Adolescent Scoliosis Screening in Nara City Schools: A 23-Year Retrospective Cross-Sectional Study
Article information
Abstract
Study Design
Retrospective cross-sectional study.
Purpose
To determine the prevalence of idiopathic scoliosis, define the distribution of the curve magnitude, evaluate the accuracy of Moiré topography as a screening tool, and investigate the cost-effectiveness of our screening system.
Overview of Literature
Early detection of idiopathic scoliosis provides the opportunity for conservative treatment before the deformity is noticeable. We believe that scoliosis screening in schools is useful for detection; however, screening programs are controversial owing to over referral of students who do not require further testing or follow-up. In Japan, school scoliosis screening programs are mandated by law with individual policies determined by local educational committees. We selected Moiré topography as the scoliosis screening tool for schools in Nara City.
Methods
We selected Moiré topography as the scoliosis screening tool for schools in Nara City. We screened boys and girls aged 11-14 years and reviewed the school scoliosis screening results from 1990 to 2012.
Results
A total of 195,149 children aged 11-14 years were screened. The prevalence of scoliosis (defined as ≥10° curvature) was 0.057%, 0.010%, and 0.059% in fifth, sixth, and seventh grade boys and 0.337%, 0.369%, and 0.727% in fifth, sixth, and seventh grade girls, respectively. The false-positive rate of our Moiré topography was 66.7%. The minimum cost incurred for scoliosis detection in one student was 2,000 USD.
Conclusions
The overall prevalence of scoliosis was low in the students of Nara City schools. Over 23 years, the prevalence of scoliosis in girls increased compared to that in the first decade of the study.
Introduction
Adolescent idiopathic scoliosis is defined as a lateral curvature of the spine ≥10°. Although the rate of change is unpredictable, rapid progression of the curvature can occur. Severe curve deformity is a cosmetic concern, and more importantly, it is associated with an increased risk of mortality and morbidity [1]. It is important to detect scoliosis in its early stages and begin conservative treatment with bracing early in the disease course to prevent progression to severe scoliosis, which requires invasive treatment [2].
While there is agreement that the early detection of scoliosis is important, the need for a screening program in all schools has been debated [34]. Currently, insufficient evidence for both recommending and rejecting routine screening exists [5].
The main concerns about routine screening are unnecessary referrals and excessive costs owing to a high false-positive rate [36]. However, we believe that it is a powerful tool to detect scoliosis at an early stage in children.
Several screening methods exist. The most widely used is the forward bending test, which has high false-positive and false-negative rates [47]. Moiré topography is a biostereometric screening technique that projects contour lines, or Moiré fringes, on a subject's back [89]. This method is more sensitive than conventional clinical screening including the forward bending test [10].
Routine school scoliosis screening was initiated as part of the national school health screening program in Nara City in 1978. Moiré topography was adopted as the preferred screening test in 1989. Currently, we routinely screen the fifth and seventh grade students.
The objectives of our study were to (1) determine the prevalence of adolescent idiopathic scoliosis over 23 years (1990-2012) and compare the prevalence between the first and last decades of that time period; (2) evaluate the curve magnitude and distribution; (3) evaluate the accuracy of Moiré topography as a screening tool by determining its false-positive rate; and (4) investigate the cost to detect scoliosis with our screening system.
Materials and Methods
The authors obtained approval for this study design and the publication of this manuscript from the Nara City Medical Association.
1. Subjects
This retrospective cross-sectional study included 195,149 public school children who were screened for scoliosis in Nara City from 1990 to 2012. Students of two school grades (fifth and seventh grades) were routinely screened. Moreover, we screened sixth grade students between 1993 and 2002. The ages of the fifth, sixth, and seventh grade students were 11-12 years, 12-13 years, and 13-14 years, respectively.
2. School scoliosis screening program in Nara City
The initial screening was performed using Moiré topography by 1 nurse and 1 radiology technician in all the schools. We included children previously diagnosed with or currently being managed for scoliosis. Each child was told to stand erect in a relaxed position for approximately 1 minute. A Moiré photograph was taken; the number of fringes on each half of the back were compared and determined to be symmetric or asymmetric. One spine specialist reviewed all of the photographs to identify abnormal Moiré patterns (asymmetry indicating a rotational component) or abnormal clinical signs such as an uneven shoulder height, pelvic tilt, or waistline differences (abnormalities indicating lateral deviation). Students with abnormal findings were referred for radiography. Because it was not compulsory, radiography was not performed for all students. Those found to have a Cobb angle ≥20° were referred to a spine specialist for additional intervention such as a brace treatment.
