Introduction
Treatment of non-small-cell lung cancer (NSCLC) with vertebral body invasion is challenging and is the current goal of several innovative surgical techniques. NSCLC with substantial invasion of vertebral bodies used to be a contraindication for surgery due to poor long-term survival [1]. However, en bloc resection of NSCLC after induction chemoradiotherapy has long-term survival with acceptable morbidity and a 5-year predicted survival rate of 43%–74% [23456].
O-arm (Medtronic Inc., Minneapolis, MN, USA) is an intraoperative full-rotation, multidimensional imaging system and a new computer-assisted surgery device. O-arm with a navigation system generates real-time multi-images and has an advantage for placement of pedicle screws [789]. Here, we report our successful use of O-arm in en bloc partial vertebrectomy for lung cancer. There have been no previous reports of such a procedure using O-arm. Use of this device permitted accurate confirmation of the surgical margins of osteotomy, and it was possible to perform osteotomy clearly and easily from a posterior approach.
The study was approved by the ethics committee of Nagoya University Graduate School of Medicine. The patient gave informed consent to the collection and use of data for research purposes.
Case Report
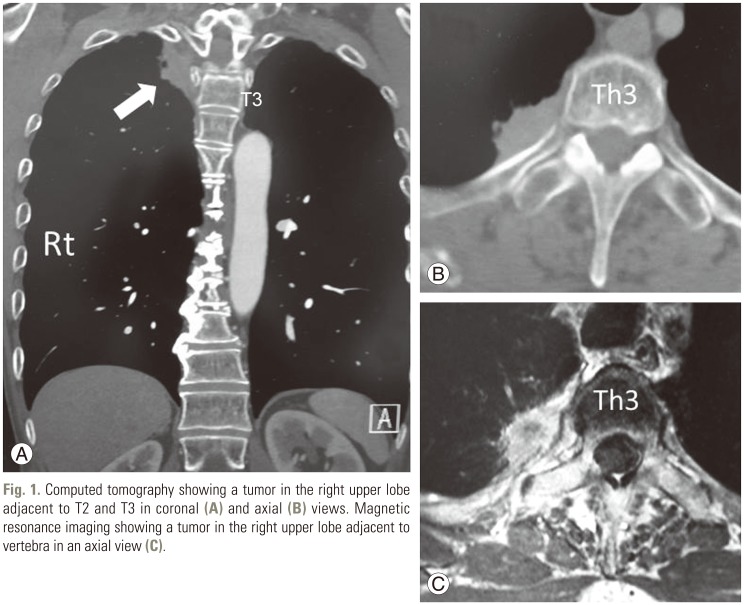
A 61-year-old man was found to have adenocarcinoma of the posterior apex of the right lung with invasion of the adjacent rib, thoracic wall, and T2 and T3 vertebral bodies, as shown on chest CT and magnetic resonance imaging (MRI) (Fig. 1). No distant metastasis was evident on abdominal CT, brain MRI, bone scan, and FDG-positron emission tomography, and thus the pretreatment TNM staging was IIIA (T4N0M0). Chemotherapy with two cycles of cisplatin and vinorelbine was conducted, together with radiotherapy at a dose of 40 Gy (2 Gy/day, 5 day/week). On subsequent chest CT, the tumor had shrunk by 25%. Restaging confirmed persistent T4N0M0 and en bloc resection was planned two months after performance of chemoradiotherapy.
