Cortical Trajectory Screw Fixation in Lumbar Spine Surgery: A Review of the Existing Literature
Article information

Abstract
Posterior lumbar fusion is a safe and effective surgical method for diseases, such as lumbar stenosis, spondylolisthesis, lumbar instability, spinal deformity, and tumor. Pedicle screw (PS) fixation was first introduced by Bouche and has been adopted as the gold standard for posterior lumbar fusion. Santoni and colleagues introduced a new methodological screw insertion technique that uses a cortical bone trajectory (CBT), described as that from a medial to lateral path in the transverse axial plane and caudal to the cephalad path in the sagittal plane through the pedicle for maximum contact of the screw with the cortical bone. Owing to the lower invasiveness, superior cortical bone contact, and reduced neurovascular injury incidence, the CBT technique has been widely used in posterior lumbar fusion; however, these advantages have not been proven in clinical/radiological and biomechanical studies. We designed the present study to review the existing evidence and evaluate the merit of CBT screw fixation. Six electronic databases were searched for relevant articles published in August 2020 using the search terms “cortical bone trajectory,” “CBT spine,” “CBT fixation,” “cortical pedicle screws,” and “cortical screws.” Studies were analyzed and divided into the following groups: “biomechanics investigation,” “surgical technique,” and “clinical/radiological studies.” Most studies compared CBT and PS fixation, and the CBT screw fixation method showed better or similar outcomes.
Introduction
Posterior lumbar fusion is a safe and effective surgical method for diseases, such as lumbar stenosis, spondylolisthesis, lumbar instability, spinal deformity, and tumor [1–3]. Pedicle screw (PS) fixation was first introduced by Boucher [4] and has been adopted as the gold standard in posterior lumbar fusion [4]. This technique had shown good biomechanical strength and properties [5], superior correction, and non-union rate in patients with spinal deformity; however, PS fixation is also associated with certain limitations, such as dural tears, cerebrospinal fluid leakage, increased neurological or vascular injury risk and superior facet joint violation, wide muscle damage, larger intraoperative blood loss, and longer incision due to its lateral to medial trajectory [6–10]. Moreover, the maximum screw misplacement rate of PS fixation was 40% despite the use of navigation techniques [11–13]. In particular, PS fixation showed screw loosening, correction loss, and non-union in the osteoporotic bone [14–16]. For more rigid fixation, various approaches, including the use of a different screw trajectory, have been presented with the focus of enhancing stability and preventing such complications [17]. The conventional pathway for the PS passes through the pedicle axis with a lateral to a medial path beginning at the cross line of the lateral border of the superior articular facet and line through the center of the transverse process (Fig. 1) [18]). In contrast, Santoni et al. [17] introduced a new methodological screw insertion technique via a cortical bone trajectory (CBT), described as that from medial to a lateral path in transverse axial plane and caudal to cephalad path in sagittal plane through the pedicle (Fig. 2) to secure greatest contact of the screw with cortical bone [19]. It may contribute to the stability in osteoporotic patients by increasing screw bone purchase unlike in PS fixation. Further, the medial starting point in the CBT screw fixation method involves minimal soft tissue dissection as compared with that in PS screw fixation and may lower the risk of neurovascular injury around the vertebrae. In the present review, we performed a comprehensive study of several articles to accumulate evidence regarding CBT screw fixation as an alternative technique in osteoporotic vertebrae for PS fixation.

Pedicle screw fixation (L4/5). (A, D) Entry point is cross line of lateral border of the superior articular facet and center of the transverse process. (B, E) Screw go through 15°–25° at transverse pedicle angle. (C, F) L4 and L5 sagittal pedicle angle is each 0°, 5°–10° caudally declined.
