Introduction
Spine surgeries are among the most common procedures performed worldwide. Over the years, the number and complexity of spine procedures have consistently increased [1,2]. Proper patient positioning for spine surgery is critical because it improves operating efficiency, reduces the occurrence of surgical complications, and influences surgical outcomes. Position-related complications, while rare, have the potential to cause serious morbidity in patients and can be a source of medicolegal issues and potential litigation [3]. According to an anesthesia closed-claims analysis, spine surgery accounts for more than 10% of all claims. Spine surgeries were also associated with more permanent disabilities like vision loss and nerve injuries, than other surgeries [3]. Prone positioning and long-term surgeries (>4 hours) significantly increase the risk of severe permanent injury in spine claims [3]. We discuss the most common position-related complications associated with spine surgery in this narrative review and provide a brief overview of the equipment and technical considerations for safe positioning for prone spine surgery. Furthermore, a viewpoint on patient positioning regarding spine surgery under regional anesthesia has been presented. We also discuss the intricacies of less commonly used positions in spine surgery, like lateral and sitting positions.
Position-Related Complications
1. Perioperative vision loss
Perioperative vision loss (POVL) is a rare complication of prone spine surgery, but it is one of the most feared because the effects are often permanent [4]. Various studies have shown that the incidence ranges from 0.02% to 0.16% and is higher in deformity surgeries than in lumbar fusions [5–9]. Ischemic optic neuropathy (ION) is the major reason for POVL with posterior ION being more prevalent and causing more severe vision loss than anterior ION [10,11]. Retinal ischemia, cortical blindness, acute glaucoma, and external ocular injury are other causes [11]. Although the exact cause of this complication is unknown, several risk factors have been linked to it. Male sex, Wilson frame use, increasing duration of surgery, increased blood loss, and less use of colloids have all been proposed as ION risk factors [12,13]. Another nationwide in-patient sample study of spinal fusion patients identified deformity correction surgery, diabetes mellitus with end-organ damage, and extremity paralysis as independent risk factors for POVL [6]. POVL risk factors have also been identified as intraoperative hypotension, anemia, and peripheral vascular disease [8].
POVL prevention should take a multifaceted approach. The patient’s preoperative counseling and disbursing information for this uncommon complication are critical. Consenting to this uncommon complication remains poor, with studies indicating that more than half of patients are not counseled about POVL risk [4,14]. Patients undergoing long-term surgeries (>6 hours), those with high expected blood loss, and those undergoing deformity correction should be counseled on the risk of POVL, with a case-by-case review for shorter-term surgeries. When compared to normal prone positioning, positioning the patient with the orbit level above the heart (reverse Trendelenburg) is effective in lowering intraocular pressure [15]. Additionally, compared to the head-down position, the head-neutral position is associated with a lower conjunctival chemosis incidence [16]. Other effective strategies include the anesthetist verifying the eyes for pressure and position frequently, avoiding hypotension, estimating blood loss and providing adequate replacement as needed, and using colloids with crystalloids for replacement [17]. Alternatives to the Wilson frame include the three-pin holder frame and foam headrests, which reduce eye strain [17].
2. Perioperative neuropathies
Though uncommon, perioperative peripheral nerve injuries (PPNI) are significant due to the potential loss of function, increased patient morbidity, and risk of litigation associated with disability [18]. The mechanism for these injuries is not well understood, and in most cases, no apparent mechanism is found [18]. When a patient is sedated for prone spine surgery, the protective reflex restricting excessive loading or irritation of the peripheral nervous system is lost, increasing PPNI risk [19]. The ulnar nerve, brachial plexus, and the thigh’s lateral femoral cutaneous nerve (LFCN) are the most commonly injured peripheral nerves. These neuropathies are discussed in depth in the following subsections.
