Bilateral Pedicle and Crossed Translaminar Screws in C2
Article information
Abstract
Multiple techniques exist for the fixation of C2, including axial pedicle screws and bilateral translaminar screws. We describe a novel method of incorporating both the translaminar and pedicle screws within C2 to improve fixation to the subaxial spine in patients requiring posterior cervical instrumentation for deformity correction or instability. We report three cases of patients with cervical spinal instability, who underwent cervical spine instrumentation for stabilization and/or deformity correction. Bilateral C2 pedicle screws were inserted, followed by bilateral crossed laminar screws. The instrumentation method successfully achieved fixation in all three patients. There were no immediate postoperative complications, and hardware positioning was satisfactory. Instrumenting C2 with translaminar and pedicle screws is technically feasible, and it may improve fixation to the subaxial spine in patients with poor bone quality or severe subaxial deformity, which require a stronger instrumentation construct.
Introduction
Several surgical techniques exist for the fixation of the cervical axis (C2). The transarticular screw fixation, introduced by Jeanneret and Magerl [1], offered a superior atlantoaxial rotational stability compared to the traditional wiring techniques pioneered by Gallie [2]. However, the risks accompanying this surgical option include injury to the vertebral artery, hypoglossal nerve, and spinal cord [3]. The newer C2 pedicle screw technique of Harms and Melcher [4] allows for rigid fixation of the axis and poses less risk of vertebral artery injury [5]. Both transarticular and transpedicular screws can be incorporated into subaxial and C1-C2 constructs [67]. The rigid fixation afforded by transpedicular screw instrumentation improves fusion rates, decreases postoperative malalignment, and reduces the need for postoperative immobilization with Halo vests or bracing [8]. Although no cases of vertebral artery injury were reported by Harms and Melcher [4], subsequent studies reported of screw breaches into the vertebral foramen, suggesting a risk of vertebral artery injury with this technique [910].
In 2004, Wright [11] reported on the bilateral crossing translaminar screw technique. When compared to transarticular and transpedicular fixation, the translaminar construct offers comparable biomechanical stability and fixation with improved rigidity in axial rotation but less resistance to lateral bending [121314]. This option boasts of high fusions rates (97.6% in the largest series) and essentially eliminates the risk of injury to the vertebral artery [15]. However, this technique has the potential risk of anterior laminar breach and cord injury [16], and the intraoperative radiographs have limited sensitivity for detecting the anterior breaches [17]. Although it is an uncommon requirement, the technique also precludes C2 laminectomy.
Screw pullout in cervical spine instrumentation is a relatively infrequent complication. According to biomechanical studies, C2 pedicle screws have superior insertional torque and pullout strength compared to other C2 fixation techniques [1819]. A retrospective study comparing axial pedicle screws to translaminar screws found a significantly higher rate of screw pullout rate, requiring reoperation in translaminar screws for the long subaxial constructs within 1 year postoperatively (6.1% vs. 0%) [20]. Screw pullout can be challenging to manage, and the low bone mineral density increases the risk of this complication [21]. Patients with comorbidities associated with low bone mineral density, such as osteoporosis and ankylosing spondylitis, are at an increased risk of screw pullout, and they may benefit from the improved fixation in axial-subaxial constructs. Significant kyphosis correction may also pose a higher level of stress on the proximal instrumentation and thus increase the incidence of screwbone interface failures. Screw pullout can be prevented with multiple points of fixation. Laminar hooks and sublaminar wires combined with pedicle screws can decrease the rate of screw-bone interface failure in osteoporotic bone [22]. However, instrumentation with laminar hooks and sublaminar wires poses risks of injury to the spinal cord.
Here, we report of a novel method for improving axis fixation and potentially preventing screw pullout in axial and subaxial cervical spine constructs, in which C2 is the upper most instrumented level. We incorporated both C2 pedicle and C2 bilateral crossed laminar screws in a series of three patients. To our knowledge, this is the first report of instrumenting four screws into C2.
Technical Note
We report three cases of patients with cervical spinal instability, who underwent cervical spine instrumentation for the stabilization and/or deformity correction. These three patients were prospectively followed for a minimum of 24 months. Postoperative computer tomography (CT) scans were obtained in all three patients to assess the accuracy of hardware position. Plain X-rays were done postoperatively, at 3 months, and at 1 year follow-up.