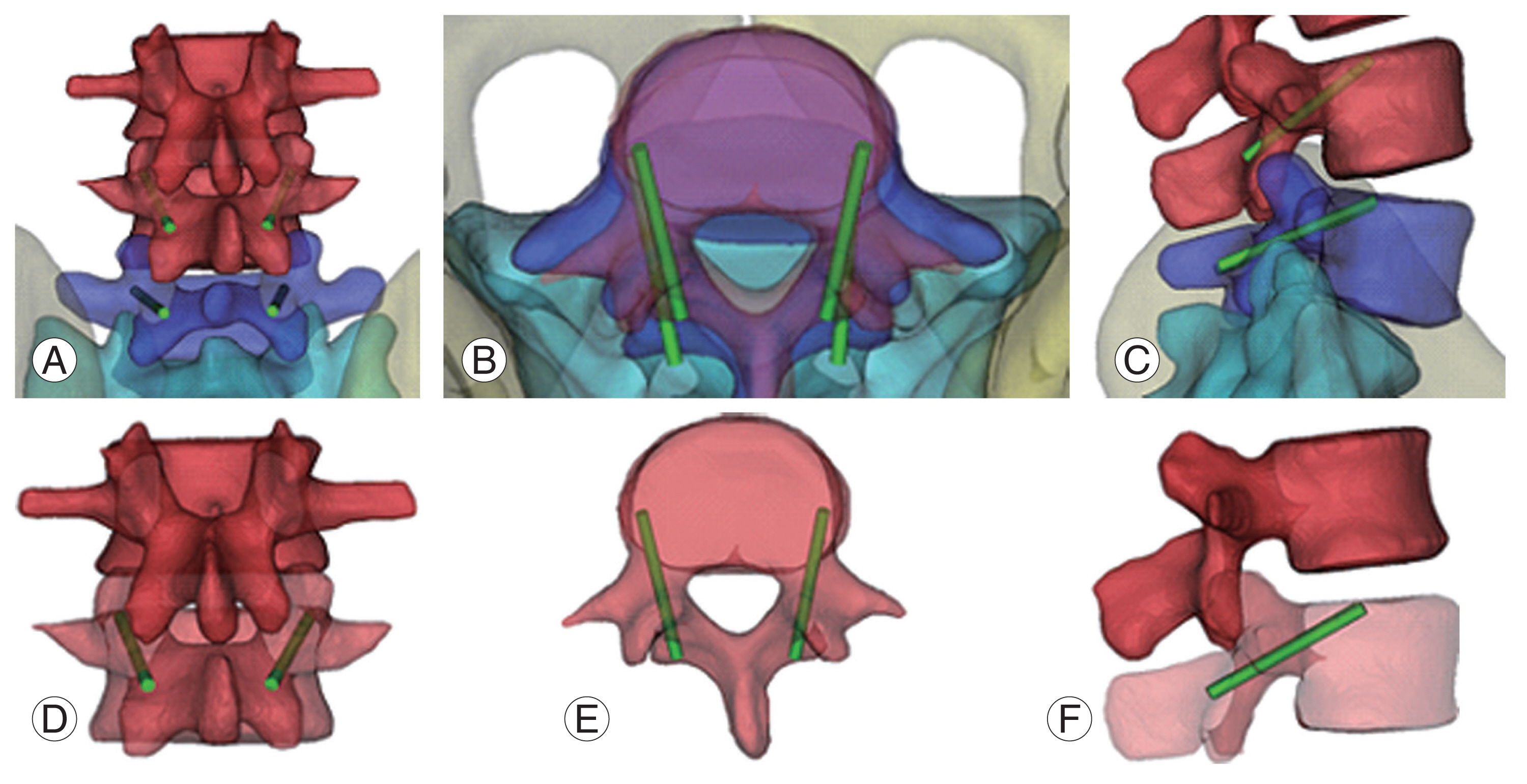
Cortical bone trajectory screw fixation (L4/5). (A, D) Starting point is junction of the center of the superior articular process and 1 mm inferior to the inferior border of the transverse process. (B, E) Screw go through pedicle at medio-lateral pathway in transverse plane. (C, F) 25°–30° caudocranial pathway in sagittal plane.
Methods
MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and SCOPUS electronic databases were searched for relevant articles published in August 2020 using the search terms “cortical bone trajectory,” “CBT spine,” “CBT fixation,” “cortical pedicle screws,” and “cortical screws.” Studies were analyzed and divided into the following groups: “biomechanics investigation,” “surgical technique,” and “clinical/radiological studies.” Full text articles and abstracts were included in the present review, whereas editorials and commentary texts were excluded.
