Introduction
The National Inpatient Sample database reported an increased long construct spine fusion by 141% from 2004 to 2015, while the corresponding figure was massively driven by 460% for individuals aged 65–84 years [1]. Fusion at L5 or the pelvis for the long construct spine fusion surgeries remains debatable. Several studies recommended spinopelvic fixation to achieve satisfactory stability, which could decrease the incidence of rod fracture, pseudarthroses (L5–S1), or neurological deficits [2–4]. Additionally, spinopelvic fixation is essential for achieving proper sagittal and coronal alignment [3,5]. Several spinopelvic fixation strategies are available, among which iliac screws (IS), and S2 alar-iliac (S2AI) screws were widely used [5–9]. Complications related to S2AI and IS should not be ignored, such as the caudal screw loosening, despite the favorable outcomes reported with the use of S2AI screws and IS in adult spinal deformity surgery [10].
The caudal screw loosening (S2AI or IS) demonstrated the failure of the long construct spine fusion, indicating potential pseudarthrosis. The rate of S2AI or IS loosening after long construct spine fusion varied among different reports [10–14]. Banno et al. [10] reported that IS loosening rate was 27.8%, and IS loosening group demonstrated a higher upper thoracic fusion rate (>T6), a lower L5/S1 inter-body fusion rate, a higher misplacement rate, and a higher insufficient correction rate (pelvic incidence minus lumbar lordosis [PI–LL] of >10°). Marie-Hardy et al. [6] reported several risk factors, including osteoporosis, sagittal imbalance, and rigid material. Multiple factors lead to screw loosening, including older age, larger pelvic incidence (PI), revision surgery, failure to restore lumbar lordosis, and insufficient sacropelvic fixation [10]. The risk factors of S2AI and IS loosening are debatable although researchers focusing on S2AI and IS loosening are increasing, and some essential factors are not properly considered. Therefore, the current meta-analysis investigated the influencing factors of S2AI screw and IS loosening.
Materials and Methods
1. Data sources and searches
PubMed, Web of Science, and Embase databases were searched to get eligible articles focusing on IS or S2AI screws loosening, on October 14, 2022. The following was the searching strategy: screw AND loosening AND (iliac OR S2AI).
2. Inclusion and exclusion criteria
Inclusion criteria are as follows: (1) case-control study or cohort study; (2) include patients with adult spinal deformity; (3) >4 fusion segments; (4) IS or S2AI screws were inserted; and (5) English literature. Any dispute was resolved through discussion within the study group. The current meta-analysis followed the standard Preferred Reporting Items for Systematic Reviews and Meta-Analyses [15].
3. Data collection
Two reviewers extracted and checked the following information: (1) the first author, publication date, study design, and follow-up time; (2) age at surgery, gender, and preoperative T-score; (3) preoperative and postoperative radiographic parameters: thoracic kyphosis (TK), lumbar lordosis (LL), pelvic tilt (PT), PI, PI–LL, sagittal vertical axis (SVA), T1 pelvic angle (TPA); and (4) surgery-related information: the number of fusion segments, rod breakage, and proximal junctional kyphosis (PJK).
5. Sensitivity analysis
The study further assessed whether the single paper exerted excessive weight on the overall results by removing each article in sequence.
6. Statistical analysis
Binary variables used odds ratio (OR) and 95% confidence interval (95% CI) to describe the risk factors of IS or S2AI loosening, while the weight mean difference (WMD) and 95% CI were used to describe the difference of continuous variables. p-values of <0.05 indicated statistical significance. The random effect model would be used when I2 is ≥50%, otherwise, the fixed effect model was employed. The Review Manager ver. 5.3 (RevMan; Cochrane, London, UK) pooled the statistics.
Results
1. Paper selection and characteristics
We retrieved 672 articles, of which 14 met the inclusion criteria [2,8–14,16–21]. Three studies focused on S2AI [11,13,21], six on IS [8–10,12,14,18], and five on S2AI and IS [2,16,17,19,20]. The flow chart in Fig. 1 shows the selection and exclusion process. This meta-analysis included 1,138 ASD cases (S2AI=286, IS=852), and 243 cases (S2AI=83, IS=160, 21.35%) were included in the loosening group. This study used the Newcastle-Ottawa quality assessment scale to assess every included paper (Table 1).
