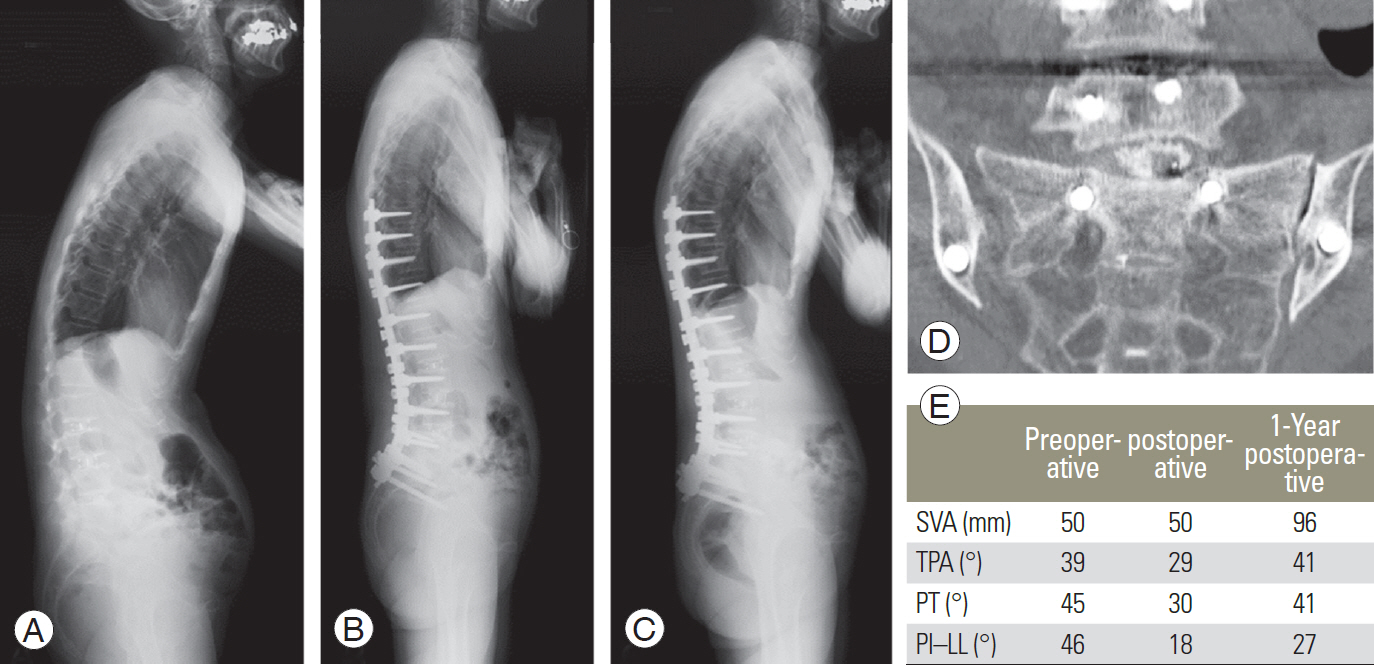
Regarding screw loosening, some authors have reported that screws with radiolucent areas are indicators of instability and influence the achievement of solid fusion [12,13]. However, in terms of iliac screws, screw loosening itself does not necessary indicate instability of the lumbosacral junction because the sacroiliac joint exists between the iliac and S1 screws. In fact, we found no significant influence of iliac screw loosening on postoperative spinopelvic parameters or the ODI score in the present study (Table 5). Previously, we investigated iliac screw loosening after corrective fusion surgery in 72 patients to find that those with iliac screw loosening for >2 years had worse sagittal alignment and ODI score than those without iliac screw loosening [11]. However, the short follow-up period (1 year) and relatively small number of study subjects in the present study may be the reason for the different results. However, patients with both, iliac and S1 screw loosening had significantly worse SVA and TPA at 1 year postoperatively, indicating high instability of the lumbosacral junction and possible pseudarthrosis (Figs. 3, 4).
In order to lower the risk of screw loosening, surgeons should consider treatment of perioperative osteoporosis. Ohtori et al. [19] reported that teriparatide therapy significantly decreased the rate of pedicle screw loosening in osteoporosis patients. Moreover, to improve the anchoring strength of iliac screws, dual-screw placement or polymethylmethacrylate augmentation should be considered in osteoporosis patients [24,25]. Recently, the S2 alar iliac (S2AI) screw that can provide durable distal fixation with a low-profile, in-line technique, has been widely used, instead of a conventional iliac screw, for rigid lumbosacral fixation [26]. Screw head prominence is a major complication of iliac screws and frequently leads to severe pain, requiring screw removal. The incidence of iliac screw removal due to screw head prominence is reported to range from 6.1% to 34% [27-29]. However, in this study, screw removal was only required in one case (0.9%) for a prominent screw head, indicating a relatively low rate. We can prevent screw head prominence by attempting to place the iliac screw deep enough to hide the screw head below the iliac crest. However, screw breakage has been reported with the S2AI screw [30]. The S2AI screw penetrates the sacroiliac joint; therefore, mechanical stress might be concentrated on the screw. Once screw breakage occurs, revision surgery becomes challenging. Thus, we prefer to use iliac screws rather than S2AI screw.
This study has certain limitations. First, this study was designed retrospectively. Therefore, the follow-up period was different between the two-rod and multi-rod groups. Lertudomphonwanit et al. [6] investigated 526 patients who underwent corrective fusion surgery for ASD and reported that rod fracture occurred in 97 patients (18.4%). Among them, approximately 50% of rod fractures occurred more than 3 years postoperatively. Moreover, the long-term effect of iliac screw loosening on the distal junction is relatively unknown. Therefore, a long-term follow-up study is necessary on patients with a multi-rod construct. Second, our study did not perform bone union assessment. It is unclear whether iliac screw loosening was related to pseudarthrosis progression because we could not directly assess the presence of pseudarthrosis. However, five cases with S1 screw loosening involved significant deterioration of the SVA during the follow-up period, while iliac screw loosening alone did not affect postoperative alignment. These results suggest that S1 and iliac screw loosening together indicate distal junctional failure. Therefore, patients with iliac screw loosening should be provided treatment with care, with a special focus on the appearance of S1 screw loosening.
Conclusions
The use of a multi-rod construct for long-segment fusion surgery was associated with a higher incidence of iliac screw loosening than the use of a conventional two-rod construct, especially in patients with osteoporosis. Iliac screw loosening did not affect sagittal alignment or clinical outcomes in the short term.