Biomechanical Characteristics
In order to overcome the disadvantages of PS fixation in the osteoporotic bone, Santoni et al. [17] devised a CBT screw technique wherein the screw is fixed from the medial to the lateral path in the transverse plane, caudal to the cephalad path in the sagittal plane through the pedicle (Fig. 1). CBT screw fixation increases the holding screw strength by increasing the screw bone purchase power via modification of the thread pitch and shape and minimization of loosening that it showed a pullout and toggle character commensurate with PS [17]. An in vivo study reported 1.7 times higher insertion torque in CBT as compared with that in PS [20]. Although the maximal insertional torque and the correlation coefficient of bone mineral density (BMD) in the CBT technique were smaller than those in the PS technique, the maximal insertional torque was larger in the CBT group relatively fixed to the cortical bone less affected by osteoporosis [20]. Moreover, a finite element study showed higher resistance to flexion and extension loading in the CBT method and superior resistance to lateral bending and axial rotation in the PS method, irrespective of BMD owing to the emanant and short lever arms structure of CBT [21]. In several biomechanical and clinical studies, the CBT technique has shown good mechanical properties in terms of higher pullout strength and insertional torque, with similar stability of the screw rod construct as that with PS fixation [22–25]. Another in vivo study demonstrated that the CBT screw is affected by technical factors, such as the cephalad angle and screw length within the lamina and BMD; therefore, an appropriate insertion angle of 25°–30° cranially along the inferior border of the pedicle with sufficient length in the vertebral body and maximum contact to laminar is ideal [26]. In an animal experiment, the CBT technique showed similar biomechanical fixation as PS although shorter screws with a smaller diameter were used [25]. A cadaver study showed that CBT screw fixation had higher insertional torque, pullout strength, fatigue resistance, and load for displacing screws in the osteoporotic bone than PS fixation [27]. This issue remains debatable in patients with spondylolisthesis. CBT fixation in spondylolisthesis showed similar pullout strength as that using PS fixation; however, CBT screw fixation has lower cortical bone contact in the posterior lamina and short lever arm, with lower vertebral fixation strength than PS fixation in all planes of motion [23]. As per a radiological study, no significant differences were noted in the loss of slippage between the CBT and PS groups [28]. A cadaveric study also showed similar results at a multilevel lumbar segment with low-grade spondylolisthesis between the two groups. CBT fixation may have at least comparable biomechanical characteristics in reference to PS fixation [17,20–25,27–33] (Table 1). Different results may be obtained, depending on the surgical method. The CBT and PS methods showed no significant differences in stability as assessed using the range of motion (ROM) test (flexion, extension, lateral bending, and axial rotation) in direct lateral interbody fusion (DLIF). When performing the axial rotation test, the PS group had less ROM than the CBT group in transforaminal lumbar interbody fusion (TLIF) support [31]. In DLIF, greater cage insertion is possible than in TLIF, ensuring better stability to resist bending force.