1) Ulnar nerve palsy
One of the most commonly reported postoperative peripheral nerve injuries is ulnar nerve palsy [20]. It accounts for roughly one-third of anesthesia malpractice claims involving nerve injury [18]. Ulnar nerve injuries are also common in prone spine surgery, but the exact frequency is unknown [21,22]. Pressure at the elbow at the cubital tunnel, elbow flexion greater than 90°, blood pressure cuff malposition, accidental falling of the arm during surgery, and obesity are all risk factors for ulnar nerve palsy. More than 70° and 100° of elbow flexion have been shown to significantly increase intraneural and extraneural compression, respectively, while both flexion compressions are lowest at 45° [23]. Flexion of the elbow by >135° causes nerve elongation of nearly 18%, and hence extreme flexion increases the likelihood of ischemia and nerve injury [24]. Another study compared the change in intraoperative neural monitoring (IONM) signals concerning upper extremity nerve injuries and discovered a considerably higher somatosensory evoked potential (SSEP) change in the prone-superman and lateral decubitus positions (6.5%–7% cases) compared to other positions like supine arms out, supine arm tucked, and prone arms tucked (1.8%–3.2%) [25]. Preventive measures include detecting pre-existing cubital tunnel syndrome, avoiding excessive elbow flexion and pressure, and using IONM [23,24]. IONM is effective in detecting a change in SSEP early, and changing arm position at this stage can help prevent postoperative neurological injuries [25].
2) Brachial plexus injury
Brachial plexus injury (BPI) following prone positioning is becoming more common. Most of these injuries are traction injuries caused by patient misalignment, with neuropraxia being the most common mechanism [26]. The nerve plexus is fixed between the axillary fascia on one end and the cervical vertebrae on the other, increasing the possibility of traction injury. Furthermore, because the neural plexus passes through mobile bony structures like the head of the humerus, clavicle, and first rib, it is susceptible to ischemia due to compression or stretching over these structures in certain arm positions [26]. Hypothermia, hypovolemia, alcoholism, diabetes mellitus, and arm abduction greater than 90° have all been linked to increased BPI risk [26]. Other risk factors for this uncommon complication include abduction, extension, external arm rotation, neck rotation and lateral flexion in the same direction, and the use of shoulder braces [26] (Fig. 1). It has been observed that BPI in the prone position is more likely to cause motor deficit [27]. Because these are neuropraxia injuries, recovery is usually expected. However, due to the proximal nature of the injury, recovery is frequently incomplete [28]. Proper positioning, avoiding excessive positional stretches on the roots, and the use of IONM are all preventive strategies. It has been observed that intraoperative changes detection in IONM signals and immediate corrective measures can prevent the development of postoperative deficits [26].
3) LFCN neuropathy
With a reported incidence of 10%–24%, LFCN neuropathy or meralgia paresthetica is common in posterior spine surgery [29–31]. Pelvic support or bolster placement near the anterior superior iliac spine is the prevalent cause of the compression. Postulated risk factors include long duration of surgery (>3.5 hours), degenerative spinal disease, obesity, and surgery in lean-built patients [29,31]. The use of the Relton Hall frame has also been linked to an increased LFCN risk and bilateral injury [30,31]. The condition is self-limiting, and the prognosis is excellent, with half of the patients recovering within 1 week and all recovering within 3 months [31]. Preventive measures include keeping support below the anterior superior iliac spine, proper post padding, and minimizing retraction during bone graft harvest [30].
3. Pressure ulcers
Pressure ulcers are common as a result of prone positioning in spine surgery, with estimates ranging from 5.9% to 23% [32,33]. These figures can rise even higher in longer cases (>3 hours) and spine deformity surgery [33,34]. It has been observed that the presence of pressure ulcers can result in 13% longer hospitalization times [32]. Fortunately, the majority of these ulcers are National Pressure Ulcer Advisory Panel (NPUAP) Grade 1 or 2. Higher-grade ulcers (NPUAP 3 and 4) are rarely responsible for positioning alone [33]. The face, inguinal region, and chest are the most common locations for these ulcers [32,33]. Previous skin problems, myelopathy, and a lower preoperative plasma protein concentration are all risk factors for the development of pressure ulcers [32,33]. Long operative duration (>300 minutes), four or more levels of intended interbody fusion, spinal deformity surgery, hypotension, and higher patient temperature are all intraoperative risk factors [33,34]. In addition to pressure ulcers, excessive pressure on vascular structures can result in compartment syndrome [35,36]. There have been reports of patients developing anterior thigh compartment syndrome when operated on the Jackson frame for lumbar pathology, and of patients developing tibial compartment syndrome when operated on the Andrews frame in a prone-sitting position [35,36]. To prevent pressure ulcers, adequate padding and attention to bony prominences are required, and risk factors for ulcer development should be avoided. Certain materials and devices can aid in the prevention or reduction of pressure ulcers. Grisell and Place [37] compared three different head positioners: OSI (Orthopedic Systems Inc., Union City, CA, USA) disposable polyurethane foam head positioner, ProneView protective helmet system (Dupaco Inc., Oceanside, CA, USA) with a polyurethane foam head positioner, and ROHO device (The ROHO Group, Belleville, IL, USA) with a neoprene air-filled device. When compared to other devices, the ProneView system showed significantly lower pressure at the forehead and chin [37]. Pressure ulcers were significantly higher in the OSI patient group. Another study found that soft silicone foam dressings were significantly better than polyurethane foam dressings at preventing intraoperatively acquired pressure ulcers in prone spine surgery [38].
