Incidence and Skeletal Features of Developmental Cervical and Lumbar Spinal Stenosis
Article information
Abstract
Study Design
Cross-sectional study.
Purpose
To report the prevalence and relationship of developmental cervical and lumbar spinal stenosis (DCSS and DLSS) with the bone parameters of the skull and extremities.
Overview of Literature
DCSS and DLSS are found occasionally in daily practice. DCSS and DLSS can cause compressive myelopathy, radiculopathy, and cauda equina syndrome; however, data on their prevalence and correlation with skull and skeletal extremity profiles is scarce.
Methods
A cross-sectional measurement study of 293 whole-body dried-bone samples was conducted. We measured the anteroposterior (AP) and transverse diameter of the fourth to sixth cervical vertebrae (C4–C6) and third to fifth lumbar vertebrae (L3–L5). Stenosis of the cervical spine and lumbar spine was defined as an AP diameter of <12 mm and <13 mm, respectively. We also measured the skull circumference, the AP and transverse diameters of the foramen magnum, the inner and outer inter distances between the left and right orbital bones, the humerus length, and the femoral length. Kruskal-Wallis and post hoc analyses were used in the statistical analyses.
Results
The age was 22–93 years. DCSS was found in 59 (20.1%) and DLSS in 28 (9.6%). Twelve samples had both DCSS and DLSS (development spinal stenosis, DSS). When compared to the “no spinal stenosis sample,” DSS (−), DCSS and DSS had a significantly smaller skull circumference, the transverse diameter of the foramen magnum, and inner and outer distance between the orbital bone (p<0.05). There was no significant difference in humeral length, femoral length, or AP diameter of the foramen magnum.
Conclusions
DCSS was correlated with a small skull, a small transverse diameter of the foramen magnum, and a small orbital bone. A small skull was strongly associated with a small cervical canal. DLSS, on the other hand, was unrelated to either a small cervical canal or a small skull.
Introduction
Anteroposterior (AP) spinal development is complete by the age of 5 years, while the transverse spinal canal diameter stops growing by the age of 15–17 years, and the spinal canal does not grow after the age of 18 years [1,2]. DSS is a condition in which the spinal canal does not grow sufficiently during these growth processes, resulting in developmental cervical spinal stenosis (DCSS) [3] and/or developmental lumbar spinal stenosis (DLSS) [4]. DCSS and DLSS are important spinal diseases encountered often in daily practice. Myelopathy in DCSS [5] and cauda equina syndrome and radiculopathy in DLSS [6] are relatively common and frequently necessitate surgical treatment. However, few reports have investigated the prevalence of DCSS and DLSS [7–9].
Kasai et al. [10] studied the physical characteristics of patients with DCSS and reported on the small inter inner canthal distance on the face. Cheung et al. [11] and Lai et al. [12] recently proposed that DLSS may be a multifactor hereditary disease similar to hypertension, diabetes, cancer, or dementia. As a result, we concentrated on height, head size, face shape, and upper limb length as physical features that are easily influenced by genetic information, and we investigated skeletal features other than the spine in people with DCSS and DLSS. In the current study, we first investigated the frequency of DCSS and DLSS using human systemic bone specimens; then, we examined the skeletal characteristics of DCSS and DLSS using skulls, upper arms, and femurs, which have relatively easy-to-understand features. Finally, we talked about DCSS and DLSS, as well as their respective pathogenesis. The goal of this study was to report on the prevalence and relationship of DCSS and DLSS with skull and extremity bone parameters.
Materials and Methods
The materials were the whole-body dry bones of 293 cases who died in northeastern Thailand. Each whole body included the cervical and lumbar spines, skull, humeri, and femurs, without apparent fractures or surgical damage. The bones were donated to the Department of Anatomy of Khon Kaen University and were examined by the Human Bone Warehouse for Research Unit. At the time of death, age ranged between 22 and 93 years (average, 67.0 years). The Ethics Committee for Human Research of Khon Kaen University reviewed and approved the study (approval no., HE611293).
