Conservative Treatment and Unfavorable Factors to Bone Healing of “Pre-lysis”-Stage Lumbar Spondylolysis in Adolescents
Article information
Abstract
Study Design
Retrospective cohort study.
Purpose
To evaluate the clinical outcomes of the conservative treatment of “pre-lysis”-stage lumbar spondylolysis.
Overview of Literature
With the widespread use of magnetic resonance imaging (MRI) for early diagnosis of lumbar spondylolysis, a new disease stage called pre-lysis has emerged, in which intensity change is observed only on MRI without a fracture line on computed tomography. This study aimed to evaluate the clinical outcomes and factors unfavorable to bone healing of the conservative treatment of pre-lysis-stage lumbar spondylolysis.
Methods
Fifty-three patients with 57 fresh pre-lysis-stage lesions who had completed conservative treatment were included in the study (40 men, 13 women; mean age, 14.3 years). We investigated the rate of bone healing and the relationship between bone healing after conservative therapy and factors such as age, sex, vertebral level, unilateral/bilateral lesions, and presence of spina bifida occulta.
Results
The overall bone healing rate was 95% (54/57 lesions). Bilateral lesions had a significantly lower bone healing rate than unilateral lesions (86% vs. 100%, p=0.046). There were no statistically significant differences based on age, sex, vertebral level, or presence of spina bifida occulta.
Conclusions
The bone healing rate in unilateral lesions was 100%, which was significantly higher than that in bilateral lesions. It is important to detect and initiate treatment while the lesion is still unilateral, if possible.
Introduction
Lumbar spondylolysis is a common fatigue fracture in adolescent athletes. The first line of treatment is conservative therapy, which includes rest and a brace [1,2]. In the past, staging with axial computed tomography (CT) slices was common and influenced the outcome of conservative treatment [3]. Recently, Sairyo et al. [4] reported and popularized the early diagnosis of lumbar spondylolysis based on high-intensity changes within the pedicle in short tau inversion recovery (STIR) of magnetic resonance imaging (MRI).
With the widespread use of MRI for early diagnosis of lumbar spondylolysis, a new stage has emerged in which intensity change is observed only on MRI without a fracture line on CT. This stage is even earlier than the traditional “early stage” and called the “pre-lysis” or “very early” stage, as proposed by Tatsumura and others [5,6]. Pre-lysis lesions have a bone healing rate of nearly 100% with conservative treatment; however, there are few reports on their characteristics and conservative treatment outcomes [6–8]. This study aimed to evaluate the clinical outcomes and factors unfavorable to bone healing of the conservative treatment of pre-lysis-stage lumbar spondylolysis.
Materials and Methods
In our study, we retrospectively investigated 441 high school students or younger patients diagnosed with lumbar spondylolysis in Tsukuba University Hospital Mito Clinical Education and Training Center/Mito Kyodo General Hospital between April 2014 and March 2020. All patients were symptomatic with predominantly low back pain, and no asymptomatic patients were included. Because most patients are referred to our hospital by their primary care physicians for a comprehensive adolescent examination, MRI is used in all cases, except those involving obvious trauma, as it has previously been reported to be useful for early diagnosis and prevention of missed lesions [4,9]. Furthermore, in cases where MRI shows high-intensity changes within the pedicle, CT is performed because bone fusion rates in lumbar spondylolysis vary greatly depending on the stage (e.g., 94% in early stage, 80% in progressive stage, and 0% in terminal stage), and stage diagnosis can only be performed by CT, as many reports have shown [1,3,5,7,8,10,11].
The exclusion criteria excluded the following: 42 patients who were transferred to another hospital during treatment, 16 patients with missing data, 122 patients who dropped out (including 23 patients with pre-lysis-stage lesions), and 208 patients with early-, progressive-, and terminal-stage lesions other than those in the pre-lysis stage.
