Introduction
With the increasing number of spinal fusions performed [1-3], spine surgeons must be acquainted with a variety of fusion procedures. Lumbar interbody fusion has become a popular technique for treating spinal conditions such as spondylolisthesis, degenerative disc disease, recurrent disc herniation, pseudarthrosis and spinal deformity. Anterior lumbar interbody fusion provides direct access to the disc with potential improvement in fusion rate, but also carries the risk of injury to the iliac vessels, peritoneal content, ureteral and autonomic nervous system [4]. The traditional anterior retroperitoneal approach can also result in pain, muscular atony or herniation of the abdominal wall [5]. In an attempt to decrease the complications related to traditional exposures, various minimally invasive techniques have been developed to minimize the incidence of pain and abdominal wall atony or herniation after anterior lumbar interbody fusions [5-7]. Laparoscopic procedures have been proposed, but they are not widely used due to the steep learning curve, technical complexity, and limited visualization of the spine associated with the technique, and due to the absence of clear benefits over open procedures in terms of complication rates and outcomes [8-11]. However, miniopen techniques have gained wider acceptance among surgeons performing anterior lumbar interbody fusion because they allow direct access and visualization of intervertebral discs in order to achieve a more complete discectomy and theoretically a better fusion, while potentially decreasing morbidity [5-7,11].
Mayer [12] described a minimally invasive anterior approach to the lumbar spine through retroperitoneal access for L2-3 to L4-5 discs and transperitoneal access for L5-S1 disc, performed after prior posterior instrumentation and fusion. He presented performed his technique on 25 patients and obtained solid anterior fusion for all patients with minimal blood loss and no evidence of technique-related complications. The technique involves a muscle-splitting approach through a 4-cm oblique skin incision parallel to the fibers of the external oblique abdominal muscle that is extended to 6 cm if exposure of two discs is required. Kaiser et al. [11] reported their experience for single- or two-level anterior interbody fusion using the technique described by Mayer [12] on 51 patients, showing 3.9% and 17.6% of intraoperative and immediate postoperative complication rates, respectively. The intraoperative complications were: vascular laceration and dural tear. The immediate postoperative complications were: transient ileus, retroperitoneal hematoma, urinary tract infection, wound infection and worsened radiculopathy [11]. They also suggested that the mini-open technique is associated with a decreased incidence of retrograde ejaculation. Saraph et al. [13] compared the technique of Mayer [12] to the traditional anterior retroperitoneal approach for anterior interbody fusion. After a mean follow-up of 5.5 years, fusion and complication rates were similar between the two groups, but intraoperative blood loss, operation time and postoperative back pain were decreased with the mini-open technique. Interestingly, there were three patients with postoperative weakness of abdominal muscles in the group undergoing the traditional approach (n=33), as opposed to none in the mini-open group (n=23). Other miniopen anterior approaches to the lumbar spine have also been proposed [10,14], but these techniques involve opening the rectus sheath and mobilizing the rectus abdominis muscle with theoretically increased potential for abdominal wall morbidity. However, these techniques are useful when a more direct anterior approach is required.
In the past few years, the authors have used a minimally invasive retroperitoneal anterior approach similar to that of Mayer [12] for anterior lumbar interbody fusion. The technique is referred to by the authors as the oblique lumbar interbody fusion (OLIF). The purpose of this study was to report the use of this minimally invasive approach in 179 patients and to describe early complications and morbidities.
Materials and Methods
1. Cohort description
Medical and radiological charts of 179 consecutive patients undergoing posterior instrumentation and fusion followed by OLIF as a second stage operation were reviewed. All patients underwent OLIF between January 1st 2006 and June 30th 2009, and had prior posterior fusion using the Colorado 2 instrumentation system (Medtronic, Minneapolis, MN, USA). Included patient were treated for deformity, spondylolisthesis, disc disease or facet arthrosis, sagittal imbalance, revision surgery. No traumatic, tumorous nor spondylidiscitis cases were included in this study. Patients were excluded from the study if they had: 1) a thoracotomy, 2) a fusion through a transperitoneal L5-S1 approach, 3) a lumbar corpectomy, or 4) anterior instrumentation.