3. Data collection
In our cohort, the demographic information, school grade, date, and results of tests were obtained at each visit, and the Cobb angle measurements were obtained from the Nara City Medical Association.
4. Statistical analysis
Prevalence rates were calculated at predefined Cobb angles of 10°-19° and ≥20°. A Cobb angle of ≥10°, as defined by the Scoliosis Research Society, was considered positive for scoliosis; an angle ≥20° was the threshold for evaluation for brace treatment.
1) Prevalence of scoliosis
Using a chi-square test, we compared the prevalence of scoliosis between the first decade (1990-1999) and the last decade (2003-2012) to determine changes in prevalence over time.
2) Accuracy of Moiré topography
We calculated the false-positive rate to evaluate the accuracy of the Moiré topography test using the following formula:

Using a chi-square test, we compared the false-positive rate from the first decade (1990-1999) with that from the last decade (2003-2012) to determine changes in the false-positive rate over time.
Some students declined radiography although their Moiré topography was positive. We excluded these student data.
3) Cost of scoliosis screening
We investigated the cost of the initial and second screening including diagnostic costs and staff salaries. Finally, we calculated the cost to identify one scoliosis student with a lateral curvature of ≥10°.
Results
1. Prevalence of scoliosis
The overall prevalence rates are shown in Table 1. The prevalence rates from 1990 to 1999 are shown in Table 2, and those from 2003 to 2012 are shown in Table 3. Of the students with positive Moiré topography, 259 declined to undergo radiography and were excluded from the study.
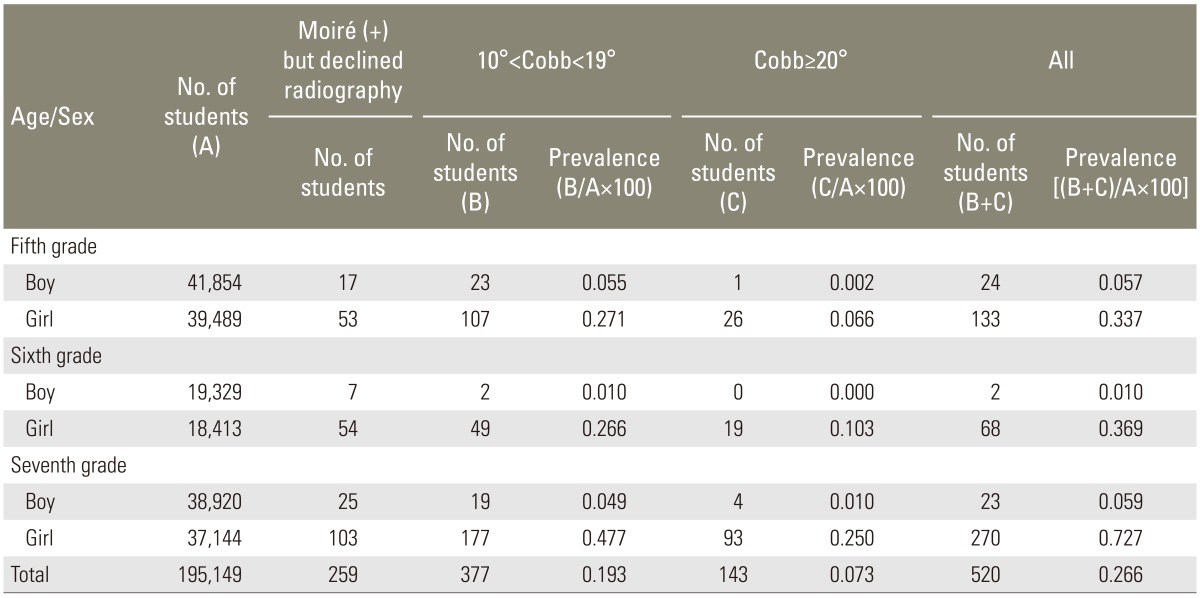
The prevalence of scoliosis in each grade group from 1990 to 2012

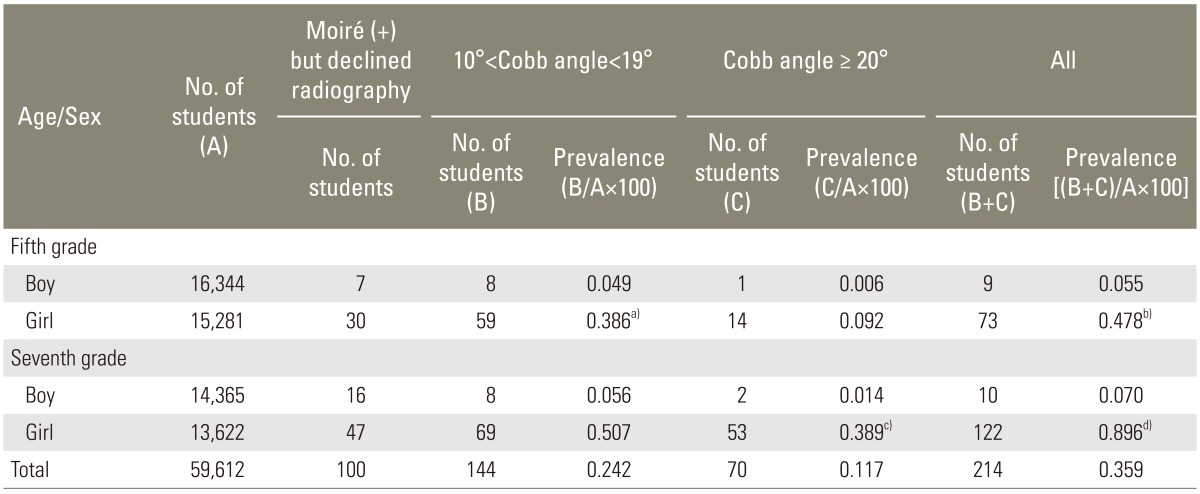