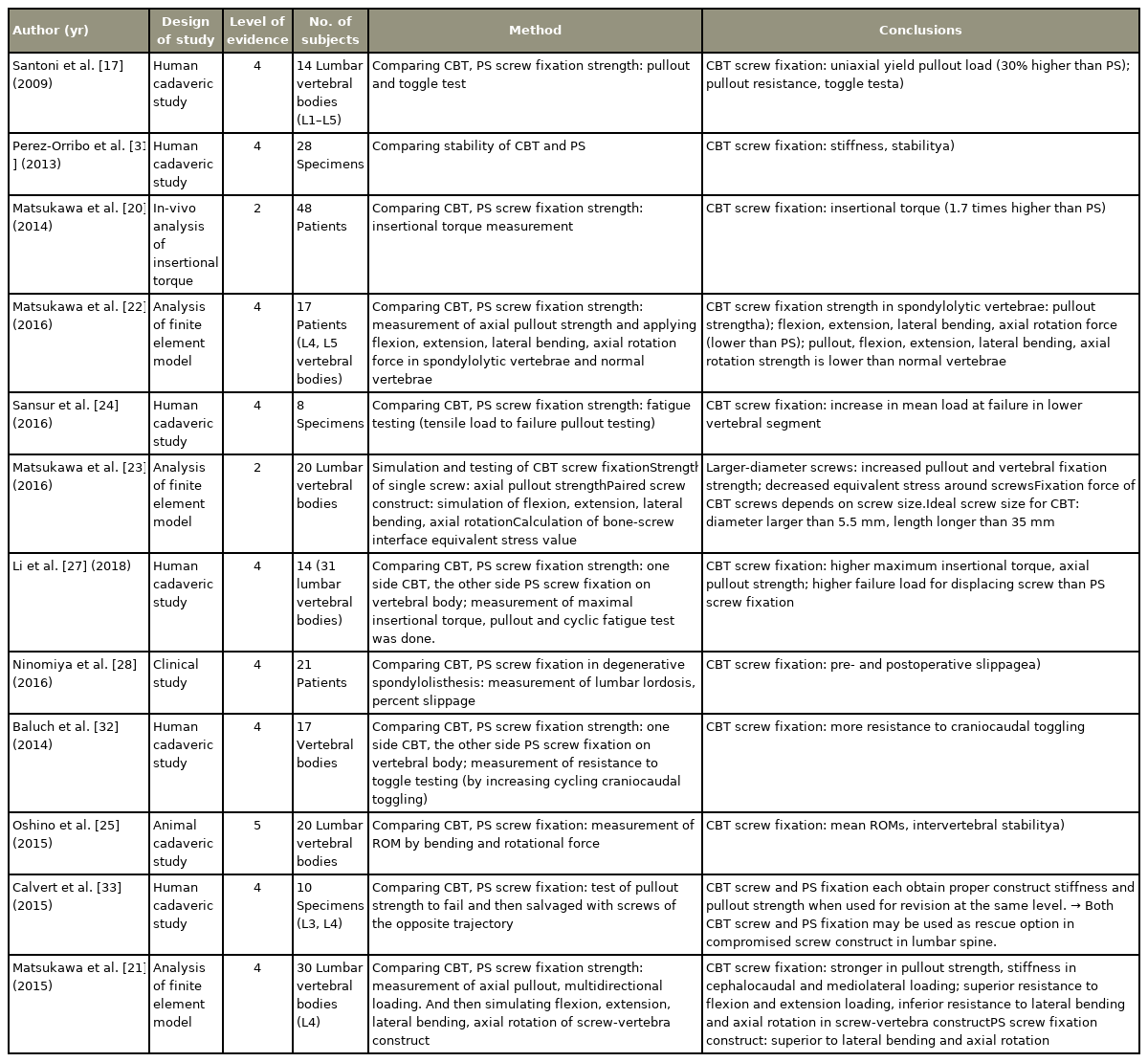
Characteristics of biomechanical studies
Surgical Techniques
First, Santoni et al. [17] introduced the new CBT that caudo-cephalad path in sagittal plane, mediolateral path in transverse plane for solid fixation to osteoporotic bone. Medio-latero-superior trajectory procedures for degenerative lumbar disease were proposed by Mobbs [34] with the use of a burr drill and proper tapping to prevent fracture of the pars, screw size, and rod diameter. In order to obtain detailed information about direction, screw size, and so on, Matsukawa et al. [19,20] performed morphometric measurement of the CBT. The starting point was defined at the junction of the center of the superior articular process and 1 mm inferior to the inferior border of the transverse process, at the 5 o’clock position of the left pedicle and 7 o’clock position of the right pedicle radiographically. In vivo analysis showed that the ideal cortical trajectory was dependent on technical factors in which 25°–30° cranially along the inferior border of the pedicle in sagittal plane to get maximum purchase with the lamina [26]. Other strength tests confirmed that the laterally directed cortical screws have superior resistance in the transverse plane [32]. Matsukawa et al. [26] performed fixation toward the posterior third to the posterior half of the superior endplate through a 25°–30° cranially and 10° laterally directed route. With respect to the size of the CBT screw, a three-dimensional (3D) finite element study showed that a screw larger than 5.5 mm and longer than 35 mm is appropriate for maximum contact to the lamina of the L4 vertebra [22]. Another morphometric study using computed tomography (CT) showed no significant difference between all pairs in terms of the maximum screw length in the axial plane; however, the maximum screw diameter in the axial plane showed a gradually increasing tendency from L1 to S1 of 4.8, 5.1, 6.1, 6.8, 8.0, and 6.1 mm, respectively [35]. A study of the anatomic variations in CBT screw placement using preoperative CT reported favorable screw location, trajectory, and length, with improved outcomes and reduced complications [36]. In particular, the anatomic variations in each patient disturb the conventional trajectory [37]. A cadaver study that aimed to verify the accuracy and safety of the CBT screw using 3D patient-matched guide or navigation showed satisfactory results [37–39]. Moreover, primary clinical description of patient-matched guide for CBT screw fixation study showed improved accuracy and reduced the risk of nerve damage and reduced radiation exposure [40–42].