The authors decided on the following strategy. Posterior instrumentation was done with or without decompression to control the sagittal balance. Six weeks later, after the patient recovered, OLIF was done.
2. Minimally invasive oblique lumbar interbody fusion
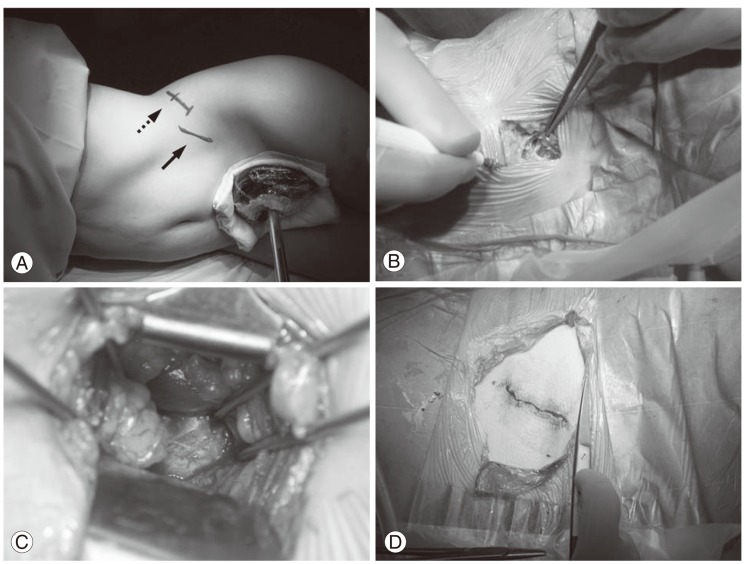
The patient was put in the lateral decubitus position and a radiograph was made in order to identify the intervertebral levels to approach. A 4-cm skin incision, centered on the spinal segment to expose, was made in the lateral abdominal region parallel to the fibers of the external oblique muscle (Fig. 1A). The incision was made perpendicular to the line joining the anterior superior iliac spine to the umbilicus at one third of the distance from the anterior superior iliac spine, similar to the McBurney incision. The approach was usually carried out from the left side but could also be performed from the right side, such as for right lumbar scoliosis. External oblique, internal oblique, and transverse abdominal muscles were then dissected along the direction of their fibers in this muscle-splitting approach (Fig. 1B). The retroperitoneal space was accessed by blunt dissection and the peritoneal content was mobilized anteriorly. The psoas muscle was identified and reclined posteriorly, while the sympathetic chain and the ureter were mobilized anteriorly. It was important to minimize the retraction of the psoas as much as possible in order to decrease postoperative pain-particularly cruralgia-secondary to injury of the lumbar plexus or psoas fibers. Four Steinman pins were used to expose the intervertebral disc without having to ligate segmental vessels (Fig. 1C). A window of only about 1cm in the annulus fibrosis was required anterolaterally to perform the discectomy and insert the cage. A radiograph was done to confirm the proper level before proceeding to interbody fusion. Segmental vessels usually did not need to be ligated unless the vertebral body needed to be exposed. At L4-5, the disc space could be obstructed by the iliolumbar vein, in which case it would need to be ligated.
Up to three discs could be approached using the same 4-cm incision through a "sliding window" technique without the need to extend the incision by taking advantage of the mobility of the abdominal wall. The described minimally invasive technique was well suited for exposure of the L2-3 and L4-5 discs, but rarely the L1-2 and L5-S1 discs. Exposure of L1-2 disc was limited by the chest cage and could be performed only in the presence of relatively horizontal and mobile floating ribs. As for L5-S1 disc, its access was limited by the iliac wing and by the need to mobilize iliac vessels.