We measured the AP and transverse diameters of the spinal canal of the 4th, 5th, and 6th cervical spines, 3rd to 5th lumbar spines, the skull circumference, the AP and transverse diameters of the foramen magnum, the inner and outer inter distances between the left and right orbital bones (Fig. 1), the length of each humerus and femur. The AP and transverse diameters of the spinal canal of the 4th, 5th, and 6th cervical and lumbar spines, as well as the AP and transverse diameters of the foramen magnum and the inner and outer inter distances between the left and right orbital bones, were measured using a digital vernier caliper (Mitutoyo series 500-193 ABSOLUTE Digimatic Caliper, 300 mm/12”; Mitutoyo Corp., Kawasaki, Japan). The skull circumference was measured using a tape measure by connecting the interbrow and external occipital protuberance as the landmarks (Fig. 2). Using a dedicated measuring device, the distance from the proximal end of the humeral head to the tip of the trochlea humeri represented the humerus length (Fig. 3), while the distance from the proximal end of the femoral head to the tip of the femoral medial condyle represented the femur length. The average value of the left and right lengths was adopted as the measurement value. Two orthopedic surgeons (Y.K. and P.P.) independently performed all the bone measurements, and if the difference in the measured value was ≤3 mm, the measurement value was considered a match, and the average value of both was adopted. When there was a difference of ≥4 mm in the measurement value of both, another orthopedic surgeon (T.W.) completed a new measurement, and the value of the first two measurements closest to that of T.W. was adopted.
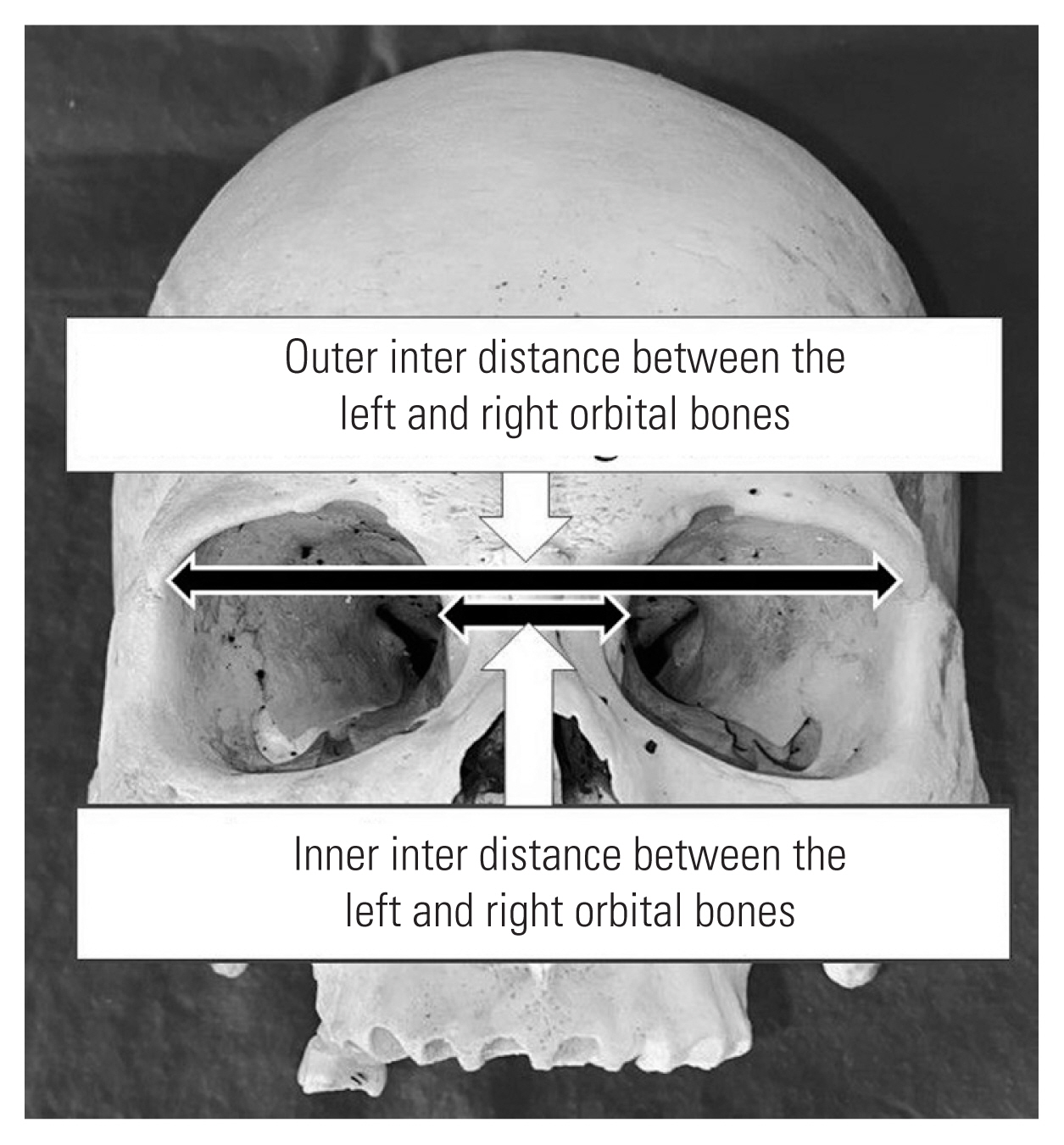
Inner and outer inter distances between the left and right orbital bones.

Skull circumference measured using a tape measure by connecting the inter-brow and external occipital protuberance as measuring landmarks.

Humerus measured using a dedicated measuring device—distance from proximal end of humeral head to tip of trochlea humeri.