Indications and Contraindications
Generally, CBT screw fixation can be used for most lumbar spine disorders except severe spondylolysis and spinal deformity [43]. On the basis of evidence, indications for CBT screw fixation are described as follows. In osteoporosis, diminished fixation strength and increased screw loosening because of compromised trabecular bone are observed [16]. Osteoporotic changes have a greater effect on the cancellous bone than on the cortical bone. As PS fixation inserts screw anatomic axis of pedicle and depends on its stability with cancellous bone, CBT screw fixation firmly secures its contact between the screw thread and the cortical bone. In case of obese patients with a larger incision, minimally invasive surgery using the CBT technique is a good option because the medial starting point involves less muscle dissection [43]. Moreover, evaluation of the damage to the paraspinal muscle using CT scan indicated that the CBT technique was associated with less fat infiltration ratio, indicating less soft tissue injury [44]. As the CBT starting point on the pars interarticularis site that does not invade the superior facet joint [43], CBT screw fixation can lower the facet joint violation rates. This is in keeping with the result that CBT screw fixation significantly reduces symptomatic adjacent segment degeneration (ASD) and radiologic ASD as compared with PS fixation [45–47]. One of the reasons is that caudomedial entry point enables a reduction in the dissection of the superior facet joints [48]. Moreover, symptomatic ASD or screw failure with PS fixation requiring revision surgery can be indications for the use of the CBT technique. Thanks to different pathway of screw, CBT can be fixed and obtain proper stability without increasing screw size and length [33]. However, as per a meta-analysis, the revision rates in both the groups were comparable [49]. There are several contraindications for CBT screw fixation, and these contraindications have not been established [50]. Spondylolysis, described as a defect or stress fracture in pars interarticularis, should be excluded from indication [51]. CBT screw fixation depends on the force and stability on cortex of pars [52]. CBT is recommended in elderly patients with osteoporosis; however, elderly women and patients with spondylolysis with inadequate pars interarticularis should choose the surgical method, considering complications, such as screw loosening that may occur later [53]. In addition, the spondylolytic vertebra shows approximately 50% lower insertional torque (4.25 versus 8.24 in-lb [53]), 20% lower pullout strength, and 30%–40% lower vertebral fixation strength when compared with non-spondylolytic vertebra [22]. Other contraindication is severe spinal deformity with horizontal rotation. CBT screw fixation has a shorter trajectory; therefore, it does not have sufficient rotational stability to de-rotate the vertebra [16]. Moreover, congenital deformity of pars, narrow pars, lacks of cortical bone at pars due to wide decompression, iatrogenic pars fracture are contraindications. Regarding caudal fixation of S1, penetrating S1 endplate screw (PES) was presented [54]. The starting point of the PES is the intersection between the under 3-mm spot most endpoint of inferior articular facet of L5 and center line of L5/S1 articulating facet joint and the route is caudo-cephalad straight direction without convergence to infiltrate middle column of sacral endplate [54]. The PES is aimed at the lateral area of the sacrum with abundant trabecular bone for solid fixation; therefore, it showed higher insertional torque than that in the monocortical technique [55], was more resistant to loosening, and had higher pullout strength than S1-alar screws. The modified CBT screw technique in lumbosacral posterior lumbar interbody fusion (PLIF) showed a higher incidence of screw loosening at S1 than that in single-level fusion in spondylolisthesis. The entry point of the caudal screw was the medial margin of the pedicle on an articular surface of the superior articular process, and the track led from medial to lateral, parallel to the cephalad endplate [56].