The prevalence of scoliosis in each grade group from 1990 to 1999
The prevalence of scoliosis in each grade group from 2003 to 2012
1) Overall prevalence of scoliosis
The prevalence rate of scoliosis in the fifth grade girls was similar to that in the sixth grade girls (0.337 and 0.369, respectively). The prevalence rate of scoliosis in the seventh grade girls was 0.727, which was significantly higher than that in both the fifth (p<0.01) and sixth (p<0.01) grade girls. The prevalence rate of scoliosis in boys was low, and the prevalence rate in the sixth grade boys was 0.01, which was significantly lower than that in both the fifth (p=0.01) and seventh (p=0.01) grade boys (Table 1).
2) Cobb angle ≥20°
The prevalence rates in girls gradually increased from the fifth to the seventh grade. Meanwhile, for boys, the prevalence rates did not change among the three groups (Table 1).
3) Comparison of prevalence in the first and last decade of the study
The prevalence of scoliosis from 1990 to 1999 is shown in Table 2 and from 2003 to 2012 in Table 3. The prevalence rate was significantly different between the first and last decade for girls in the fifth grade with a Cobb angle >10° but <19° (0.225% vs. 0.386%, p<0.01) and for girls in the seventh grade with a Cobb angle >20° (0.157% vs. 0.389%). A statistically significant increase was also found in the overall prevalence during the 10 years.
4) Curve magnitude distribution
The distribution of curve magnitudes for boys and girls is shown in Fig. 1.
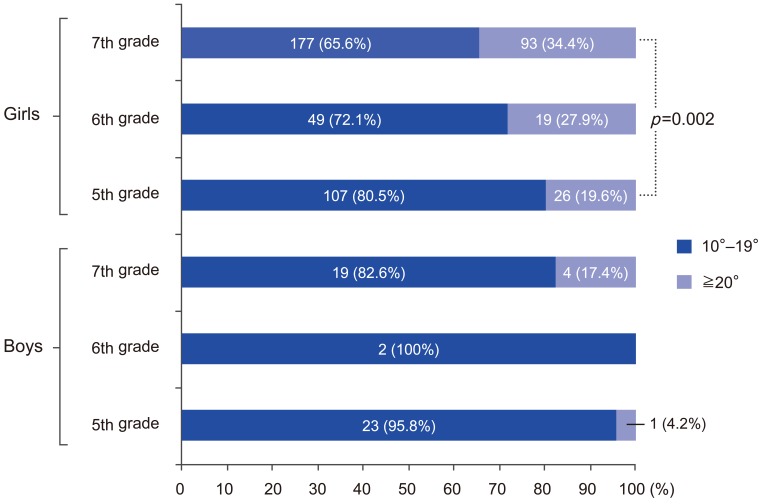
Distribution of curve magnitudes for boys and girls. Scoliosis is defined as a Cobb angle ≥10°. The need for additional intervention such as brace treatment was indicated in cases with a Cobb angle ≥20°. A statistically significant difference in the prevalence of scoliosis between girls of fifth and seventh grade occurred.