As shown by Horne et al. [13], the criteria for determining DCSS are DCSS (+) if all AP diameters for C4, 5, and 6 are <12 mm (Fig. 4). Then, as per Postacchini and Pezzeri [14], the determination criteria for DLSS are DLSS (+) if all AP diameters of the spine canals of L3, 4, and 5 are <13 mm (Fig. 5). All 293 cases were then subdivided into four groups: (1) the DSS (−) group with neither DCSS nor DLSS; (2) the DCSS (+) group without DLSS; (3) the DLSS (+) group without DCSS; and, (4) the tandem DSS (+) group with both DCSS and DLSS. Age, skull circumference diameter, AP and transverse diameters of the foramen magnum, inner and outer interorbital distances, humerus length, and femoral length were the eight items compared among the four groups.
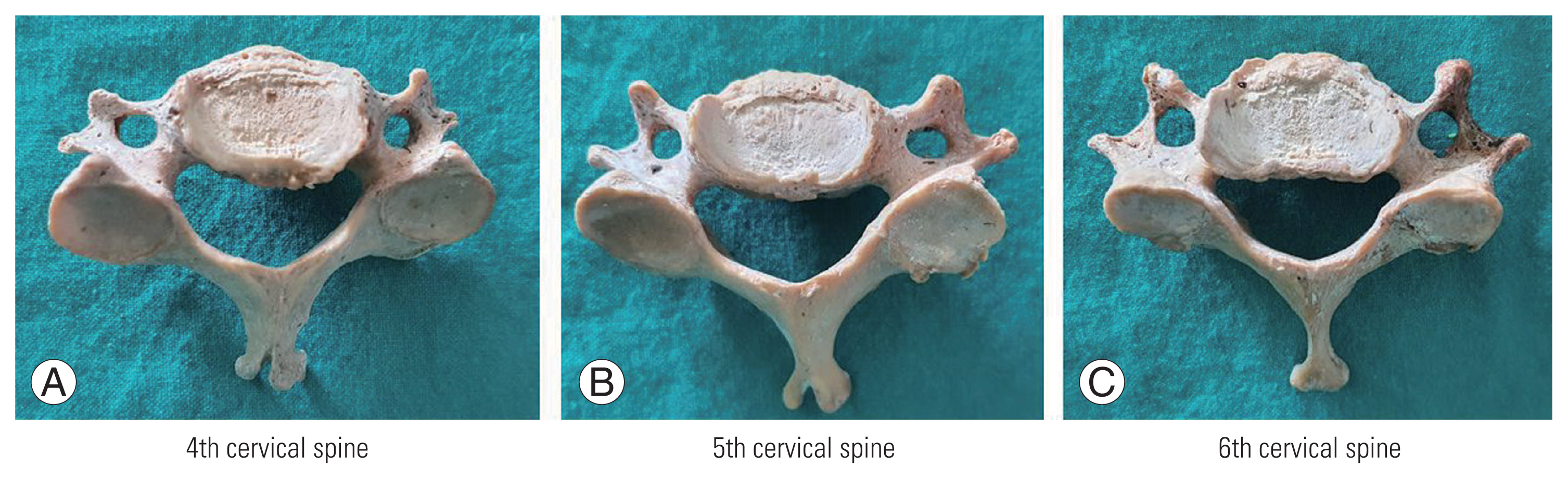
(A–C) Developmental cervical spinal stenosis the fourth to sixth cervical spine.
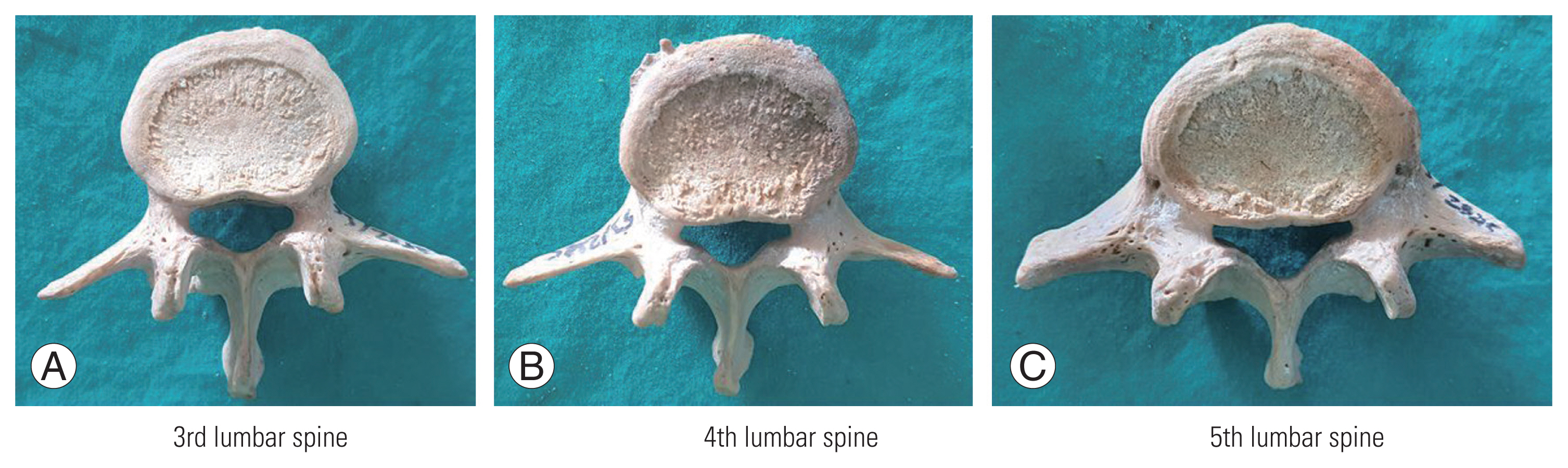
(A–C) Developmental lumbar spinal stenosis the third to fifth lumbar spine.