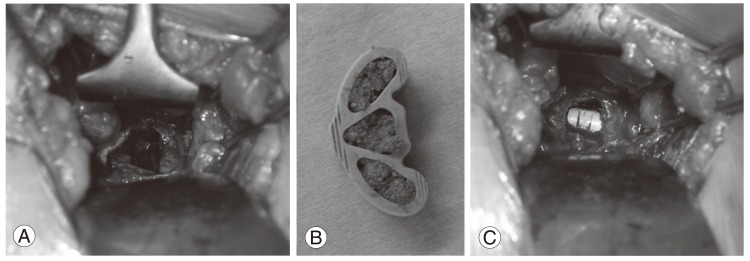
After discectomy (Fig. 2A), vertebral endplates were prepared in order to expose the subchondral bone. A banana-shaped polyetheretherketone cage (Boomerang, Medtronic, Inc., Minneapolis, MN, USA) was filled with a bone graft and/or a substitute (Fig. 2B) and inserted in a press fit fashion into the exposed disc spaces that remained open after the posterior procedure (Fig. 2C). Bone substitute was used as a graft to avoid morbidity of the donor site. If required, an autogeneous iliac graft could also be harvested from the same incision. Abdominal muscles planes were closed sequentially and the skin was closed using subcutaneous and subcuticular sutures (Fig. 1D). Although the procedures were performed without magnifying loupes or a surgical microscope, they could be used for improved vision. In addition, a headlight could be useful especially with overweight patients.
3. Data acquisition and analysis
Data acquisition included age, gender, weight, body mass index (BMI), side of the approach, levels approached, surgical blood loss, operation time, and length of hospital stay. Aborted procedures were also noted. All complications included in the medical charts were collected. Comparisons were performed using Student t tests with a level of significance of 0.05.