Clinical and Radiological Outcomes
The clinical and radiological outcomes obtained using the CBT technique are similar to those achieved using PS fixation. As per a randomized control study [57], the fusion rates of both techniques were comparable (CBT 94.5% versus PS 91.4%, p>0.99) at 24 months postoperatively. Patient satisfaction at 1 month was higher in the CBT group than in the PS fixation group (63% versus 35%, p=0.03); however, the Visual Analog Scale (VAS) leg pain score, the Oswestry Disability Index, and short form-12 score were not significantly different between the two groups. There were no significant differences in terms of screw loosening, infection, and recurrent radiating pain between the groups; however, facet joint violation was significantly lower in the CBT group (0% versus 18%, p<0.01) [57,58]. Comparative studies showed better results in terms of perioperative pain and Japanese Orthopaedic Association (JOA) Back Pain Evaluation Questionnaire social life function scores at 1 month, with similar improvement in the JOA score [59]. Regarding complications, the prevalence of symptomatic adjacent segment disease was lower in the CBT group than in the PS group (3% versus 11%, p<0.05) [46,47]. Other studies have shown similar fusion rates, JOA scores, radiographic fusion, and intraoperative and postoperative complications in patients with osteoporosis, with lower rates of screw loosening (6.5% versus 28.13%, p=0.03) [60,61]. A systematic review and meta-analysis also showed less external bleeding loss, intraoperative muscle damage, and perioperative pain, with faster recovery to normal activities in the CBT group (Table 2) [29].

Outcomes of meta-analysis studies
Complications
Several studies have reported the intraoperative/postoperative complications [58,62,63]. Screw loosening, neurological deficits, infections, vascular injuries, cerebrospinal fluid leak due to dural laceration, wound dehiscence, urinary retention, and screw malposition were observed; however, but there were no differences in the complications between the CBT and PS groups. With respect to ASD, symptomatic ASD and patients who needed additional surgical intervention for ASD were higher in the PS group [45–47]. Furthermore, radiologic ASD increased in the PS-PLIF group owing to the risk of proximal facet joint violation that caused destabilization at the supra-adjacent segment. Pars interarticularis and pedicle fractures may occur in the osteoporotic bone when setting the starting point. A high-speed round burr drill can help in lowering the risk of pars fracture [34].
Clinical Application of the Cortical Bone Trajectory Technique
A 75-year-old woman with osteoporosis who had been taking bisphosphonate for 10 years presented with a complaint of low back pain radiating to both the extremities, accompanied by intermittent claudication that had persisted for 3 years and had aggravated 1 month previously. Conservative treatment (physiotherapy and medication) did not relieve her chief complaint. Imaging studies showed central stenosis involving L4/5. Considering patient age and bone quality, PLIF using CBT screw fixation method was performed. In order to reduce bleeding and muscle damage, we made a smaller incision (approximately 7 cm) and performed muscle dissection rather than PS screw fixation. Her back pain and neurogenic claudication reduced postoperatively. Preoperative and postoperative plain radiography and CT scans showed good CBT screw placement (Fig. 3).

(A, B) Preoperative L-spine anterior-posterior (AP), lateral X-ray. (C, D) Postoperative L-spine AP, lateral X-ray. (E, F) Intraoperative X-ray. (G–I) Postoperative computed tomography.