4. Hemodynamic changes
Prone positioning during spine surgery poses unique difficulties for the anesthetist and spine surgeons due to varied hemodynamic changes. Compression of the abdomen causes engorgement of epidural and paravertebral veins due to inferior vena cava compression and increases bleeding in the surgical field. Furthermore, the prone position is linked to hypotension and decreased cardiac function [39,40]. It has been proposed that the main reasons for the drop in blood pressure are a decrease in stroke volume and cardiac index [41]. It has also been demonstrated that the type of operating table used influences the various hemodynamic parameters. Dharmavaram et al. [40] discovered that Wilson (OSI model no. 5319[G] 5321[G]; Orthopedic Systems Inc.) and Siemens AG frames had lower cardiac output. The Andrews (model no. 914; Mizuho OSI, Union City, CA, USA), Wilson, and Siemens systems reduced cardiac index and stroke volume; the Andrews frame resulted in a lower cardiac preload. The use of longitudinal bolsters and the Jackson spine table (OSI model no. 5840–831; model no. 5840-831; Mizuho OSI) had the least effect on cardiac performance [40].
What Can Make Prone Spine Surgery Safe?
1. Headrests
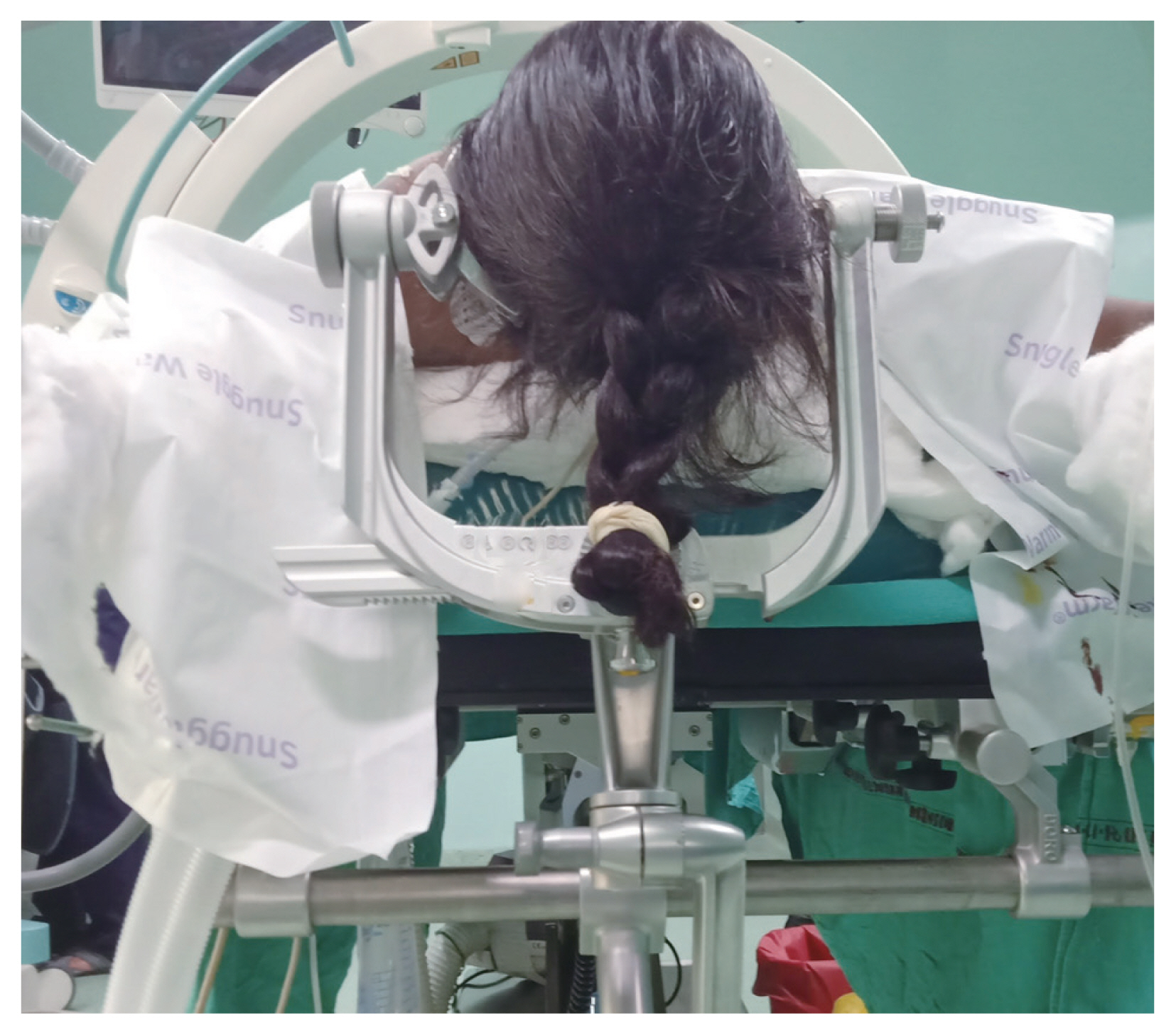
The ideal headrest for prone spine surgery provides adequate head stability, and minimal compression of the face and eyes, and allows for monitoring while avoiding various position-related complications. Unfortunately, all of these qualities are difficult to find in a single type of headrest. Classic horse-shoe-shaped headrests have the problem of inability to provide head stability and cause compression of one of the eyes [42]. The Mayfield skull clamp is a 3-point clamp that is secured to the skull’s outer table. Their sine surgery application has also been described. The benefits include stable head fixation and no external pressure on the eyes and face [43]. However, the device’s invasive nature and potential complications like minor skin lacerations, extradural hematomas, meningitis, and cerebrospinal fluid rhinorrhea have limited its use in spinal procedures [44,45] (Fig. 2). Prone positioner/OSI head positioner (Orthopedic Systems Inc.), ROHO head positioner (The ROHO Group), and ProneView (Dupaco Inc.) are some other popular headrests [37]. In terms of lower facial pressures, the ProneView