Comparison of Korean Body Image Questionnaires in Adolescent Idiopathic Scoliosis
Article information
Abstract
Study Design
A prospective study.
Purpose
To obtain the results of four body image questionnaires analyzed for validity in Korean and compare them to radiographic findings and quality of life scores.
Overview of Literature
Each of the four body image questionnaires has been studied, but comparative studies of each other are rare.
Methods
Adolescent idiopathic scoliosis (AIS) patients ages 10 to 19 years completed the Korean version of the Quality of Life Profile for Spinal Deformities (K-QLPSD), the Scoliosis Research Society-22 self-image subscale (K-SRS-22-si), Korean version of the Spinal Appearance Questionnaire (K-SAQ), Korean version of the Body Image Disturbance Questionnaire-Scoliosis (K-BIDQ-S), and Korean version of the Italian Spine Youth Quality of Life (K-ISYQOL). Four body image questionnaires were compared with K-ISYQOL and radiographic major curve magnitude, coronal balance, and sagittal balance. Spearman’s correlation was performed to compare the four body image questionnaires.
Results
The study included 84 AIS patients, with a mean age of 12.6 years and a major Cobb angle of 29.4°. The four surveys were correlated with major curve magnitude and K-ISYQOL. K-SAQ and K-BIDQ-S were correlated better than K-QLPSD, and K-SRS-22-si was correlated with K-ISYQOL. The four surveys were moderately correlated with major curve magnitude, but there was no correlation with age, coronal balance, and sagittal balance.
Conclusions
K-SAQ and K-BIDQ-S correlate better with K-ISYQOL than K-QLPSD and K-SRS-22-si.
Introduction
Adolescent idiopathic scoliosis (AIS) is a complicated deformity characterized by shoulder imbalance, protrusion of the ribs, trunk shift, and anterior chest deformity [1–4]. Thus, body image disturbance is associated with the health-related quality of life (HRQOL) and other related factors among AIS patients and their parents. Consequently, the perception of body image in AIS has been evaluated by various patient-reported outcome measures. Among them, the Quality of Life Profile for Spinal Deformities (QLPSD) [5], the Scoliosis Research Society-22 self-image subscale (SRS-22-si) [6], the Spinal Appearance Questionnaire (SAQ) [7], and the Body Image Disturbance Questionnaire-Scoliosis (BIDQ-S) [8] are frequently used for measuring body image disturbance.
SRS-22 is the most common reassure of quality of life (QOL) in scoliosis. However, the recently reported Italian Spine Youth Quality of Life (ISYQOL) showed better validity than SRS-22 in measuring HRQOL in adolescents with spinal deformities [9].
This study aimed to evaluate the relationship between the instrument scores and the curve magnitude because the Cobb angle is generally recognized as the gold standard in measuring disease severity. This study also aimed to determine the relationship between these four body image instruments and the other HRQOL [10]. (The Korean version of ISYQOL is the standard instrument used for this purpose.)
Materials and Methods
Eighty-four AIS patients ages 10–18 years old who visited the orthopedic outpatient clinic between 2019 January and May 2020 were included prospectively for this research (Fig. 1). The study was approved by the clinical research ethics committee of the Pusan National University Hospital (IRB no., 1909-001-082). Documented informed consent was obtained from all participants and their parents. The study inclusion criteria were AIS patients with a Cobb angle of >20°. Patients receiving any surgical treatment for scoliosis were excluded from the study. Patients with a history of congenital deformity, neuromuscular disease, endocrine disease, skeletal dysplasia, connective tissue abnormality, or mental retardation were excluded from the study. Demographic and radiographic findings, including age, sex, history of brace wear, major curve magnitude, coronal balance (mm), and sagittal balance (mm) during the visit, were examined.