Results
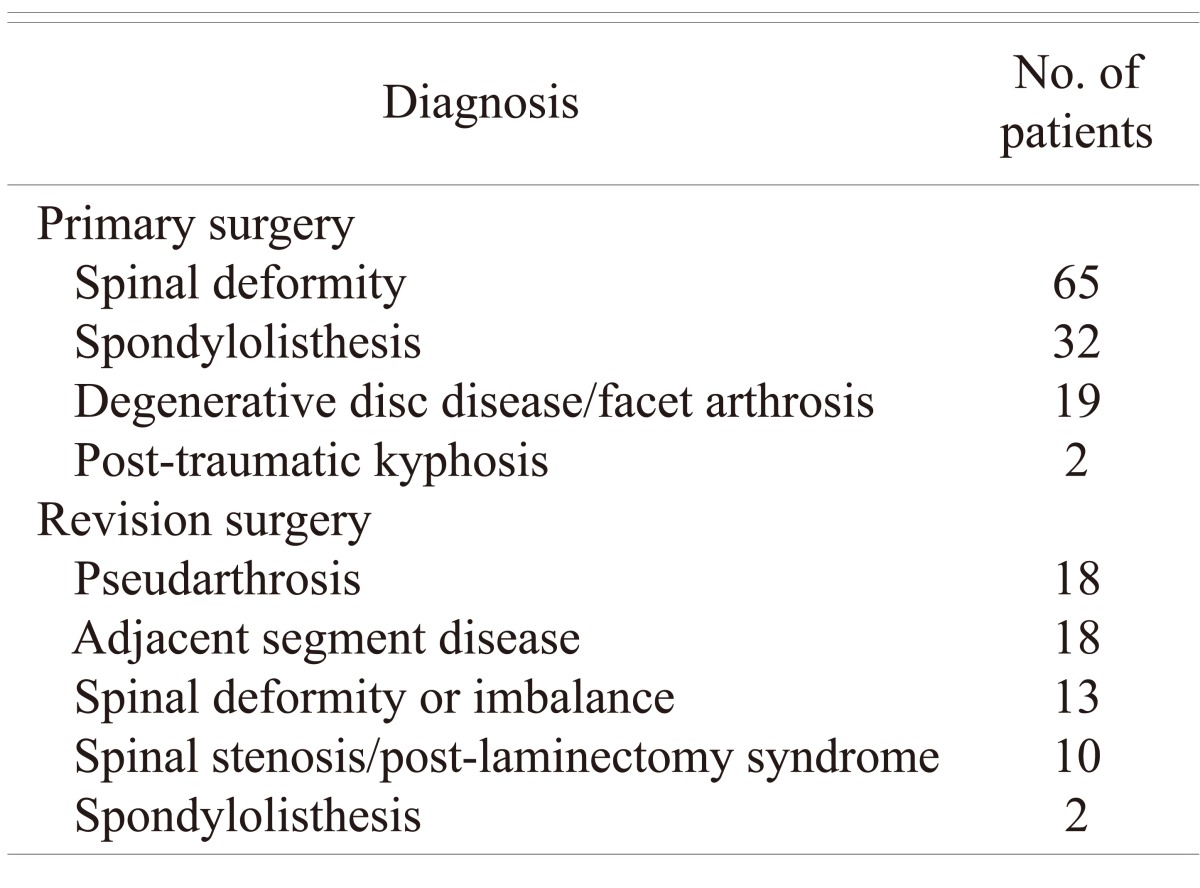
Patients were age 54.1 ┬▒ 10.6 years (range, 14.9 to 77.4 years). There were 148 females age 54.5 ┬▒ 11.0 years (range, 14.9 to 77.4 years) and 31 males age 52.2 ┬▒ 8.7 years (range, 27.2 to 67.7 years). There were 118 primary cases and 61 revision cases. There was no occurrence of revision after a previous anterior approach. Diagnosis at the time of surgery is shown in Table 1. Weight and BMI were respectively 67.1 ┬▒ 14.5 kg (range, 35 to 116 kg) and 24.8 ┬▒ 4.1 kg/m2 (range, 15.6 to 38.6 kg/m2). Follow-up was 0.94 ┬▒ 0.72 years on average and 17 patients had more than two years of follow-up.
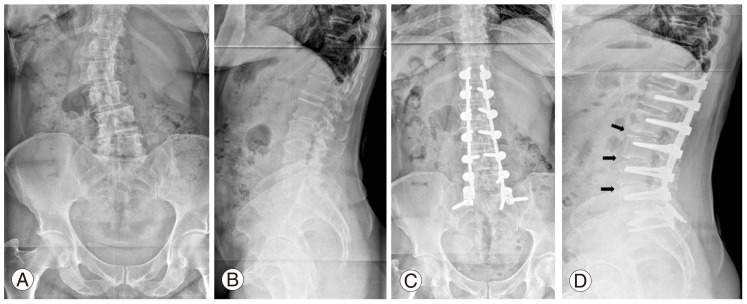
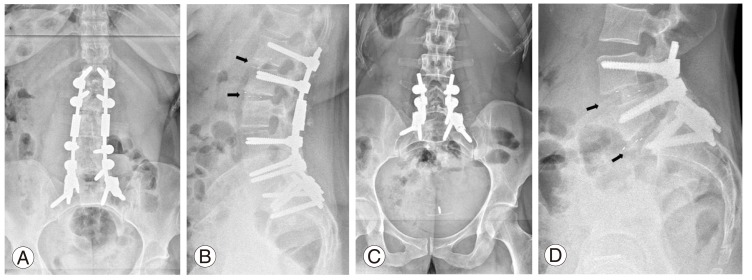
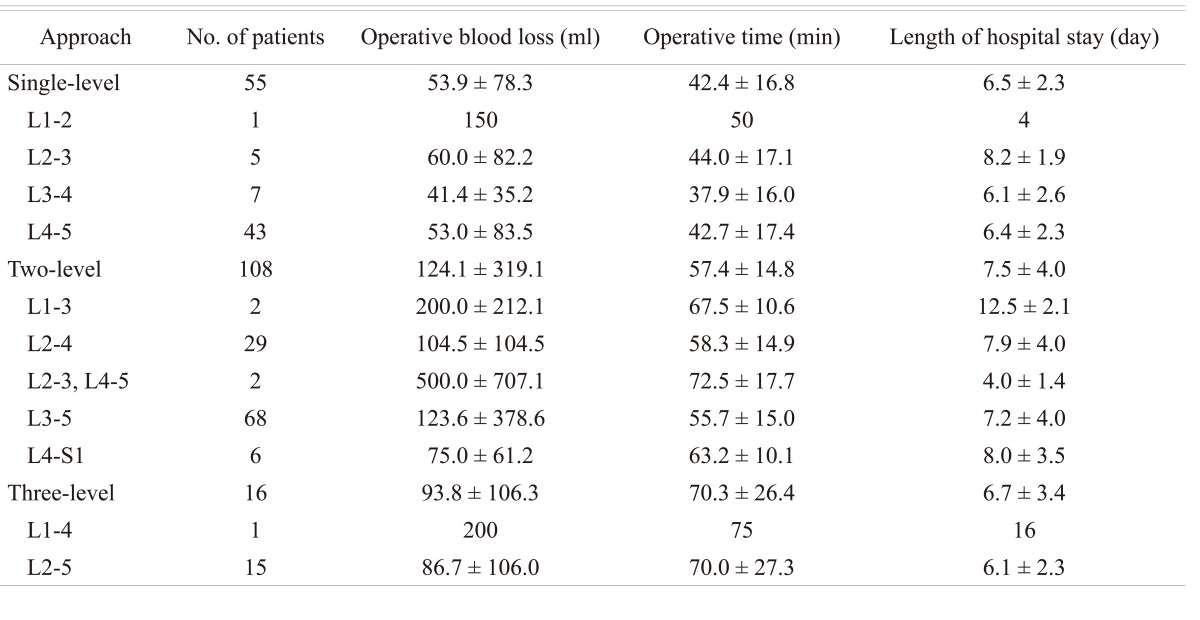
Four patients with scoliosis and one patient with L4-5 degenerative spondylolisthesis had a right-sided approach. Details of the levels approached with the respective operative blood loss, operation time and length of hospital stay are provided in Table 2. The procedure was performed at discs L1-2 in 4, L2-3 in 54, L3-4 in 120, L4-5 in 134, and L5-S1 in 6 patients. It was done at a single level for 56, two levels for 107, and three levels for 16 patients. Fig. 3 shows radiographs of a patient with a three-level OLIF at L2-5, while Fig. 4 shows two different patients with L1-3 and L4-S1 OLIF, demonstrating the potential use of the described technique for approaching L1-2 and L5-S1 levels, respectively.
In three patients, the procedure was aborted for one level. For the first patient, an L3-5 OLIF was planned but only L4-L5 was performed. Surgery at the L3-4 level was not performed because the disc space was too narrow for the smallest cage. It was a T4 to S1 fusion for Scheuermann kyphosis. At last follow-up (6 months), there was no loss of correction. For the second patient, only L4-5 OLIF was done rather than L4-S1 OLIF because the L5-S1 level could not be reached. In that case, the left iliac vein was adherent to the L5-S1 disc and the surgeon felt that mobilization of the iliac vein would have been too risky. It was a long fusion for adult lumbar scoliosis. At follow-up (3 years), there was a loss of correction with decreased disc space. In the last patient, approaching the L2-3 level was not possible due to a prominent rib cage, and only the L3-5 OLIF was performed. It was a T4-S1 fusion for global imbalance in a patient with Parkinson's disease. At last follow (6 months), there was no loss of correction.