system is superior to the other systems [37,46]. It was also discovered that the ProneView system caused fewer facial ulcers than the OSI head positioner [37]. A face-contoured polyurethane headrest covered by a plastic shield sits on top of a viewing mirror in the preview system. This type of system not only reduces facial pressure and the risk of pressure ulcers but also keeps the eyes free of any extraocular pressure. The viewing mirror allows the anesthetist to confirm and check that the eyes are not under any pressure [42]. However, this system raises concerns about cost, availability, and limited access and viewing when sterile drapes are in place. The latter can be addressed by the ProneView Video Camera Monitoring System (Dupaco Inc.), which attaches a camera cartridge to an LCD (liquid-crystal display) monitor and provides continuous on-screen monitoring of the face and eyes even when mirror and lighting access is limited [42].
2. Intraoperative neural monitoring
Many authors have reported that the use of SSEP can be effectively used to monitor peripheral nerve function in patients undergoing prone spine surgery, with early identification and possible prevention of upper extremity nerve injury (peripheral nerve injury and brachial plexus injuries) [25,47–50]. SSEPs have primarily been used to assess the central nervous system’s integrity during various spinal and neurosurgical procedures, but the detection of peripheral nerve injuries is an added benefit. Loss of SSEP signals intraoperatively can indicate an impending nerve injury; changing the position of the upper extremity at this stage often results in signal return and thus potential prevention of PPNI. Reducing elbow flexion and extension, shoulder abduction to <90°, removing compressive bandages and tapes, and reducing wrist extension are all possible maneuvers. In most patients, intraoperative extremity manipulation improves the SSEP signal, preventing potential nerve injuries [25,47]. Despite the benefits, the use of IONM for this purpose is not widespread due to limited availability, high costs, and a lack of public awareness. Furthermore, only the status of the nerves being monitored can be commented on, and monitoring of all peripheral nerves may be impractical. When IONM is used, however, SSEP monitoring can be used to detect intraoperative upper extremity neuropraxia.