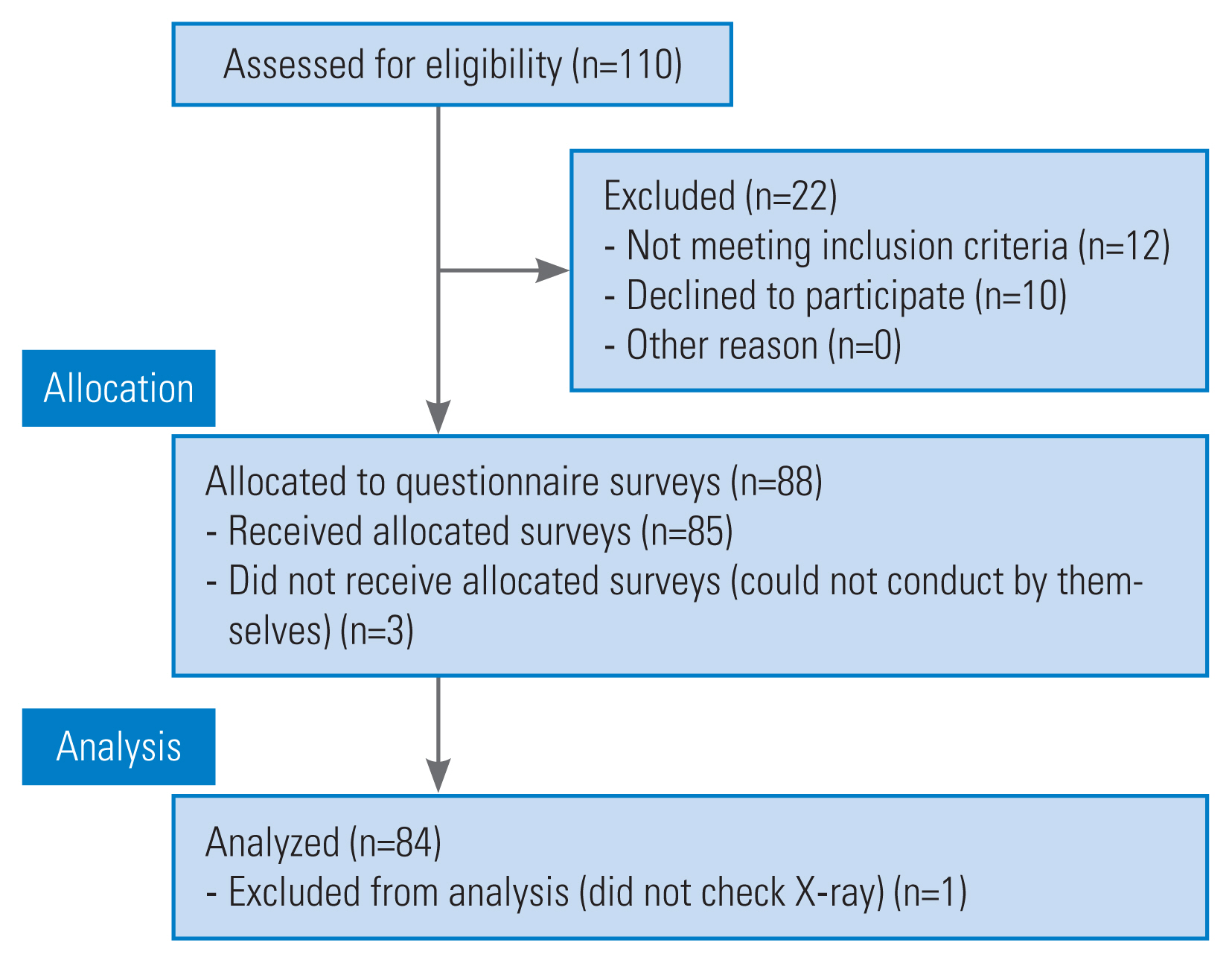
Flow diagram of enrollment.
A standard standing whole-spine anteroposterior radiograph was taken for each AIS at the first presentation. A standard technique was used for the measurement of Cobb’s angle. If more than one curve were found, the more severe curve would be selected for measurement. AIS patients who had curves of >20° were included. Coronal balance was defined as the width between the central sacral vertical line and the mid-C7 vertebra plumb line. Sagittal balance was defined as the horizontal distance between the C7 plumb line and the posterosuperior corner of the sacrum.
On the day of the visit, all patients completed the Korean version of QLPSD (K-QLPSD), Korean version of SRS-22 (K-SRS-22), Korean version of SAQ (K-SAQ), Korean version of BIDQ-S (K-BIDQ-S), and Korean version of ISYQOL (K-ISYQOL). Questionnaire surveys were administered with paper forms and conducted by the patients without assistance. X-ray measurement was completed without any information on the questionnaire scores.
K-QLPSD was validated to assess HRQOL in AIS [11]. The questionnaire contained 21 items grouped into five dimensions: psychosocial functioning, sleep disturbances, back pain, body image, and back flexibility. K-QLPSD-body image evaluated the body image of AIS and included four items (Appendix 1). The possible answers consisted of a typical five-level Likert item ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). The score was calculated as the sum or average of the answers to each question. A higher score indicated better QOL, and a lower score indicated poor QOL.
SRS-22 was designed by Asher et al. [6] to assess the outcome of AIS and was translated into Korean [12]. K-SRS-22 contained 21 items belonging to five dimensions: function/activity, pain, self-image, mental health, and satisfaction with treatment. K-SRS-22-si contained five items (Appendix 2). Each question was answered using a typical five-level Likert scale from 1 (“worst”) to 5 (“best”). The score was also calculated as the sum or average of the answers to each question.