2. Meta-analysis results
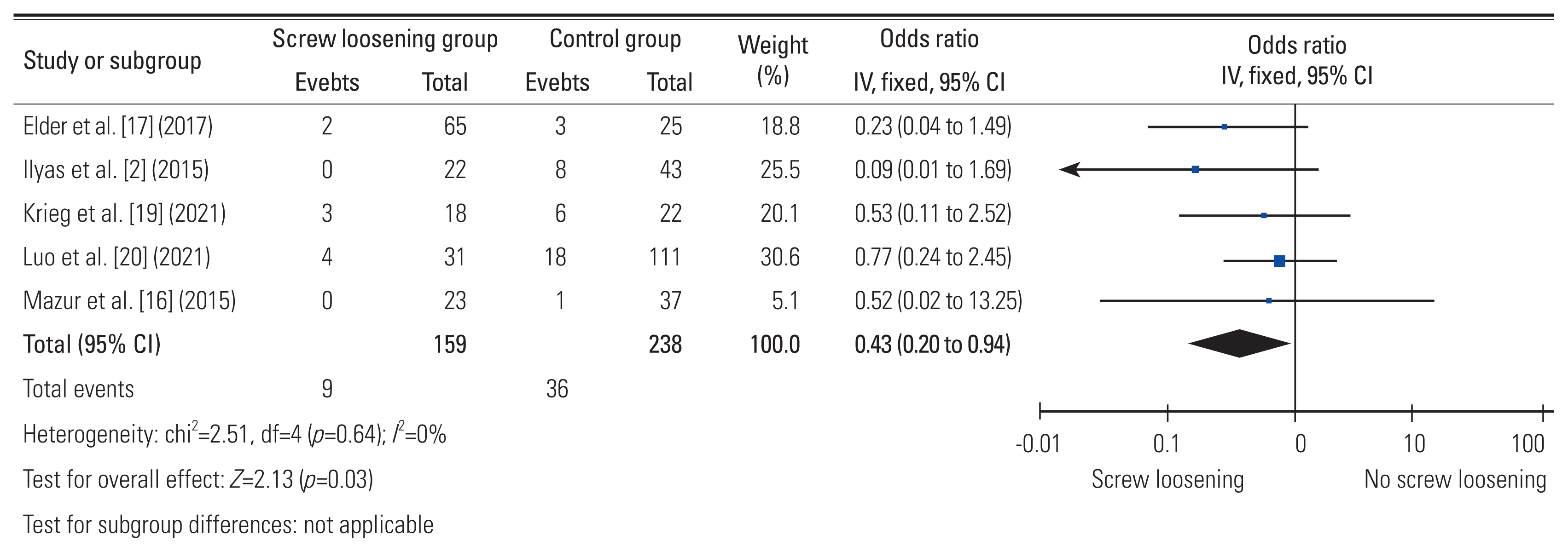
The loosening group was older than the control group (WMD, 2.17; 95% CI, 0.48–3.87; p=0.01). The S2AI could prevent screw loosening (OR, 0.43; 95% CI, 0.20–0.94; p=0.03) (Fig. 2). However, gender distribution (p=0.36), the number of fusion levels (p=0.24), rod breakage (p=0.97), T-score (p=0.10), and PJK (p=0.75) demonstrated no difference.
Preoperatively, only PI in the loosening group was higher (WMD, 5.08; 95% CI, 2.71–7.45; p<0.01) (Fig. 3), while preoperative TK (p=0.09), preoperative LL (p=0.69), preoperative PT (p=0.31), preoperative PI–LL (p=0.35), preoperative SVA (p=0.27), and preoperative TPA (p=0.10) demonstrated no significant difference.
PI–LL (WMD, 6.05; 95% CI, 0.96–11.14; p=0.02), PT (WMD, 4.12; 95% CI, 0.99–7.26; p=0.01), TPA (WMD, 4.72; 95% CI, 2.35–7.09; p<0.01), and SVA (WMD, 13.35; 95% CI, 2.83–3.87; p=0.001) were higher in the screw loosening group immediately postoperatively. However, TK (p=0.24) and LL (p=0.44) demonstrated no significant difference.