3. Proper patient positioning
Proper patient positioning is in prone spine surgery and should be given the undivided attention of both the surgeon and the anesthetist before the procedure begins. In prone surgery, patients are primarily positioned in two positions: prone arms tucked and prone surrender position [51]. When compared to the prone surrender position, the prone arms tucked potion has a lower incidence of SSEP changes in the upper extremity [37]. In the prone arms tucked position, the arms should be neutral with palms facing the body. Arms and legs should be sufficiently padded and protected. Shoulder traction is frequently required for lower cervical spine imaging, but it should be avoided whenever possible [51]. Shoulder abduction should be less than 90° for the prone surrender position, arms should be well padded, elbow flexion greater than 90° should be avoided, forearms should be in the neutral or prone position, and wrist extension should be avoided [51] (Fig. 3). The head should be centered in the midline, with no lateral rotation. All bony prominences should be optimally padded in both positions. These precautions reduce the likelihood of PPNI and pressure ulcers [51].
4. Padding material
A variety of materials have been used as operating table surfaces and for extremity padding during surgery. Soft, lightweight, with good shape memory, cheap, easy to clean, compressible, insulating, non-inflammable, non-irritant, and minimally adhesive materials are ideal for these applications [52]. When compared to a standard operating table, Nixon et al. [53] found a lower incidence of pressure ulcers with a dry viscoelastic polymer. Another study found that polyurethane and polyether mattresses had significantly lower interface pressures than foam and gel mattresses when comparing the effect of four different mattresses on pressure ulcers. It was interesting to note, however, that none of the mattresses reduced pressure sufficiently to prevent the development of pressure ulcers [54]. In long-term (>3 hours) prone spine surgery, high-density foam (HDF) pads were compared to viscoelastic polymer (VP) pads. While the mean and peak pressures measured in VP pads were significantly lower than in HDF pads, the difference in pressure ulcer rates between the two groups did not translate. A high initial cost is another factor limiting the use of VP pads [55]. More research is needed in this area, and the search for the ideal padding material continues.
5. Appropriate table for surgery
There are numerous surgical tables available today, and understanding the characteristics and limitations of each table is critical for the best results. Wilson frame, Relton Hall frame, Andrews frame, Jackson spine table, and conventional radiolucent table with bolsters are some of the most commonly used tables and frames. Table 1 summarizes the benefits and drawbacks of various commonly used spine surgery tables [12,31,42,56–63]. Hence, the benefits and drawbacks of each frame should be carefully considered before deciding on the best surgical table for a particular case.
6. Use of regional anesthesia for spine surgery
For lumbar spine surgery, the use of regional anesthesia rather than general anesthesia is gaining traction. Regional anesthesia has several advantages, including a shorter hospital stay, a lower incidence of postoperative nausea and vomiting, comparable postoperative function, and lower overall complication rates [63,64]. Another added advantage of using regional anesthesia is the potential to reduce position-related complications because patients are awake and can reposition themselves, avoiding ophthalmic complications, facial ulcers, and upper limb nerve injuries [65]. In cases of lumbar microdiscectomy, Ulutas et al. [65] reported a lower rate of ophthalmic complications with epidural anesthesia. However, the limited indications (primarily lumbar spine surgeries), time constraints associated with regional anesthesia, and several contraindications (multilevel fusion, unpredictable or long duration of surgery, respiratory issues and limited lung reserve, anxious patient, high body mass index, need for a protected airway, etc.), its widespread use is currently limited [64]. Nonetheless, regional anesthesia appears to play a role in reducing position-related complications, and more research is needed to investigate this.