SAQ was created and validated by Sanders et al. [7] based on the Walter Reed Visual Assessment Scale to assess patients’ self-perceptions and parents’ perceptions. It contained standardized drawings that demonstrate the severity levels of several components of spinal deformity and questions that allow the rating of dissatisfaction with aspects of the appearance. K-SAQ contained 20 items [13] (Appendix 3). K-SAQ scores ranged from 1 (“best”) to 5 (“worst”). The surgical scar domain and three items about the most bothersome deformity were not included for calculating K-SAQ scores because no patient had previously received any surgical treatment. Thus, the questions were deemed unsuitable for scoring.
BIDQ-S was created and validated by Auerbach et al. [8] Based on the modifications of the Phillips’ Body Dysmorphic Disorder Questionnaire [14], BIDQ-S was developed to assess appearance concerns and related distress and impairment in daily functioning. K-BIDQ-S also was validated [15] (Appendix 4). K-BIDQ-S contained seven items, including appearance-related concerns; corresponding mental preoccupation; associated experiences of emotional distress; resultant impairment in social, occupational, or other important areas of functioning; interference with social life; interference with school, job, or role functioning; and consequent behavioral avoidance. Each item was rated from 1 (“not at all concerned”) to 5 (“extremely concerned”). The average of the seven results was the K-BIDQ-S total score.
ISYQOL was developed using Rasch’s analysis to measure QOL in spine deformity patients during growth [16]. Designed in Italy, ISYQOL has been translated and validated for use in English. Recently, the validated K-ISYQOL consisted of 20 items scored on three categories rated from 0 (“best”) to 2 (“worst”) (Appendix 5). Seven K-ISYQOL items assessed the impact of bracing on QOL and were administered only to patients wearing the brace. The seven items about bracing were not included for calculating K-ISYQOL scores in patients who did not wear a brace. Rasch’s analysis showed that ISYQOL offers a QOL measure fully complying with the requirements of a fundamental measure.
The Shapiro-Wilk test was used to determine whether data were normally distributed. Spearman’s r was used for all continuous variables; point-biserial correlations were used between continuous and categorical data. A correlation (r) of 0–0.29 was considered weak correlation strength, 0.30–0.69 was moderate, and 0.70–1.0 was strong [17]. The Mann-Whitney U test was used to determine the difference of means. A priori power analysis was conducted for two-tailed Spearman’s r with a moderate effect size (q=0.3), 0.05 alpha error, and 0.80 power. The necessary sample size was 82 surveys (G*Power ver. 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany; http://www.gpower.hhu.de/) [18].
Results
The study included 84 AIS patients, with a mean age of 12.6 years, and 71 (84.5%) of them were females (Fig. 1). The average major Cobb angle was 30.0° (Table 1). The majority of the curves were thoracic. The curve types of the final enrolled participants were Lenke type 1 (n=56), type 2 (n=2), type 3 (n=15), type 5 (n=9), and type 6 (n=2).

The demographic characteristics of the study population
The mean questionnaire scores for body image and QOL surveys are shown in Table 2. Correlations between the four body image questionnaires, demographic measurements, radiographic measurement, and QOL survey are shown in Table 3. The four body image questionnaire surveys correlated with major curve magnitude and K-ISYQOL, including total, physical, and mental functions. Overall, K-SAQ and K-BIDQ-S were correlated better than K-QLPSD and K-SRS-22-si, with more strong correlations and a higher correlation with K-ISYQOL and major curve magnitude. K-SAQ and K-BIDQ-S had a similar correlation with major curve magnitude, body image questionnaire, and K-ISYQOL, including total, physical, and mental functions. To highlight the comparison, K-SAQ and K-BIDQ-S strongly were correlated with each other (r=0.748), and K-SAQ and K-BIDQ-S had strong correlations with the K-ISYQOL total score. The four body image questionnaires were moderately correlated with major curve magnitude, but there was no correlation with age, coronal balance, and sagittal balance for the four body image questionnaires. The best moderate correlations with the radiographic parameter were major curve magnitude to K-BIDQ-Q (r=0.482).

The scores of body image questionnaire and K-ISYQOL

Correlations of questionnaire scores
Data were divided into two groups based on major curve magnitude (<45° and >45°). There was a significant difference in the mean scores for questionnaire surveys, with the >45° group showing worse on all body image and QOL scores (Table 4). However, no improvement was found in correlations between the four body image questionnaires, demographic measurements, radiographic measurement, and QOL survey after dividing into the major curve magnitude groups (Table 5).