Once sedated under general anaesthesia, the patient was immobilized in a three-pin head clamp (Schaerer Mayfield USA Inc., Cincinnati, OH, USA) and carefully placed in a prone position on a Jackson table (Mizuho OSI, Union City, CA, USA). An X-ray confirmed the spinal alignment. The reference frame was attached to the Mayfield head clamp, where computer-assisted navigation was utilized. A midline incision from inion to C7 was followed by subperiosteal dissection to expose the posterior elements. C2 pedicle screws were inserted by identifying the bony landmarks of the pedicle and by using fluoroscopy or with navigated image-guidance. For the translaminar screws, small cortical windows were fashioned with a high-speed drill at the junction of the C2 spinous process and lamina. The contralateral lamina was drilled with a hand drill in the trajectory of the lamina, or slightly more dorsally to prevent ventral breach. A screw was inserted, and the process was repeated for the contralateral side. Care was taken to ensure that the starting points of the two screws allowed sufficient room for the passage of both screws. The subaxial spine was instrumented with lateral mass screws or pedicle screws. Lateral offset connectors were used to link the cross laminar screws to the rest of the construct. Crosslink connectors were applied to prevent rotational failure. Given the potentially reduced surface area, available for bone graft secondary to bulkier instrumentation, meticulous decortication of the C2-C3 joint was undertaken prior to the insertion of hardware. Moreover, the lamina of C2, the subaxial cervical spine lamina, and lateral masses were also carefully decorticated, and the bone graft was placed to promote the fusion. Autologous bone graft from the decompression or from the posterior iliac crest is the preferred graft option.
1. Case 1
A 73-year-old male sustained an isolated ligamentous injury following a low-velocity injury. After a trial of external immobilization, he developed a progressive cervical kyphotic deformity to the point where he had a chin on the chest deformity with mandibular pressure sores. After a successful initial course of traction, posterior surgical stabilization was undertaken (Fig. 1A). At 24 months of follow-up, the patient's neck pain had resolved. X-rays demonstrated satisfactory hardware positioning and preservation of the deformity correction (Fig. 1B).
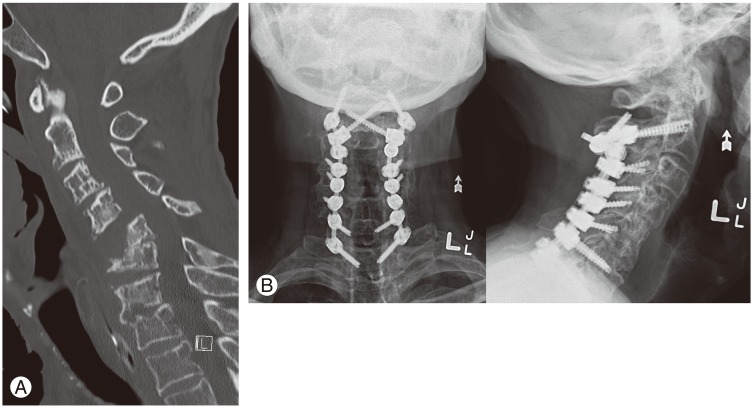
A 73-year-old male presented with a progressive cervical spine kyphotic deformity which developed a left arm weakness and neuropathic pain. (A) Preoperative sagittal cervical spine computer tomography demonstrating C5/6 kyphotic deformity and C3-5 anterolisthesis. (B) Postoperative lateral and anteroposterior cervical spine X-rays A of a C2-T1 instrumented fusion.
2. Case 2
A 65-year-old male with psoriatic arthritis was referred with a 2 month history of progressive arm and leg weakness, paresthesias, and hand clumsiness. His examination was consistent with cervical myelopathy. A cervical spine CT revealed C2-C4 anterolisthesis with severe canal stenosis and a kyphotic deformity at C4 and C5 (Fig. 2A). The patient underwent a posterior-anterior-posterior cervical decompression and fusion.

A 65-year-old male presented with cervical myelopathy. (A) Preoperative sagittal cervical spine computer tomography (CT) demonstrating C2-C4 anterolisthesis with kyphotic step deformity at C3 and C4. (B) Postoperative lateral and anteroposterior cervical spine X-rays of a C2-T1 instrumented fusion. (C) Postoperative axial cervical spine CT illustrating the arrangement of the C2 pedicle and crossed laminar screws.
Postoperative imaging revealed satisfactory hardware positioning (Fig. 2B). Fig. 2C shows an axial CT revealing the configuration of the pedicle and translaminar screws in C2. At 24 months of follow-up, the patient's myelopathic symptoms improved considerably.
3. Case 3
A 49-year-old male with ankylosing spondylitis had previously undergone a T4-S1 fusion for a thoracic kyphotic deformity. Years later, he sustained a fracture on the C5-C6 ankylosed level, which extended through the anterior and posterior columns of the spine (Fig. 3A). He was neurologically intact, but the fracture was highly unstable so an operative intervention was pursued.