The prevalence of a Cobb angle ≥20° gradually increased with age in both boys and girls. The prevalence was similar among boys in the fifth, sixth, and seventh grades. The difference in the percentage of children with a Cobb angle ≥20° was statistically significant only between girls in the fifth and seventh grades (19.6% vs. 34.4%, p=0.002).
2. Accuracy of Moiré topography
From 1990 to 2012, 1,820 children had a positive Moiré topography test (Table 4). Of those, 259 children (49 boys, 210 girls) declined to undergo radiography and were excluded from the study. Consequently, radiographs from 1,561 students with a positive Moiré topography test were analyzed. When the radiographs were interpreted, a Cobb angle ≥10° was seen in only 520 students (predictive value: 33.3%), thus leaving 1,041 children with a positive screening test but a negative result on radiographs. Of these children, 795 were girls, and 246 were boys; thus, the Moiré test had a false-positive rate of 66.7% (Table 4).
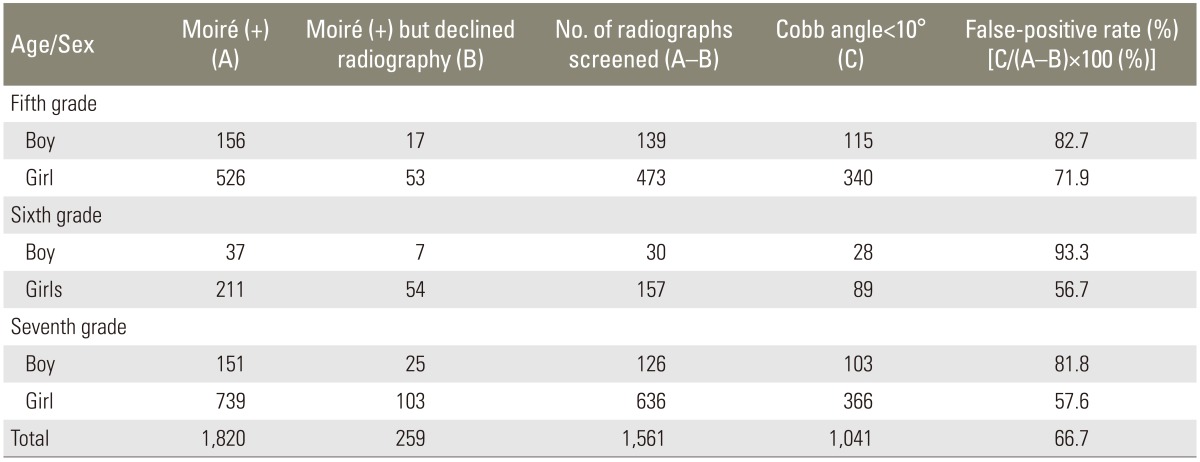
Overall false-positive ratios in patients who showed positive results on Moiré topography from 1990 to 2012
We compared the false-positive rate between 1990-1999 and 2003-2012 and between genders. A statistically significant decrease in the false-positive rate was found between the first and last decades of the study in the seventh grade girls (61.8 vs. 53.1, p=0.007). No other significant change was found (Tables 5, 6).