Finally, the study included 53 patients with 57 fresh pre-lysis-stage lesions who had completed conservative treatment (40 men, 13 women; mean age, 14.3 years,). All patients underwent CT and MRI scans. In this study, pre-lysis was defined as a lesion on STIR MRI with high-intensity changes due to bone marrow edema within the pedicle but no fracture line on CT or T1 weighted image [5] (Fig. 1). There was one case of recurrence after conservative treatment, and all patients were athletes who participated in sports on a daily basis. There were five patients with multilevel lesions, including lesions outside of the pre-lysis stage, but the pre-lysis-stage lesions were all confined to one level. There were 36 patients with unilateral lesions and 17 with bilateral lesions. Of the 17 patients with bilateral lesions, four had pre-lysis-stage lesions on both sides, and 13 had early-, progressive-, or terminal-stage lesion on the contralateral side. All patients and their parents provided informed consent to participate in this study. This study was approved by the institutional review board of Tsukuba University Hospital Mito Clinical Education and Training Center/Mito Kyodo General Hospital (no., 17–01).
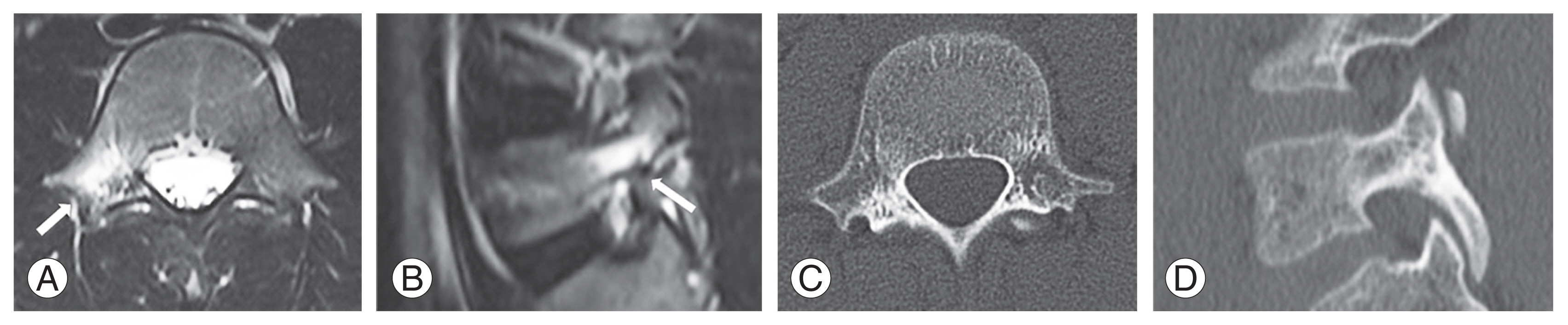
Definition of “pre-lysis” stage. “Pre-lysis” was defined as a lesion with high intensity changes on magnetic resonance imaging (arrow, A, B) without a fracture line on computed tomography (C, D).
We also evaluated factors reported to affect bone healing, such as age (divided into three groups: elementary school patients, junior high school patients, and high school patients), sex, vertebral level, unilateral or bilateral presentation, and the presence or absence of spina bifida occulta at the time of the initial examination [3,5,7,8,10]. In this study, we investigated the rate of bone healing and the relationship between bone healing and each factor after conservative therapy.
For all patients, the conservative treatment protocol was to wear a hard Knight-type plastic brace and refrain from exercising, including physical education and physical therapy [5]. MRI was used to assess the intensity change within the pedicle once a month during conservative treatment [5,7]. When the intensity change on STIR MRI disappeared, CT was performed to evaluate bone healing. Because pre-lysis is defined as the absence of a fracture line, bone healing was defined in this study as (1) no fracture line visible and (2) incomplete fracture line visible but bone continuity preserved. A fracture line that appeared after conservative treatment but did not show bone continuity was deemed to have failed to achieve bone healing. CT images were evaluated by two orthopedic surgeons. Differences in evaluation were discussed before making the final decision. The duration of conservative treatment was defined as the period from the date of diagnosis until the high-intensity changes disappeared on STIR MRI.
The relationship between age group, sex, vertebral level, unilateral/bilateral presentation, and presence of spina bifida occulta with bone healing was analyzed statistically using Fisher’s exact test. Welch’s t-test was performed for the statistical analyses of the duration required for bone healing. The significance level was set to p<0.05. SAS JMP ver. 10.0 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis.