The mean operative blood loss was 99.5 ┬▒ 254.0 ml for all patients, averaging 56.8 ┬▒ 131.3 ml per level. The mean blood loss was lowest for single-level approaches (53.9 ┬▒ 78.3 ml) and highest for two-level approaches (124.1 ┬▒ 319.1). Blood loss was 400 ml or less for all patients, except for two. The first patient lost 3,127 ml due to iliac vein laceration during a two-level L3-5 OLIF. The second patient lost 1,000 ml after laceration of the iliolumbar vein during a two-level L2-3 and L4-5 OLIF. In the last case, L3-4 postero-lateral interbody fusion (PLIF) had already been performed successfully.
As for mean operation time, it was 53.8 ┬▒ 18.7 minutes for all patients with an average of 32.5 ┬▒ 13.2 minutes per level. The mean operative time was lowest for single-level surgery (42.4 ┬▒ 16.8 minutes), increasing to 57.4 ┬▒ 14.8 minutes for two-level and 70.3 ┬▒ 26.4 minutes for three-level approaches. The average length of hospital stay was 7.1 ┬▒ 3.5 days for all patients. It was similar for patients undergoing single-level (6.5 ┬▒ 2.3 days), two-level (7.5 ┬▒ 4.0 days) and three-level (6.7 ┬▒ 3.4 days) procedures. However, some patients had longer hospital stays while waiting for transfer to a rehabilitation center. Due to the health system of our country (France) and to economic reasons, patients must stay a minimum of 4 nights in the hospital.
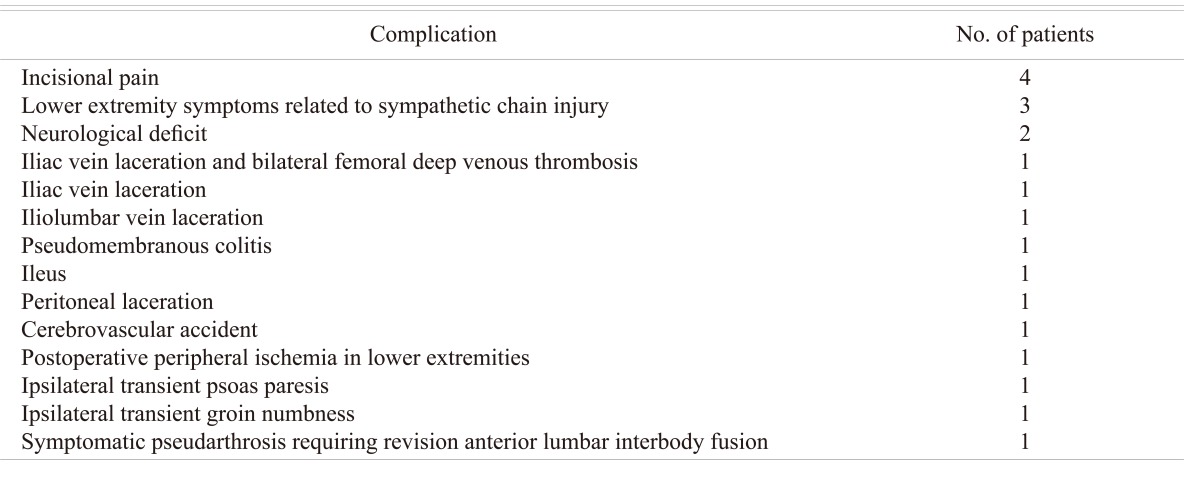
There were 19 patients with a single complication and one with two complications (Table 3). Patients with and without complications were similar with respect to age (56.2 ┬▒ 9.6 years vs. 54.1 ┬▒ 10.6 years), weight (62.3 ┬▒ 12.4 kg vs. 67.7 ┬▒ 14.7 kg), BMI (23.6 ┬▒ 3.3 kg/m2 vs. 25.0 ┬▒ 4.2 kg/m2), and the number of levels approached (1.8 ┬▒ 0.4 levels vs. 1.8 ┬▒ 0.6 levels). Of the 17 patients with more than two years of follow-up, only one had a complication consisting of left lower extremity symptoms related to iatrogenic sympathetic chain injury. The most common complication was incisional pain (2.2%), followed by lower extremity symptoms from sympathetic chain injury (1.7%). There was neither occurrence of abdominal muscle weakness nor herniation, nor retrograde ejaculation.