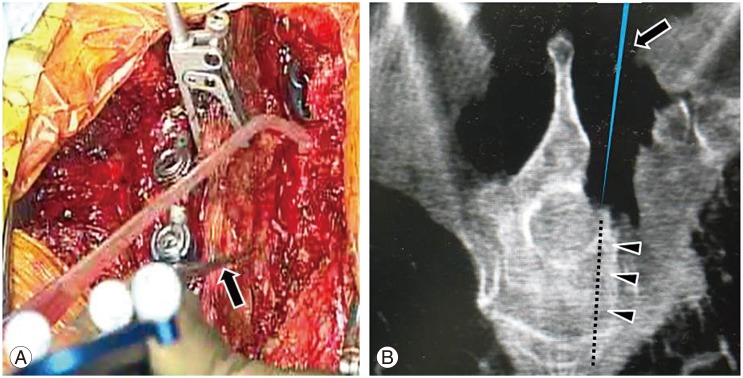
The surgical procedure was performed in two steps. First, the patient was placed in a prone position on a Jackson radiolucent table with a Mayfield head clamp, and a median posterior incision was made from C7 to T4. Pedicle screws were inserted at left T1 to T4, and right T1 and T4, and laminectomy from the right T2 to T3 was performed, followed by left rod fixation. On the right side, the pedicles and transverse processes from T2 to T3 were resected (Fig. 2A), the costovertebral joints were disarticulated, and the right T2 and T3 roots were dissected. After a reference frame was clamped to the exposed spinous process, an intraoperative CT scan was obtained sterilely with O-arm. With reference to the intraoperative CT data, the navigation system then generated real-time axial, coronal, and sagittal images that allowed confirmation of the location of the cutting edge in the T2–3 right vertebral internal bodies. Using the margin from the tumor defined in the preoperative plan, osteotomy was performed with a chisel to the anterior cortex (Figs. 2B, 3) and then right rod fixation was performed.
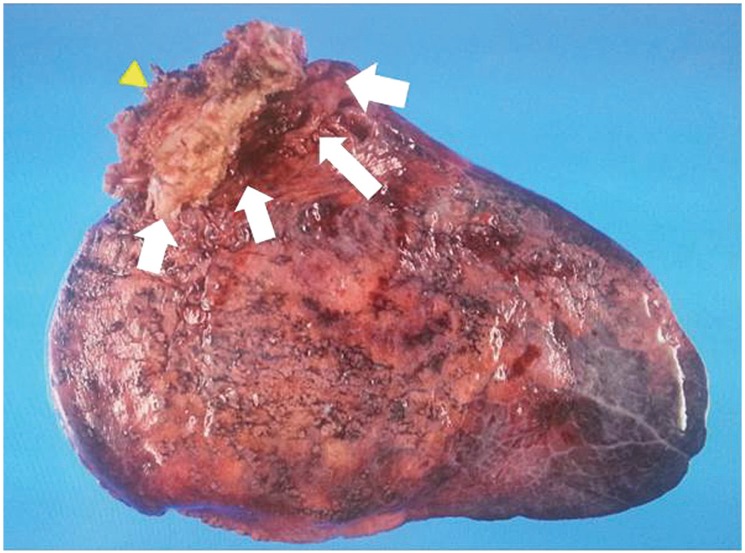
Second, the patient was placed in a left decubitus position, and a long posterior thoracotomy incision was made as a gentle arc from the spinous process of T2 to the inferior angle of the scapula. The right second and third ribs were resected in thoracotomy, with right upper lobectomy of the lung (Fig. 2C). A surgical specimen including vertebral bodies (T2 and T3), attached tumor, right upper lobe, and chest wall was extracted en bloc (Fig. 4). Finally, we confirmed hemostasis and closed the thoracotomy. The operation time was 493 minutes and the estimated blood loss was 1,242 mL.