Other Positions
1. Lateral Decubitus position
When anterior spinal surgery and transpleural approaches were commonly used to approach anterior pathologies such as spinal tumors and spinal tuberculosis and perform anterior column fixation, the lateral decubitus position in spine surgery was popular [66,67]. With the development of dependable posterior fixation techniques and access to the anterior column via posterior approaches, the use of anterior approaches in spine surgery has decreased. However, with the popularity of surgeries like lateral and oblique lumbar interbody fusion, the use of the lateral decubitus position in spine surgery has seen a resurgence [68]. In this section, we discuss the unusual problems and complications associated with this position and potential solutions. The lateral decubitus position has been linked to a higher incidence of upper extremity nerve injuries as detected by SSEP when compared to the prone arms tucked, supine arms, tucked and supine arms out positions [25]. The compression of the dependent brachial plexus, which is compressed between the thorax and the humeral head, has been attributed to this [69]. According to estimates, the mean pressure under the dependent shoulder is 66 mm Hg and can exceed 100 mm Hg [70]. The use of a chest roll under the chest (not axilla) can help reduce these pressures, lowering the risk of BPI. The use of rolls in the axilla should be avoided because it puts pressure on the brachial plexus [70]. A one-liter saline bottle, gel pads, and an inflatable chest roll are all options for roll material. The latter is significantly better than the other two in terms of pressure reduction on the dependent shoulder and thorax. Inflatable chest rolls have been shown to reduce pressure under the dependent shoulder by approximately threefold [70]. The use of a second inflatable pillow under the head can help to prevent excessive lateral neck angulation, keep the neck in line and reduce pressure under the dependent axilla [70]. Excessive elbow flexion and extension, forearm pronation, and non-dependent arm-shoulder abduction greater than 90° should be avoided. Excessive elevation of the non-dependent arm over the shoulder can increase the risk of the radial nerve and BPI, so the arm should be horizontal and level with the shoulder [20]. Other high-risk areas for pressure injury include the dependent lateral malleolus, knee, and iliac crest, which should be adequately padded to prevent pressure ulcers [20]. Even in the lateral position, POVL is a potential complication [71]. In lateral spine surgery, an asymmetric bilateral PION with more loss in the dependent eye has been reported [72]. Avoiding compression of the dependent eye, maintaining a neutral forward position of the neck to facilitate eye venous drainage, and positioning the head above the heart when possible, especially in high-risk patients, are all prevention strategies [73].
2. Sitting position
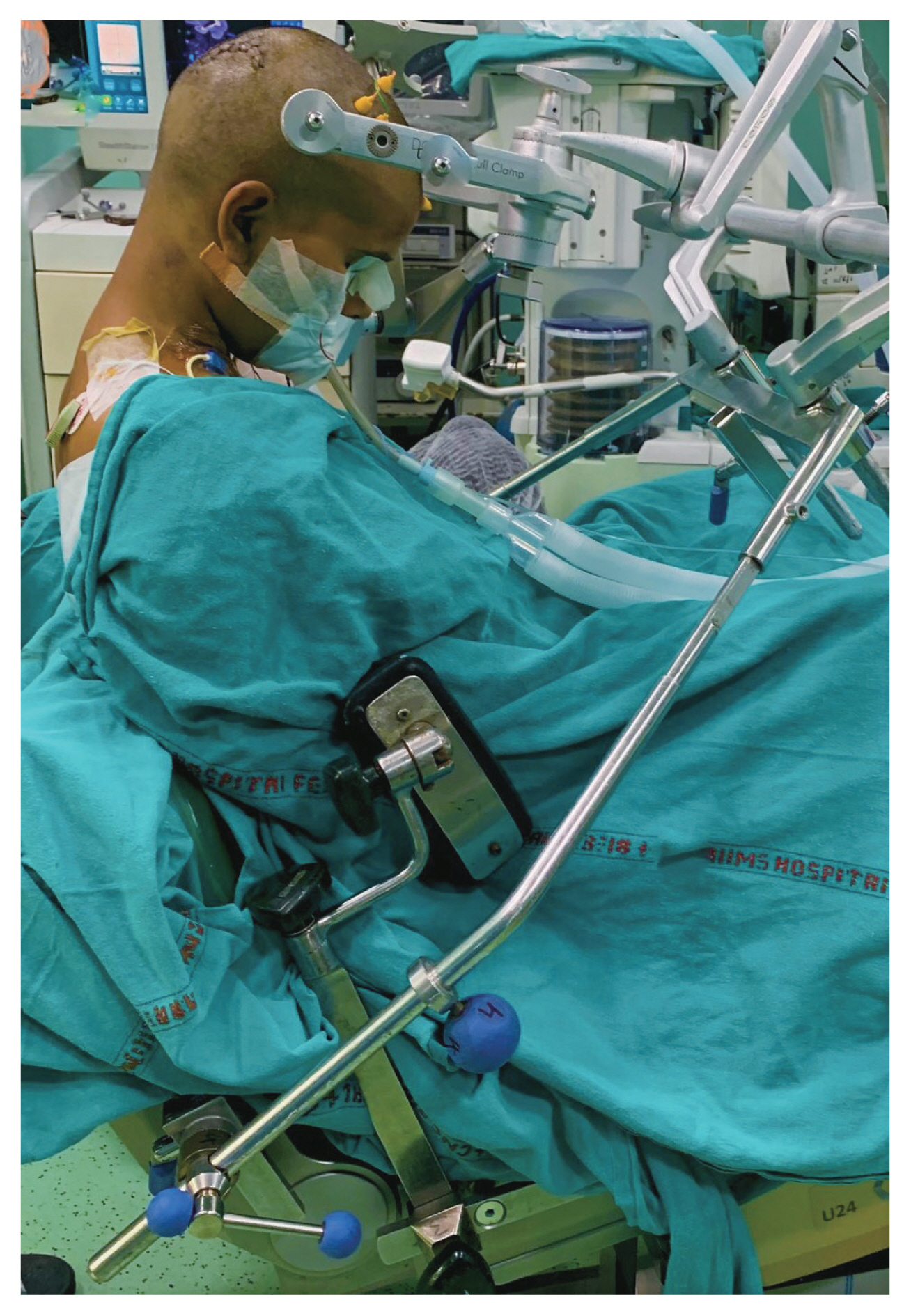