There were two patients with neurological deficit after left-sided L3-5 OLIF. The first patient had left L4 paresthesia and L3-4 motor weakness (grade 4 strength) presumably due to nerve stretching from restoration of disc height. For this case, surgery was uneventful and postoperative imaging did not show any misplacement of the interbody cages. The neurological deficit remained stable but she was diagnosed with pancreatic adenocarcinoma and died 4 months after the OLIF procedure. A second patient had right L4-5 paresthesia and weakness (grade 0 strength), as well as grade 3 strength in the right S1 postoperatively. Preoperatively, she already had weakness of her right lower extremity as a sequela of poliomyelitis at a young age. A CT scan showed a prominent cage of 36 mm in length at L3-4 and L4-5 compressing the dural sac contralaterally on the right side. She then underwent revision through the same incision with placement of shorter cages of 30 mm length at L3-4 and L4-5, but did not recover from her neurological injury.
One patient presented with ipsilateral weakness (grade 4 strength) in hip flexion after an L3-5 OLIF, but recovered full strength after 15 days. Due to the transient nature of the weakness, it was attributed to local pain from the surgical approach (manipulation of abdominal and/or psoas muscles). Another patient undergoing L3-5 OLIF had hypoesthesia at the upper medial aspect of the left thigh after surgery, which returned to normal, as noted at the 9-month follow-up visit. It was presumed to be caused by stretching of the ilioinguinal nerve located between internal oblique and transverse abdominal muscles at the L4-5 level near the anterior part of the iliac crest.
Two patients sustained intraoperative iliac vein laceration that was repaired primarily with non-absorbable sutures. One of these patients lost 100 ml of blood intraoperatively and presented with bilateral edema in the lower extremities postoperatively due to deep femoral venous thrombosis requiring anticoagulation treatment. Another patient had an iliolumbar vein laceration leading to a 1,000 ml blood loss that ceased after ligation. One patient decompensated from pre-existing peripheral arterial disease and presented pain in both lower extremities postoperatively due to peripheral ischemia. He improved with non-surgical treatment consisting of fluid repletion and aspirin. One patient sustained a left-sided cerebrovascular accident secondary to a patent foramen ovale associated with an anevrysm of the interatrial septum. He was treated by thrombolysis and had no residual deficit from his cerebrovascular accident.
Finally, one patient had symptomatic pseudarthrosis at the L5-S1 level after L4-S1 OLIF. She presented with persistent low back pain and underwent successful revision by posterior L5-S1 fusion followed by anterior L5-S1 fusion through a transperitoneal approach.
Discussion
This study investigated the usefulness and complications of a minimally invasive approach for anterior lumbar interbody fusion previously described by Mayer [12]. In order to distinguish this technique from others used for anterior interbody fusion, the authors suggest using the term OLIF. In spite of the design of this study, which limits its strength, this report presents the largest cohort so far in the literature, pertaining to this approach. As opposed to other studies referring to this approach [11,13], the current study shows that the original technique can be modified in order to address three levels through a "sliding window" using the same 4-cm incision. This "sliding window" is essential because in a recent series of 600 X-LIF [15] using the same two stage surgical strategy, X-LIF was performed at only one level in 80% of the cases. In our series two level surgery was performed in 60% of the cases. We also showed that the L1-2 disc can be approached in selected cases where floating ribs are relatively horizontal and mobile. As for the L5-S1 disc, OLIF through a retroperitoneal approach was performed successfully in 6 patients, but had to be aborted in one patient. In addition, one patient required revision of L5-S1 interbody fusion due to symptomatic pseudarthrosis after L4-S1 OLIF. Due to the technical complexity of approaching the L5-S1 discs using the retroperitoneal OLIF technique secondary to the need to mobilize iliac vessels and to the presence of the iliac wing, the authors suggest that another approach such as the transperitoneal approach described by Mayer [12] be strongly considered when anterior fusion of the L5-S1 is required.