The mean scores of major curve magnitude below and above 45°
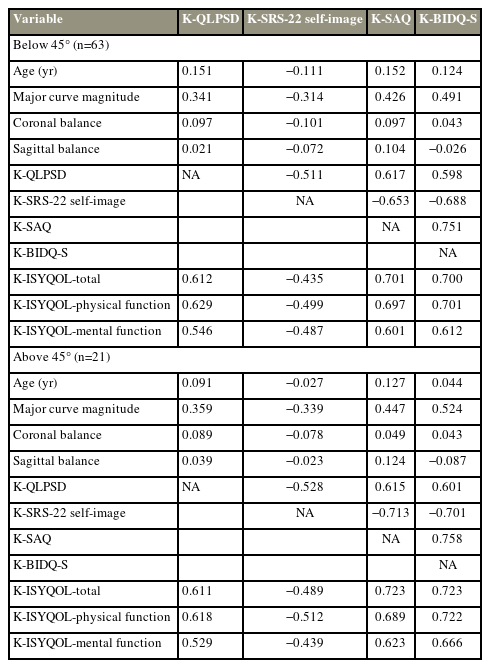
Correlations of two groups based on major curve magnitude below and above 45°
Discussion
In this study, K-SAQ and K-BIDQ-S were correlated better with K-ISYQOL than K-QLPSD and K-SRS-22-si. Moreover, K-SAQ and K-BIDQ-S were strongly correlated with each other (r=0.748), and K-SAQ and K-BIDQ-S had strong correlations with the K-ISYQOL total score. The four body image questionnaires were moderately correlated with major curve magnitude, but age, coronal balance, and sagittal balance were correlated poorly with other surveys. Data were analyzed by dividing them into two groups: <45° and >45°. Data were divided into two groups based on 45° to consider that the clinical results at <45° remained steady as in Parent et al. [19], but it deteriorated significantly at >45°. In this study, the HRQOL of the >45° group was significantly worse. However, there was no difference in the correlation between major curve magnitude and body image surveys in the two groups.
Four body image questionnaires have been studied individually but rarely compared to each other. In general, the survey scores were quite similar to previous studies that examined these surveys individually [5–8]. Regarding the correlation between body image questionnaire and major curve angle, this cohort’s correlations of K-BIDQ-S and K-SAQ were also similar to previous studies [7,8,13,15,20]. Still, no strong correlation was found between the two body image surveys and major curve angles. The sex distribution of this study population aligned with general population studies with a 5.4:1 girl/boy AIS ratio for a Cobb angle of >20° [21]. However, the sex ratio did not correlate with the four body image questionnaires.
Although several QOL surveys exist, this study used one general health survey (K-ISYQOL). ISYQOL is a valid measure of HRQOL in young people with a spinal deformity. Moreover, ISYQOL observed better validity than SRS-22 to measure HRQOL in AIS [9].
These data can be difficult to interpret without a single standard against which body image surveys will be compared. When radiographic findings were as the standard, neither of the body image surveys used performed well, nor did ISYQOL. K-ISYQOL was moderately correlated with major curve magnitude (r=0.303). The larger the curve was, the worse was the body image of QOL. A higher correlation between larger curve size and body image was expected, but no correlation was found, in line with a previous study [20].
Before interpreting these results, several limitations were considered. First, the number of patients recruited was relatively small. Second, the subjects were AIS patients with a Cobb angle of >20° recruited at one spine center and were a convenient sample, not randomly selected. Moreover, patients receiving any surgical treatment for scoliosis were excluded from the study. Thus, this cohort may not have been representative of all patients with AIS. Accordingly, the generalizability of the QOL scores was limited. Third, this study did not include body mass index, history of mental condition, and factors affecting body image. Fourth, other body image questionnaires with different languages were excluded because the study was conducted only with the Korean version of the validated questionnaire.
Conclusions
This study compared four body image questionnaires for AIS commonly used in several studies to detect body shape and its associated QOL. Body image is a complex problem in AIS and has no linear correlation with their spinal deformities. None of the four body image questionnaires showed superiority in association with radiographic spinal deformity, but K-SAQ and K-BIDQ-S showed a superior correlation with K-ISYQOL than K-QLPSD and K-SRS-22-si.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Funding
This work was supported by a 2-Year Research Grant of Pusan National University.
References
Appendices
Appendix 1.
Korean version of the quality of life profile for spinal deformities
asj-2021-0460-Appendix-1.pdfAppendix 4.
Korean version of the Body Image Disturbance Questionnaire-Scoliosis
asj-2021-0460-Appendix-4.pdfAppendix 5.
Korean version of the Italian Spine Youth Quality of Life Questionnaire
asj-2021-0460-Appendix-5.pdf