Results
The bone healing rate for all lesions was 95% (54/57 lesions) in 50 patients. Three lesions (5%) in three patients did not achieve bone healing (Table 1). The average duration of conservative treatment was 96 days: 96 days for the 50 patients who achieved bone healing and 90 days for the three patients who did not. There was no statistically significant difference (p=0.81).
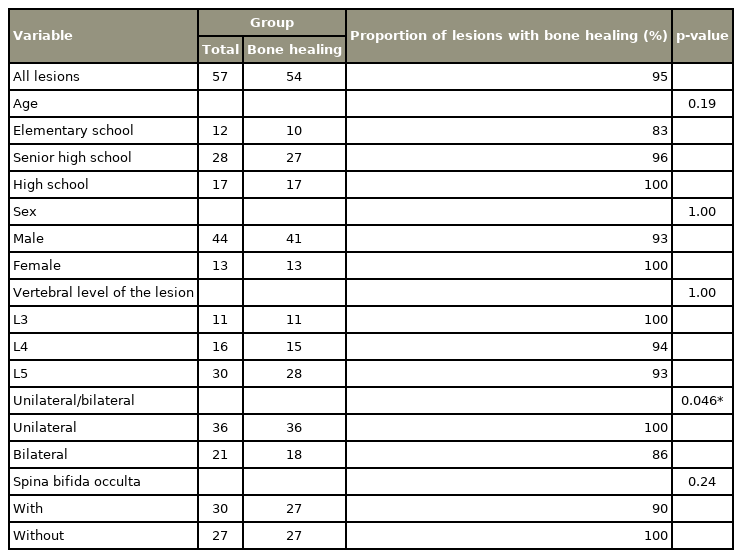
Proportion of “pre-lysis”-stage lesions with bone healing in each factors
The bone healing rate by age was 83% for elementary school, 96% for junior high school, and 100% for high school patients, with no significant difference between the three groups (p=0.19). The bone healing rate by sex was 93% for male and 100% for female patients, with no statistically significant difference (p=1.00). The bone healing rate by vertebral level was 100% for L3, 94% for L4, and 93% for L5, with no significant difference among vertebral levels (p=1.00). There were 36 unilateral lesions and 21 bilateral lesions. Bilateral lesions had a significantly lower bone healing rate than unilateral lesions (86% versus 100%, p=0.046). The bone healing rate with and without spina bifida occulta was the same (90% versus 100%, p=0.24). The following are some examples of illustrative cases (Figs. 2, 3).
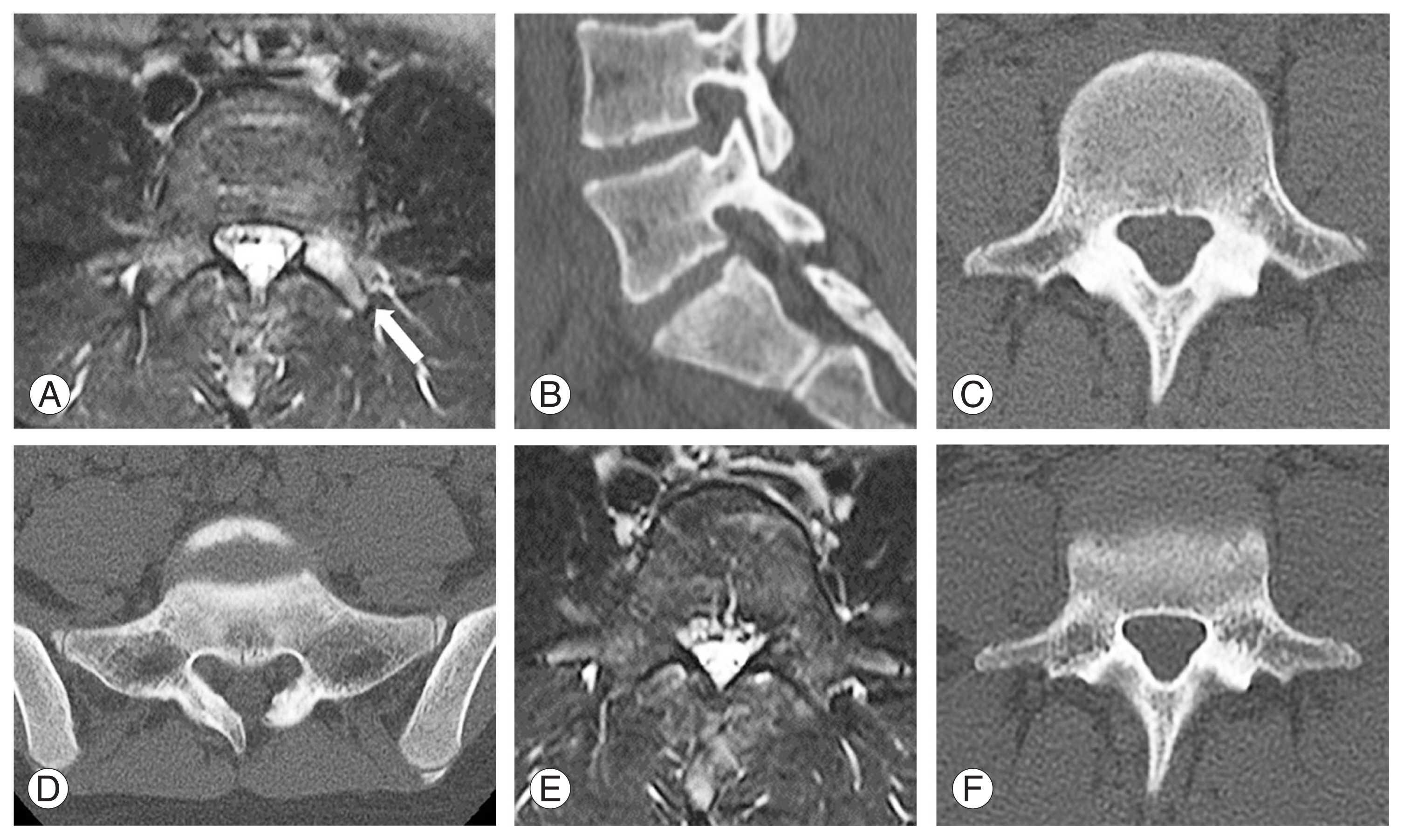
Illustrative case 1. Case of unilateral lesion. An 11-year-old girl who plays badminton presented with a chief complaint of low back pain that had been present for two weeks. The pain intensified with extension of the lumbar spine. Magnetic resonance imaging (MRI) showed intensity changes in the left pedicle of L5 (A, arrow). computed tomography (CT) showed no obvious fracture line and revealed