We tested for any significant difference using the Kruskal-Wallis test using post hoc multiple comparisons and the Bonferroni method. A p<0.05 indicated a significant difference. For DCSS and DLSS, kappa statistics were used to assess interobserver agreement between two orthopedic surgeons and intraobserver agreement by one reader (Y.K.). The intraclass correlation coefficient (ICC) was determined for skull circumference, the AP and transverse diameters of the foramen magnum, the inner, and outer inter distances between the left and right orbital bones, the humeral length, and the femoral length. The kappa and ICC value were assessed: 0–0.2 indicated slight agreement, 0.21–0.4 fair agreement, 0.41–0.6 moderate agreement, 0.61–0.8 substantial agreement, and 0.81–1 excellent agreement. The level of significance (p-value) was set at 0.05. All statistical analyses were performed in IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA).
Results
Of the 293 cases, DCSS (+) was found in 59 (20.1%) and DLSS (+) in 28 (9.6%). As for the number of cases in the four groups, the DSS (−) group had 218 cases, the DCSS (+) group had 47, the DLSS (+) group had 16, and the tandem DSS (+) group had 12. Table 1 displays the kappa or ICC values for each measurement, as well as the 95% confidence intervals. Because all of the values are >0.9, the reliability is very high.

Kappa values or interclass correlation coefficient for all measurements
The results compared among the four groups are presented in Table 2. The results of the Kruskal-Wallis test using post hoc multiple comparisons with the Bonferroni method showed significant differences (p<0.01) vis-à-vis skull circumference and the outer inter distances between the left and right orbital bones (p<0.001), the transverse diameter of the foramen magnum, and the inner inter distances between the left and right orbital bones. In the between age groups comparison, significant differences were observed between the following groups: (1) skull circumference between the DSS (−) group and the DCSS (+) group (p<0.001); (2) skull circumference between the DSS (−) group and the tandem DSS (+) group (p<0.01); (3) skull circumference in the transverse diameters of the foramen magnum, between the DSS (−) group and the DCSS (+)group (p<0.05); (4) skull circumference between the DSS (−) group and the tandem DSS (+) group (p<0.05); (5) inner inter distances between the left and right orbital bones, between the DSS (−) group and the DCSS (+) group (p<0.05); and, (6) outer inter distances between the left and right orbital bones, DSS (−) and DCSS (+) (p<0.001), and DSS (−) and tandem DSS (+) (p<0.01). There were no significant differences in age, foramen magnum AP diameters, humerus length, or femur length between the four groups.

Data compared among the four groups
Discussion
Our results showed that the prevalence of DCSS was 20.1% versus 9.6% for DLSS. Although this study only included men, we discovered that the number of cases with DCSS and DLSS was relatively high in the general healthy population. Zhang et al. [9] conducted previous studies on the prevalence of DCSS or DLSS reported that DCSS was seen in about 10% of 411 healthy cervical X-ray images. In other cohorts by Lai et al. [7] and Nagata et al. [8] using lumbar MRI, the prevalence of DLSS was 30.2% and 7.3%, respectively. Our findings were similar to the DLSS prevalence reported by Lai et al. [7], but differed from other reported prevalences, possibly due to differences in evaluation methods and DCSS and DLSS criteria. Our findings are based on measurements of the spinal canal obtained through direct observation. By comparison, Postacchini et al. [15] described variation in the spinal canal size between Caucasians, so he cited the need for further research on non-Asians, hence our study.
In our study, persons with DCSS (+) had a smaller skull circumference and the outer inter distances between the left and right orbital bones, and a strong relationship was demonstrated between the size of the head and the AP diameters of the cervical spinal canal. The entire head was confirmed to be small, and the width of the skull was especially narrow, and these findings may indirectly support the authors’ previous claim that the inter inner canthal distance was short. Notani et al. [16] and Yamahata et al. [17] reported that the size of the atlas and the spinal canal of the atlas was narrow in patients with DCSS, and our results confirmed that the transverse distances of the foramen magnum were significantly small. This observation demonstrates the strong correlation between head size and the cervical spine size. Nightingale [18] investigated the physical characteristics of patients with DCSS and discovered that they had shorter upper limb lengths; however, our findings did not support this observation.