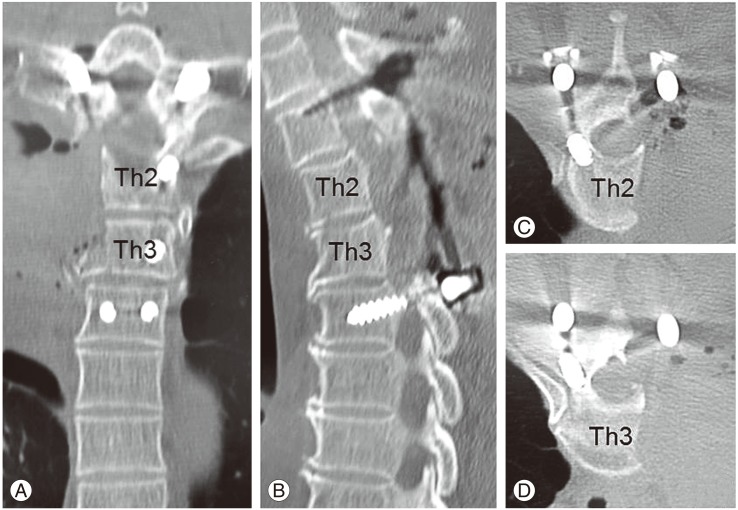
Pathologic examination confirmed complete resection of adenocarcinoma adjacent to the T2 and T3 ribs and vertebral body, which were not infiltrated. There have been no problems in the postoperative course and the patient has shown no findings indicating recurrence (Fig. 5).
Discussion
Introduction of spinal surgery techniques into lung cancer operations has improved the prognosis of lung cancer with vertebral invasion [21011]. En bloc resection of NSCLC can be achieved with acceptable morbidity and a 5-year predicted survival rate of 43%–74% [23456].
Yokomise et al. [6] described three procedures for vertebrectomy for lung cancer invading the spine: transverse resection (oblique osteotomy from posterior to the thoracic cavity), one-third resection (osteotomy from posterior to the canal, and subsequently from the thoracic cavity to the canal), and half resection (after laminectomy, osteotomy from the thoracic cavity to the canal). Each procedure is selected depending on the tumor size and extent of invasion, with reconstruction of the body recommended in more than half of vertebrectomies [1012].
Total en bloc spondylectomy (TES) is a useful procedure for metastasis to the spine [13]. TES is suitable in a case in which resection of more than half of the vertebral body is required, and bleeding is less than that in partial vertebrectomy. However, in the current case, less than half of the vertebral body was resected, vertebral body reconstruction was not required, and radiotherapy was performed. Therefore, en bloc partial vertebrectomy was considered desirable based on the reduced risk of non-union and rod breakage.
O-arm has utility for screw insertion in spine surgery [791415]. Santos et al. [14] showed that intraoperative O-arm images can accurately detect significant pedicle screw violations in the thoracic and lumbosacral spine. Shimizu et al. [15] reported that O-arm is useful for accurate pedicle screw placement in patients with scoliosis, and Ishikawa et al. [7] also evaluated the reliability of cervical pedicle screw placement using O-arm. O-arm has also been used in surgery other than spine surgery, such as in closed reduction of posterior sternoclavicular dislocations, arthroscopic glenohumeral arthrodesis, and video-assisted thoracoscopic surgery [161718]. However, there are no previous reports of use of O-arm in osteotomy for en bloc vertebrectomy with a posterior approach.
Grunenwald et al. [10] found that en bloc resection of lung cancer invading a vertebral body is complex and difficult to perform. Without use of O-arm, osteotomy of the anterior column might have to be performed via an anterior approach for en bloc partial vertebrectomy for a paravertebral tumor, after laminae and pedicle resection and screw fixation in a posterior approach. In such a procedure, it is difficult to confirm surgical margins for resection, and there would have been increased invasiveness due to the difficulty of en bloc partial vertebrectomy. In contrast, with intraoperative navigation using O-arm, as shown in the current case, it is easy to confirm the cutting edge with a navigation probe. A further advantage is that the intraoperative depth during osteotomy can be confirmed accurately and instantly using O-arm. Vertebrectomy can then be performed reliably with a chisel from a posterior approach. This procedure makes anterior osteotomy unnecessary and simplifies en bloc vertebrectomy. In addition, using O-arm, we were able to confirm the placement of pedicle screws intraoperatively.
In conclusion, we performed en bloc partial vertebrec-tomy for lung cancer adjacent to a thoracic vertebral body using the O-arm system. This case shows that O-arm can be used reliably and easily in vertebrectomy from a posterior approach to facilitate en bloc resection.