Surprisingly, the operation time (53.8 ┬▒ 18.7 minutes) was markedly decreased in the current series when compared to previous reports [11-13]. The authors hypothesize that three factors could have contributed to that finding. First, no microscope was used neither specific complex ancillary, thereby decreasing the number of manipulations during surgery, especially when radiographs are needed. Second, all surgeries were performed through the same retroperitoneal approach while previous reports used a transperitoneal approach for the L5-S1 disc. Last, fusion was performed using bone substitute only, without harvesting an autogenous iliac crest bone graft, which can increase surgical time. Although an autogenous iliac crest bone graft can be harvested from the same incision, it was not done in the current study in order to avoid donor site morbidity and because the authors believe that using a bone substitute was sufficient to achieve an adequate rate of fusion clinically, especially when all patients had been stabilized posteriorly using segmental instrumentation.
Overall, minimally invasive OLIF carries about the same risks (rate and type of complications) as in traditional anterior approaches [14]. In this series, the most common complications were incisional pain (2.2% of patients) and lower extremity symptoms due to sympathetic chain injury (1.7% of patients). Vascular injury (iliac or iliolumbar vein) occurred in 3 patients (1.7%) and could be repaired successfully despite the small incision. There are many potential advantages related to the OLIF technique. Because it is a muscle-splitting approach, the incidence of abdominal wall pain is decreased and it becomes easier to develop a "sliding window" to access multiple levels through a small incision. The incision for the OLIF technique is more anterior to the traditional anterior approach and therefore spares the proximal nervous trunks innervating the abdominal muscles. Accordingly, there was no occurrence of abdominal wall atony or herniation in the current series. In addition, the OLIF technique requires only minimal posterior retraction of the psoas to insert the banana-shaped cage, thereby reducing the incidence of postoperative crural or psoas-related pain. Finally, the OLIF technique can decrease the length of a hospital stay although that remains to be verified. In the present study, the mean length of hospital stays was only 7.1 ┬▒ 3.5 days, but some patients had to stay longer in the hospital while waiting for transfer to a rehabilitation center. Moreover patients were required to stay a minimum of four nights at the hospital.
Because this study is limited by its retrospective nature, it is suggested that a prospective study be done to compare the minimally invasive OLIF to the traditional anterior retroperitoneal approach. Based on the results, age, weight, BMI, and the number of levels approached were not associated with the occurrence of complications.
A banana-shaped cage was used in association with the OLIF procedure in an attempt to facilitate the insertion of the cage and to minimize the rate of neurological injury. With such a cage, less posterior retractation of the psoas is needed to insert a cage, and the concavity of the cage decreases the risk of injury the dural sac centrally. However, as shown in one case with a neurological deficit, the risk of injuring contralateral traversing nerve roots is still present and therefore emphasizes the need to adequately assess the position of the cage either visually or radiographically. This problem is also present with X-LIF [15]. In order to decrease the incidence of this complication, the authors recommend using cages of 30 mm length or shorter in the lumbosacral spine.
With this approach the less the psoas is reclined the less patient had thigh pain and hip flexor transient weakness. In our experience, few patients complained of this problem whereas it seemed to be nearly universal with X-LIF [15].
Conclusions
This article reports the efficacy and complications of the minimally invasive OLIF technique on 179 patients. The technique was used effectively and safely for up to three levels from L2 to L5 using a "sliding window" approach. The technique described is associated with the risk of complications similar to that reported for traditional anterior approaches, with the advantage of decreasing the risk of abdominal wall weakness or herniation. For selected cases, it can also be performed at L1-2 and L5-S1, although another approach might be preferred at L5-S1 due to the risks associated with mobilization of the iliac vessels and to the presence of the iliac wing. Because of the limited access, great care should also be taken to avoid contralateral compression of dural sac and nerves roots during insertion of interbody devices.