spina bifida occulta of the sacrum (B–D). She was diagnosed with left L5, “pre-lysis”-stage lumbar spondylolysis, and conservative treatment was performed. After 2 months of conservative treatment, the MRI intensity change disappeared, and no fracture line appeared on CT (E, F). We considered that the lesion achieved bone healing and allowed her to return to sports. She has continued to play badminton without any back pain.

Illustrative case 2. Case of bilateral lesion. A 12-year-old boy who played judo presented with worsening of his low back pain over the previous month. Magnetic resonance imaging showed intensity changes in the bilateral pedicle of L5 (A). Computed tomography scans showed no fracture line on the right, a hair line fracture on the left and spina bifida of the sacrum (B–E). He was diagnosed with bilateral L5 lumbar spondylolysis. The right lesion was in the pre-lysis stage (B, C), and the left lesion was in the early stage (B, D). After 2 months of conservative treatment, the lesions became pseudoarthrosis (F: axial plane, G: sagittal plane of right side, H: sagittal plane of left side). Back pain was improved, and he was able to return to judo. He has been followed clinically as he continues with judo.
Discussion
Many risk factors for bone healing have been reported in the conservative treatment of adolescent lumbar spondylolysis, including progressive, L5, bilateral, and contralateral terminal-stage lesions [3,5,10,11]. Many reports describe lesions that do not respond well to conservative treatment, such as progressive-stage lesions with a contralateral terminal-stage lesion [10,11]. In contrast, there have been few reports of lesions with good outcomes and lesions with consistent bone healing.