TPA (WMD, 8.38; 95% CI, 3.30–13.47; p<0.01), PT (WMD, 6.01; 95% CI, 1.47–10.55; p=0.01), and SVA (WMD, 23.13; 95% CI, 12.06–34.21; p<0.01) were higher in screw loosening group at final follow-up. However, PI–LL (p=0.17) demonstrated no significant difference. Table 2 demonstrated the comparison details in the aforementioned parameters between groups.
Discussion
1. The incidence of S2AI screws or IS loosening for the long construct spine fusion
Several papers reported that the loosening rate was 20%–35%. Mazur et al. [16] reported the lowest incidence of screw loosening at 1.67% (1/60), while Nakashima et al. [11] reported the highest loosening rate at 51.74% in 35 adult patients with spinal deformity. The screw loosening rates varied from different studies due to the heterogeneity in diagnosis and study design [11,16]. The loosening rate was 21.35%, which was similar to the previous literature, among 1,138 ASD cases (S2AI=286, IS=852) included in the current study [8,10]. Therefore, we should never ignore IS or S2AI screws loosening after the long construct spine fusion.
2. Patient-related risk factors
Patient-related factors are important factors affecting the loosening. Previous studies did not show the difference in age between groups [10,12,13], but the current meta-analysis detected that the loosening group was older than the control group. Elderly patients frequently have severe osteopenia and paravertebral muscle degeneration, which may increase the screw loosening rate [22,23]. Previously, Iijima et al. [13] reported a higher obesity rate in the S2AI screw loosening group. Banno et al. [12] also detected a lower T-score in the IS loosening group. the S2AI screw loosening rate in patients with poorly-managed osteopenia could be as high as 33.6%, which might result from the screw crossing the empty cortical shell of the osteoporotic sacral alar [24].
This meta-analysis revealed no difference in gender distribution, which was consistent with the previous reports [13,14]. However, elderly female individuals are of higher susceptibility to osteoporosis, causing a higher screw loosening rate (S2AI or IS). Many studies aimed to assess the effect of body mass index on the loosening rate, but with no consistent results. Iijima et al. [13] reported a higher obesity rate in individuals with S2AI loosening than that with no loosening. However, the majority of the literature reported no difference between the screw loosening and the control group. However, being overweight always meant higher stress on the caudal construct, increased risk of osteoporosis, and poor clinical outcomes postoperatively [25]. Thus, weight control was recommended.
3. Radiographic-related risk factors
The three-dimensional spinal misalignment is the main reason for the long construct spine fusion with pelvic fixation. Preoperatively, the pooled PI was larger in the loosening group (WMD, 5.08; 95% CI, 2.71–7.45; p<0.01). Previously, Iijima et al. [13] also reported a higher PI in the S2AI loosening group (53.5±13.6 versus 44.8±7.6, p=0.04). However, TK, LL, PT, PI–LL, SVA, and TPA demonstrated no significant difference preoperatively. Therefore, a similar radiographic balance status was demonstrated between the screw loosening group and the control group preoperatively.
Immediately postoperatively, Iijima et al. [13] reported a higher SVA and PI–LL in the loosening group. Correspondingly, Banno et al. [10] reported a higher TPA, PT, and PI–LL in the screw loosening group. However, Kim et al. [14] and Banno et al. [12] revealed no significant difference in radiographic parameters immediately postoperatively. The current pooled results demonstrated a higher SVA, TPA, PI–LL, and PT, which meant the relative forward inclination of the trunk in the screw loosening group. The immediate postoperative PI–LL and SVA were highly associated with LL reconstruction in adults with spinal deformity. Therefore, a relatively larger LL should be achieved for patients with screw loosening.
The pooled results at the last follow-up detected the higher TPA (WMD, 8.38; 95% CI, 0.33–13.47; p<0.01) and SVA (WMD, 23.13; 95% CI, 12.06–34.21; p<0.01) in the screw loosening group. Banno et al. [10] also reported significantly higher TPA and SVA in the screw loosening group than that in the control group. Furthermore, the WMD related to SVA, TPA, and PT between groups demonstrated an increasing trend during the follow-up, indicating more serious trunk anteversion deterioration in the screw loosening group than that in the control group. In particular, sagittal balance deterioration might cause screw loosening. Additionally, the loosening group was older, and the trunk inclined forward with age. Therefore, the measures to block sagittal alignment deterioration could also prevent the caudal screw from loosening such as improving bone quality and avoiding excessive dissection of paravertebral muscles during operation [26].