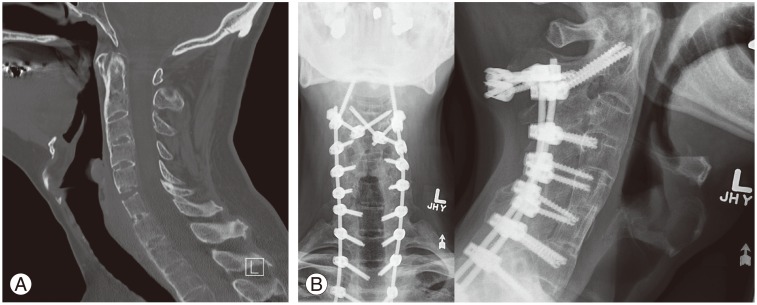
A 49-year-old male with ankylosing spondylitis was referred after falling backwards on ice. (A) Preoperative sagittal cervical spine computer tomography revealing a C5-6 bony fusion mass fracture. (B) Postoperative lateral and anteroposterior cervical spine X-rays of a C2-T3 instrumented fusion.
Postoperatively, the patient remained neurologically intact. Cervical spine X-rays revealed a satisfactory hardware positioning (Fig. 3B). At 24 months follow-up the patient remained neurologically intact with satisfactory alignment.
All three patients required axial and subaxial fixation for deformity correction or due to instability. There were no immediate postoperative hardware-related complications, such as vascular or neurologic injury, instrumentation failure, or infection. The most recent follow-up imaging confirmed satisfactory hardware positioning and preservation of alignment, without any cases of screw pullout. The third patient had ankyloses at C2-C3 preoperatively, and the follow-up X-ray confirmed that the fusion was retained at this level. Although it was difficult to identify radiographic fusion at C2-C3 for the first two patients, from the postoperative plain X-rays, neither patients demonstrated any clinical evidence of pseudoarthrosis or non-union during the follow-up.
Discussion
The most popular techniques for C2 fixation are the Harms C2 pedicle screws and Wright's translaminar screws. Pedicle screws can achieve superior screw pull-out strengths compared to translaminar screws. However, pedicles screws have an increased risk of vertebral artery injury. Although bone-implant interface failure is uncommon at the level of the axis, some patients with poor bone quality, due to underlying medical conditions or with anatomy that demands more rigid fixation, may benefit from a construct that incorporates both the pedicle and translaminar screws in C2. This is particularly in the longer constructs, where the highest level instrumented is C2. Here, we report of two patients with ankylosing spondylitis and psoriatic arthritis, and one patient with a severe cervical kyphosis and C3-C5 anterolisthesis. Combining both the pedicle and translaminar screws in C2 allowed for the improved fixation of the axis to the subaxial spine. The additional fixation points at C2 also improved rotational stability, negating the need for additional crosslinks. We believe that this technique offers the spine surgeons an alternative option for such anticipated high-risk patients. However, since the reported failure rates for conventional techniques are low, we would not recommend using this dual technique for routine cases.
The cases described here would have traditionally been instrumented with C2 pedicles or laminar screws in most of the centers, including ours. Although it is unclear if the additional instrumentation incorporated in this technique was necessary for a successful outcome, we have demonstrated that this construct is a feasible and safe option for use in patients with poor bone quality or severe deformity. The technique adds to the potential surgical options that can be used to achieve a solid axis fixation in the cases where screw-bone interface failure is a particular concern. The added C2 fixation points may also allow for the preservation of more proximal motion segments. Whilst we assume that this construct is biomechanically superior to other techniques, formal biomechanical studies are lacking and would be worthwhile pursuing. An alternative to this technique, in the long constructs with higher pullout risk at C2, is supplementing the posterior fixation with a C2-C3 anterior cervical discectomy and fusion [23]. Circumferential fusion increases the strength of the construct and may be an excellent option in selected cases with the caveat that it adds another approach to the procedure, and is associated with specific adverse events, including dysphagia.
The main limitations of this four-screw technique are the added potential operative complications and increased surgical time. We did not encounter any operative complications, but our assessment of the complication rate is limited by the small number of patients treated with this technique. This technique is certainly associated with the potential risks of both cervical pedicle screws and translaminar screws, including vertebral artery injury and ventral breach, respectively. Difficulty with the rod contouring, to incorporate both the four screws in C2 as well as the subaxial instrumentation, is also noteworthy. Rod contouring can be facilitated by side link connectors to the C2 pedicle screws or by using cervical pedicle screws instead of lateral mass screws subaxillary. The additional hardware at the C2 level reduces the exposed bone surface area, potentially limiting the surface available for fusion. This reinforces the importance of meticulous decortication and posterolateral grafting techniques. More hardware at the C2 level creates more artifacts on postoperative multi-planar imaging, and thus, it has the potential to impact on the radiographic fusion assessment. However, we did not find it interfering with the assessment of the C2-C3 facet line on the postoperative high quality CT scan, which confirms that arthrodesis status can still be established despite of this imaging pitfall. With meticulous surgical techniques, we achieved solid C2 fixation in three patients, without any hardware-related complications.
In conclusions, transpedicular and translaminar screws are two established approaches for C2 fixation with different advantages and disadvantages. Here, we demonstrated that the incorporation of both fixation methods in the axis is possible. This approach may provide improved fixation in patients with severe anterolisthesis, kyphotic deformity, or poor bone quality.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.