We did not identify any particular physical characteristics for persons with DLSS (+) in the present study. However, Griffith et al. [19] reported that the people with wide AP lumbar spinal canals were typically taller individuals. We cannot confirm the report because our results showed no difference in femoral length between the DSS (−) and DLSS (+) groups.
Suspected causes of DSS include preterm birth, placental underdevelopment, malnutrition during the fetal period, smoking of mothers, and perinatal problems such as premature babies [20–22]. Cheung et al. [11] conducted a genome-wide association study on DLSS and found a significant single nucleotide polymorphism (viz., low-density lipoprotein receptor-related protein 5 [LRP5]; 11q13.2). LRP5 is a cell surface Wnt/beta-catenin signaling coreceptor that is important in bone formation during the fetal and growing stages. In a cluster detection test, LPR5 showed distinctly different patterns at L1–L4 and L5–S1, indicating the possibility of a region-specific genetic predisposition. There remains much to be elucidated, but considering the results of this study, there may be genetic information that causes DSS. We speculate that if LRP5 is expressed in the cervical spine, it might indicate DCSS (+); if expressed in the lumbar spine, it might indicate DLSS (+). If expressed in both the cervical and lumbar spines, it might indicate tandem DSS (+). As a result, while DCSS and DLSS share the same disease concept and pathogenesis, their physical characteristics may differ due to the presence or absence of genetic information for head size.
For clinical relevance, the small in skull circumference and the outer inter distances between the left and right orbital bones patients tended to have DCSS (+). Before undergoing surgery, a computed tomography scan should be performed to determine the size and width of the cervical spine parameter and foramen magnum. In our study, the DLSS (+) did not show any relationship with appendage skeletal bone and skull morphology in our study, which was similar to the results from Lai et al. [23]. The DLSS (+) correlated with canal circumference, pedicle morphology, sagittal vertebral body width to pedicle width ratio, and facet morphology [23,24], which was difficult to conduct in our study due to the difficulty in obtaining a valid measurement value. However, the DLSS (+) showed the clinically relevant in considered as risk factors of acute and chronic radicular pain, increased tendency to have reoperation for spinal stenosis, and a higher rate of adjacent segment degeneration after operation [25–27]. More prospective radiographic studies should be conducted to better explain the DLSS and its clinical significance.
The limitations of this study were (1) the number of samples from females was limited, so only males were examined, and (2) clinical data such as height and weight could not be obtained. Although our data was only for men, we were able to show that the prevalence of DCSS was 20.1% compared to 9.6% for DLSS. We also discovered that people with DCSS had a small skull circumference and a short lateral distance between the left and right orbital bones. A small head and a thin face may indicate the presence of DCSS, so spinal surgeons and general practitioners may find this observation useful. This study provides background information on the definition and pathogenesis of DCSS and DLSS.
Conclusions
The small skull, small transverse diameter of foramen magnum, and small orbital bone were significant correlated with DCSS. The small head strongly related to small cervical canal. Whereas, small head and small cervical canal did not relate with DLSS.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Funding
The study received support grants from the Faculty of Medicine, Khon Kaen University and Research and Graduate Studies, Khon Kaen University, Thailand.
Author Contributions
Study design: YK, PP; measurement: YK, PP, TW, NS, PH; data analysis: YK, PP; drafting manuscript: YK, PP; critical revision and final approval of the version to be published: all authors.
Acknowledgements
We thank (1) the patients, (2) the Department of Orthopedics and the Faculty of Medicine for their support, and (3) Mr. Bryan Roderick Hamman under the aegis of the Khon Kaen University Publication Clinic for assistance with the English language presentation of the manuscript.