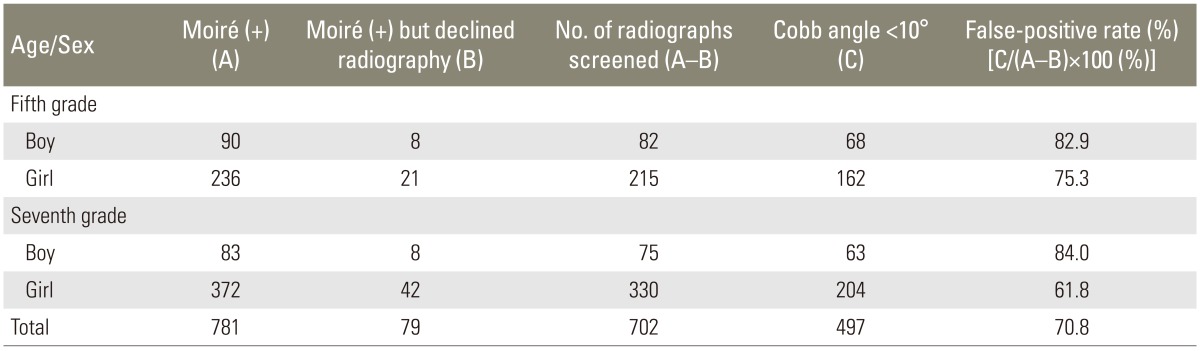
The false-positive ratios in Moiré topography from 1990 to 1999
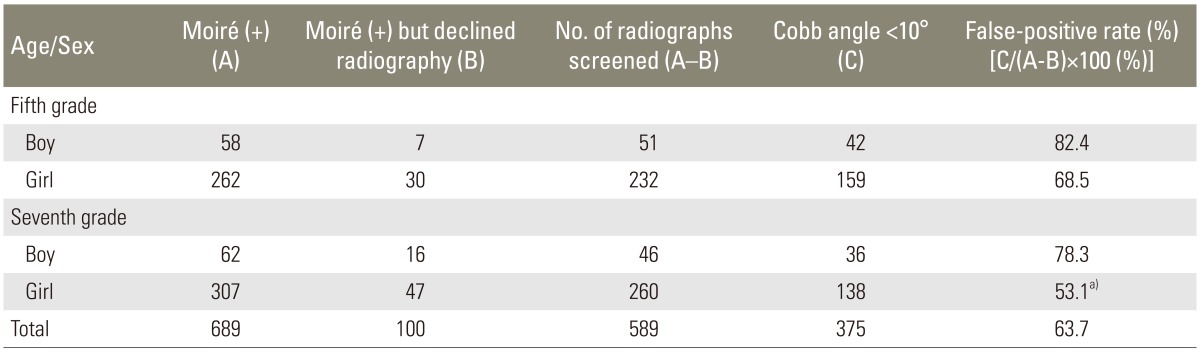
The false-positive ratios in Moiré topography from 2003 to 2012
3. Cost of scoliosis screening
We screened 195,149 students with Moiré topography. The cost of Moiré topography for each child was 5 USD. Furthermore, we used radiography as the second screening tool for diagnosing scoliosis in 1,561 students. Its cost was 40 USD for each child. In all, 520 students with Cobb angle ≥10° were identified. Of those, 143 students had a Cobb angle ≥20°. Overall, an amount of 1,996.5 USD was required to identify one scoliosis student and an amount of 7,260 USD was required to identify one student with a Cobb angle ≥20°.
Discussion
1. Prevalence of scoliosis
A review of multiple studies in the literature revealed that the prevalence of idiopathic scoliosis was 0.04%-0.66% in boys and 0.4% to 2.22% in girls [7111213]. Boys generally have a lower prevalence than girls. Although lack of standardization and consistency in the cohort age group, diagnostic criteria, and screening methods makes comparing studies difficult, we found the prevalence in Nara City to be consistent with that reported in the literature [7111213] for boys but slightly lower in girls (Table 1).
However, the prevalence in the current decade of our study was higher than that in the first decade, especially for girls in the fifth and seventh grades. We were unable to identify the exact reason for this difference. Progression of the curve magnitude in scoliosis is related to growth velocity [1415]. In girls, menarche is strongly associated with growth velocity [16]. Orito et al. [17] reported that the mean age of menarche in Japanese girls was 12.0±1.2 years. We do not have data regarding growth velocity and height change for the participants in our study; however, the girls in our study were at the mean age for menarche and, therefore, had an increased growth velocity. Although the increased prevalence of scoliosis in girls over the last 23 years seen in our study may be related to a higher growth velocity in girls in the last decade compared with that in the first decade, we do not have data to support this hypothesis; this difference requires further research.