Discussion
Several surgical approaches have been introduced for posterior lumbar fusion. The most widely used PS screw fixation involves less contact with the higher-density cortical bone and requires a larger exposure to fix the screw. The invitation of CBT screws, some drawbacks of PS fixation may be reformed. Thinner threads and shorter screw design, pathway of CBT screws make greater contact and support pullout strength for stability in osteoporotic patients. Regarding the caudomedial entry point, the CBT screw can be placed more medially than the PS screw [64]. This involved less dissection of the facet joints and the paraspinal muscles. Minimization of muscle damage using the CBT method is related to less postoperative pain and good functional recovery with a shorter hospital stay [44]. Moreover, it can reduce the possibility of pedicle medial wall perforation, neural injury risk, and facet joint violation [30]. Accordingly, less blood loss and pain can be expected in the immediate postoperative setting [58], and other studies have revealed superior outcomes with the use of the CBT technique [49,65,66]. From the perspective of fusion rates, the two groups were not significantly different [49,65,67]; however, Sakaura et al. [47] reported higher fusion rates in the PS group. It could be attributed to stronger stiffness against axial rotation and lateral bending when TLIF fusion is performed with PS fixation [31]. The micromotion resulting from CBT fixation with weaker stiffness than that with PS might cause an early cyclic loading failure and influence the fusion rate [68]. When PS screw placement fails or the pedicle is too small for screw fixation, CBT screw fixation can also be used as a salvage method. Considering the advantages of the CBT technique, it can be an alternative to PS fixation; however, there is insufficient evidence from few long-term studies on the use of the CBT technique. In terms of complications, the CBT technique showed a lower overall incidence than PS fixation. Complications are predictable through entry point and trajectory of CBT technique. Preoperative imaging study can reduce the complications by predicting the pathway of the screws and spondylosis including pars interarticularis defect and checking bone density with BMD. Entry point and trajectory have not been defined well owing to the possibilities of being excluded severe degenerative change of the anatomy of lumber spine. Given any typical or atypical pars interarticularis caused by degenerative change, fluoroscopy-guided CBT screw fixation may not always allow simple and exact placement of the screw. However, these limitations can be resolved with the use of a technological method such as 3D-printed patient-specific guide or navigation. With technological advances, the customized trajectory for diverse anatomy of a single patient may become possible for maximum cortical bone contact and achieving the biomechanical advantage of the CBT screw. As such, the CBT technique is evolving to achieve secure excellent cortical bone contact and optimal trajectory. The CBT technique is not proven to be superior to PS fixation in all aspects in previous clinical, radiological, and biomechanical studies, and various methods have been suggested for safer and more reliable CBT fixation. Santoni et al. [17] first introduced CBT, and many studies have reported on its application and short-term outcomes. However, crucial in vivo data on prerequisites for inserting interbody for proper fixation have been published recently [31,68,69]. In addition, the CBT method might be technically challenging. Loss of reduction at the 1-year follow-up [70], direct loosening of all the screws on imaging, and loss of reduction despite intraoperative O-arm confirmation have been reported [68]. Moreover, the fusion rate as well as back and leg VAS score were similar in meta-analysis [49,65,67]. Although there are advantages of the CBT technique, a careful literature review is necessary. The present review has the following limitations. Most studies included in this review were retrospective case series of case–control studies. In vivo biomechanical results, definitive surgical indications and contraindications, and patient-related clinical/radiological outcomes and complications require further examination [44–47,57–59,61–63,71–75] (Table 3). For successful CBT fixation, the following guideline has been proposed. Imaging studies should be used for checking the screw trajectory, entry point, and spondylosis. If the pars interarticularis is not intact, PS fixation should be considered. Insertion of 5.5 mm diameter and 30–40 mm length screw on the way to 25°–30° cranially, 10° laterally toward posterior half of superior endplate [22]. Transverse rod connector can be an option to prevent micromotion that causes screw loosening or a lower fusion rate than that of the PS method [47,68].