Recently, MRI has become widely used for the early diagnosis of lumbar spondylolysis [4]. Among these, pre-lysis-stage lesions, involving bone marrow edema or a stress reaction have been proposed as a preliminary stage of fracture when no fracture line is observed on CT but intensity changes are apparent on MRI. In these cases, the bone healing rate has been reported to be nearly 100% [1,5–8]. However, no detailed studies of pre-lysis-stage lesions have been reported.
We focused on the new concept of pre-lysis in this study, evaluating its characteristics and the clinical outcomes of the conservative treatment of pre-lysis-stage lumbar spondylolysis.
The concept of a pre-lysis-stage lesion arose from the widespread use of MRI for early diagnosis of bone fractures, which was previously unknown when fractures were diagnosed via X-ray or CT. Early diagnosis with MRI allows for early treatment at a stage with high bone healing rates. MRI also detects more L3 and L4 lesions than L5 lesions [9]. In general, the percentage of L5 in lumbar spondylolysis cases is 90% in adults and 65%–85% in adolescents [3,5,12]. L5 lesions accounted for 53% of the cases in this study, whereas L3 or L4 lesions accounted for 47%, which is a higher percentage of L3 or L4 lesions than previously reported [3,5,12]. It is also possible that MRI imaging enabled the extraction of more L3 or L4 lesions than in the past. This means that L3 or L4 lesions may be more common in the pre-lysis stage. The proportion of pre-lysis-stage lesions and non-L5 lesions is expected to increase in the future as MRI imaging becomes more widely used for early diagnosis.
In this study, the bone healing rate of pre-lysis-stage lesions was 95%, with 5% of the lesions failing to heal. Bilateral lesions have been reported as a risk factor for conservative treatment in previous studies involving all stages of the disease [3,5,11]. Even in pre-lysis-stage lesions, the bone healing rate in bilateral lesions is lower than in unilateral lesions. Consequently, the possibility of bilateral lesions should always be assessed.
In contrast, pre-lysis stage and unilateral lesions had 100% bone healing. The bony ring structure of the spinal canal has been proposed as a mechanism that influences bone healing [8,13]. The pre-lysis-stage lesion without a fracture line was stable without disruption of the ring structure if it was a unilateral lesion, indicating the possibility of achieving bone healing without the development of a cortical bone fracture.
According to previous reports, a terminal-stage lesion on the contralateral side of a fresh lesion is common [10,11]. This demonstrates that based on the timeline, the unilateral lesion progresses to the terminal stage, and then a fresh lesion develops on the contralateral side. Furthermore, conservative treatment has a very poor outcome in cases of the contralateral terminal-stage lesion [8,10,11]. We believe that treating the initial unilateral lesion is critical for preventing such cases. It is important to detect and start treatment at the pre-lysis-stage by performing MRI early in patients with low back pain, preferably while the lesion remains unilateral.
There are several limitations in this study. All patients were treated under strict protocols, and 122/441 patients (28%) dropped out. In particular, there were 23 patients of dropout in the pre-lysis-stage lesions. This is a significant percentage, and it is possible that the proportion of lesions that healed in this study may be higher than the actual proportion in the rest of the population because patients with good adherence to treatment were included in the analysis, and the results in this study may be limited. Furthermore, the findings of this study were obtained from a single protocol at a single hospital in a limited area of Japan. The conservative treatment protocol in this study included monthly MRI examinations. Some insurance policies may cover monthly MRI examinations, and because the patients in this study are under the age of 18 years, they may also be eligible for medical expense subsidies. The patients’ and families’ financial burden was minimal. We believe that monthly MRI examinations are important in determining the time of return to sports. However, healthcare costs vary by country, and we would recommend routine monthly MRI examinations in the clinical setting if possible. Given some of the points raised above, it is prudent to question whether the findings of this study can be applied to all patients.
Conclusions
In this study, the proportion of pre-lysis-stage lesions with bone healing after conservative treatment in this study was 95%. The bone healing rate in unilateral lesions was 100%, which was significantly higher than that in bilateral lesions. Therefore, it is critical to detect and initiate treatment while the lesion remains unilateral if possible.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
HG and MT conceived and designed the study; SO gathered and analyzed the data; HG and MT drafted the paper; MY significantly revised the drafted paper; and all the authors gave final approval of the version submitted for publication.