For a long time, the sitting position has been used in the cervical spine and intracranial surgeries. It provides the advantages of improved surgical access, improved venous drainage, lower intracranial pressure, blood drainage away from the field, and potentially reduced transfusion requirements [74–76]. The anesthetist benefits include improved ventilation due to lower intrathoracic pressure, improved airway access, and easier cardiopulmonary resuscitation if necessary [77]. The overall complication rate in sitting surgery is estimated to be 1.45% [76]. Complication rates for sitting cervical procedures are lower (0.7%) than for sitting cranial procedures, with an odds ratio of 0.28 [76]. There are numerous potential complications associated with the sitting position, including venous air embolism (VAE), hypotension, paradoxical air embolism, airway edema, macroglossia, decreased cerebral pressure, pneumocephalus, subdural hematoma dislocation of the elbow, displacement of endotracheal tubes, jugular venous obstruction, compartment syndrome, lumbosacral pressure sores, central cord syndrome, paraplegia, quadriplegia, and common peroneal nerve palsy [77–85]. The most common and feared complications of this position are VAE and associated hypotension. Various studies have estimated the incidence of VAE occurring in this position to be 4.7%–30% [86]. The detection of VAE is both users- and technique-dependent with trans-esophageal echocardiography being more sensitive than Doppler ultrasound [86,87]. The rate of clinically significant VAE with associated hypotension, however, has been estimated to be 1%–6% [86]. Due to the risk of paradoxical air embolism, a patent ventriculoatrial shunt, right-to-left cardiac shunt, and patent foramen ovale are absolute contraindications for this position due to risk of paradoxical air embolism [84]. So, in patients scheduled for surgery in the sitting position, a thorough preoperative cardiac evaluation is required. Age extremes, uncontrolled hypertension, and chronic obstructive airway disease are all relative contraindications [84]. Preoperative and intraoperative management of hypotension in the sitting position is required by the anesthetist. It can be reduced by administering fluid before positioning, using vasopressors, and positioning in a fully seated position. The hips and knees must be flexed to increase the venous return, which also reduces the risk of sciatic nerve palsy [88]. Adequate invasive arterial blood pressure monitoring at the head level contributes to adequate cerebral perfusion pressure [79]. Oral airway placement combined with extreme neck flexion can result in airway obstruction due to tongue, pharynx and palate swelling [78]. In this position, it is critical to ensure that careful positioning, padding of pressure points, and extreme neck flexion are avoided [86]. An exemplary image has been shown in Fig. 4.
Conclusions
Though rare, position-related complications in spine surgery have the potential to cause significant morbidity in patients and negatively impact surgical outcomes. Given the medicolegal implications, surgeons must be aware of the risk factors associated with these complications and concentrate their efforts on taking the necessary precautions to avoid them. The advancement in the design of some of the newer equipment, and the introduction of “awake” techniques utilizing regional anesthesia in spine surgery, can reduce the occurrence of position-related complications in spine surgery.