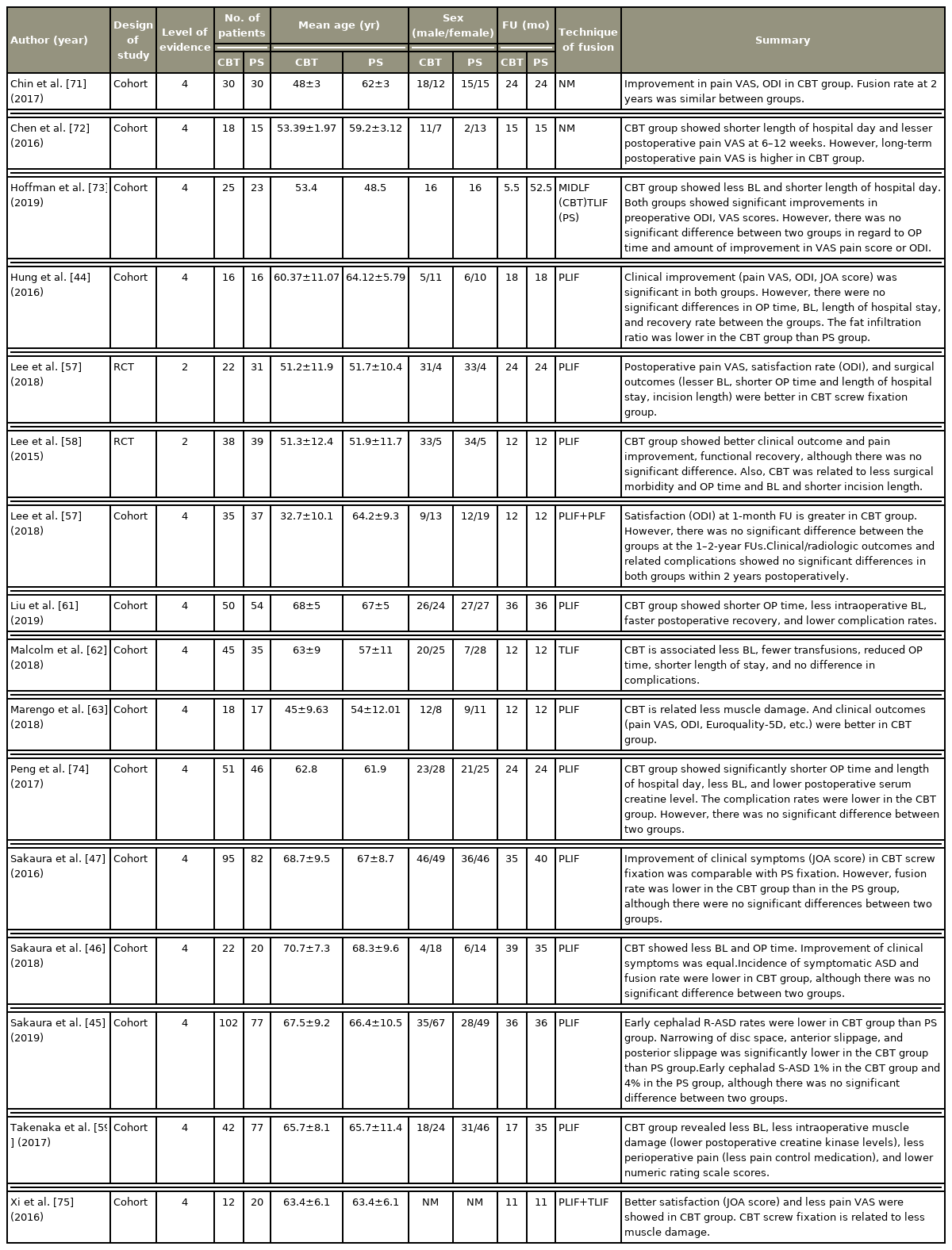
Characteristics of clinical and radiological studies
Conclusions
CBT screw fixation has been verified to be an effective and safe technique in lumbar surgery. Biomechanical studies showed similar or better results with the CBT technique than with fixation, depending on factors, such as screw position, size, and length. Clinical and radiologic outcomes showed equal or better results in the fusion rates, patient satisfaction, functional recovery, and complication incidence. Securing stability via maximal cortical bone contact is a major feature of the CBT technique; however, it is not applicable in all patients. The CBT technique is not always superior in biomechanical tests, and long-term follow-up results are yet to be reported. Thus, the CBT method is a safe and stable option for fusion, and surgery methods should be selected considering the patients’ condition.
Notes
No potential conflict of interest relevant to this article was reported.