2. Accuracy of Moiré topography
Moiré topography was the only test that was used in this study for school screening. Based on our results, the screening test's false-positive rate ranged from 56.7% to 93.3%, which was high in both sexes but was higher in boys. This high false-positive rate leads to over referral and unnecessary additional medical costs. No significant improvement in the false-positive rate was found between the first and current decades except in seventh grade girls. Because a single spine specialist performed all of the screening tests, the fact that the false-positive rate did not change indicates that it did not improve with experience. Moreover, the examiner was undoubtedly concerned about the test missing children with scoliosis. This concern could account for high false-positive rates.
An assessment of the correlation between the prevalence of scoliosis and false-positive rate revealed a significant negative relationship. In other words, the false-positive rate increased even as the prevalence of scoliosis decreased (Fig. 2) (by Pearson's correlation coefficient analysis, r=-0.52, p<0.001). To reduce costs and over referrals, more research is necessary to determine and incorporate ways of reducing the high false-positive rate observed in our screening program. Fong et al. [18] suggested that a combined examination (e.g., the angle of trunk rotation combined with Moiré topography or low-dose radiography) improved the accuracy of screening results. Because the angle of trunk rotation can be used to screen many students quickly and inexpensively, we think that this technique should be used with Moiré topography in any future screenings.

Prevalence of scoliosis and false-positive rates. A statistically negative correlation was found between the prevalence of scoliosis and the false-positive rate of Moiré topography in boys and girls (r=-0.52, p<0.001).
3. Cost of our scoliosis screening
The cost of our scoliosis screening was much lower than that of the invasive treatment required for advanced scoliosis. All screening costs were covered by our municipal government. As shown in our results, an amount of 1,996.5 USD was required for our school screening system to identify one scoliosis student, and an amount of 7,260 USD was required to identify one student with Cobb angle ≥20°. The cost for surgical intervention involving fusion of more than 5 vertebrae in Japan is at least 13,900 USD, which is strictly the surgery cost and does not include costs incurred during the hospital stay. With regard to the cost for identifying one student with Cobb angle ≥20°, our scoliosis screening system did not exceed the surgical costs. Yawn and Yawn [19] reported the cost for identifying one student with a curve of 20° or more by age 19 in Minnesota, USA, was 3,386 USD. In comparison with the cost reported by them, our scoliosis screening system required over twice the amount, which may be attributable to the high false-positive rate of the Moiré topography test.
In this study, we only focused on the cost incurred to identify one scoliosis student. We did not attempt to assess the benefits of scoliosis screening to allow for a cost-benefit analysis. Such an analysis would require the determination of short- and long-term benefits of early diagnosis and treatment of adolescent idiopathic scoliosis such as a potential reduction in the number and complexity of spinal surgeries for scoliosis. One of the several limitations of our study was that our scoliosis screening system could not follow scoliosis students until skeletal maturity was achieved. Therefore, we did not have inclusive data from initial screening through skeletal maturity. The aim of school screening is early diagnosis so that conservative treatment with bracing can be used and invasive intervention can be avoided, and the effectiveness of a screening program is determined by the number of children successfully treated without surgical intervention. Therefore, we did not have sufficient data to evaluate the effectiveness of our school screening program. Second, we did not have definite criteria for diagnosing scoliosis using Moiré topography. It is a subjective test, and this reason might contribute to the high false-positive rate. Third, although we found a significant difference in the prevalence of scoliosis between the first and current decades, our data did not allow us to determine the reason for this difference.
Conclusions
The overall prevalence of scoliosis in Nara City was lower than that reported in previous studies. In girls, the prevalence of scoliosis increased since the first decade of our study. The prevalence in boys was lower than in girls and did not change significantly over the 23 years. Our school screening test, Moiré topography, had a high false-positive rate, which did not improve with examiner experience. Although our screening cost was less than that for surgical intervention in Japan, it was twice as high as that in Minnesota, USA. Our study has highlighted the need for further research in the area of reduction of the false-positive rate of Moiré topography for scoliosis screening. Additionally, any future studies should focus on modifying the Moiré topography for use as an accurate screening tool through skeletal maturity and extend the assessment to include benefits, cost savings, risks, and indirect costs to the children and to society in order to determine a cost-benefit estimate.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.