4. Surgery-related risk factors
This study revealed a lower S2AI loosening rate than IS loosening rate (OR, 0.43; 95% CI, 0.20–0.94; p=0.03), which was consistent with a previous meta-analysis [24,27]. The IS loosening was 43% during a 5-year follow-up, with no S2AI loosening [27]. Similarly, Ilyas et al. [2] reported no S2AI loosening in both pediatric and adult individuals. More cortical screw purchases are achieved for S2AI screws that go through the sacroiliac joint, which theoretically causes a stronger pull-out resistance than IS screws. This may cause lower S2AI screw loosening rates compared with IS. Additionally, the connectors connecting the IS to the proximal lumbar construct can exert a moment arm on the proximal part of IS. Furthermore, Uotani et al. [21] reported that dual sacral-alar-iliac screws could significantly decrease the loosening rate compared with single sacral-alar-iliac screws. Ebata et al. [28] reported that the bilateral dual IS could significantly decrease the loosening rate than the common bilateral dual single iliac screw (9% versus 61%, p<0.001). Therefore, multiple pelvic screws (S2AI or IS) could be implanted to prevent screw loosening for appropriate cases. This study revealed no significant difference between groups concerning the number of fusion segments, which might result from the similar preoperative radiographic parameters between groups. The previous studies reported no difference, either [11,14]. Another influencing factor might be the multi-rod construct which increased the pull-out stress on the caudal screws. Banno et al. [12] reported the multi-rod construct as the main risk factor of IS loosening. Notably, L5/S1 pseudoarthrosis may cause the caudal screw to loosen. The multi-rod structure has better stability, which can prevent L5/S1 pseudoarthrosis and increase the caudal screw pull-out torque. Therefore, more research is needed to clarify the influence of multi-rod structure on the caudal loosening after pelvic fixation for patients with ASD. Reportedly, the longer and thicker IS were of higher pull-out resistance [29]. For each case, one ideal trajectory of screws guarantees the longer screws can be fixed without worrying about penetration. Previously, Banno et al. [10] proposed that IS direction should be consistent with the sacral slope, and then the screw would be inserted in a broad medullary cavity above the acetabulum. However, following the preset ideal trajectory is difficult while inserting the screw. Additionally, a misplaced screw is reported as one of the main reasons for the screw loosening in patients with ASD after spinopelvic fixation [10]. Other surgical strategies were also attempted to prevent screws from loosening after long construct fusion such as cement-augmented IS [30].
The most common instrumentation-related complications after long-segment spinal fixation comprised PJK and Rod fracture [4,31,32]. This study revealed no difference in PJK and rod breakage incidence between the screw loosening group and the control group, which was similar to previous reports [14,18]. Notably, the aforementioned complications were significantly associated with sagittal imbalance, indicating that the measures to prevent excessive anteversion of the trunk can simultaneously prevent PJK, rod breakage, and caudal screw loosening.
5. Shortcomings
The following shortcomings should be considered when referring to the pooled results although the meta-analysis systematically retrieved the relevant papers of S2AI or IS loosening after long construct spine fusion. Firstly, the current study failed to qualitatively assess the effect of screw misplacement on the loosening rate. The accuracy of the screw implantation position significantly affects the pull-out force of the screw. Secondly, the small sample sizes for the included literature might cause a high heterogeneity during synthesis. Thirdly, the caudal screw loosening generally causes pain and skin damage, which will inevitably cause poor clinical outcomes. This meta-analysis cannot pool statistics to analyze the impact of the caudal screw loosening on quality of life due to the lack of relevant original documents. Finally, only retrospective studies were reported, and prospective studies should elucidate the S2AI or IS loosening rate and the corresponding risk factors.
Conclusions
The S2AI screw or IS loosening was a common complication after long construct spinal fusion. Elderly individuals with osteoporosis were more susceptible to this complication. We might use S2AI screws to replace IS and reconstruct the lumbar lordosis and sagittal alignment properly to decrease the loosening rate. Measures to block sagittal alignment deterioration could also prevent the caudal screw from loosening.