Introduction
The pathologies related to the spine, encountered in tertiary hospitals, are increasing and emergence of modern diagnostic methods may be one of the reasons for this increase. The morbidity of the patients and the impact of the spinal diseases on the socioeconomic profile of the family are important aspects in treatment of affected patients, and as affected individuals with spinal problems requiring operative intervention are usually referred to a tertiary center, we are presenting the demographic profile of the patients consulting with the chief spine surgeon for operative treatment via the transthoracic transpleural approach.
Materials and Methods
Patients attending emergency services and outpatient department with spinal pathologies requiring surgery were enrolled for this study. The indications for the surgery were for patients with a neurological deficit with compressive myelopathy requiring decompression. Any stable fractures with no neurological deficits were excluded and also excluded were unstable fractures with no neurological deficit as they were planned for posterior stabilization and no decompression was required for them. This study was confined to the surgery of the dorsal and thoracolumbar junction (TLJ) until L2 vertebrae. Since all the enrolled patients were having compressive myelopathy anterior to the spinal cord, they were operated using transthoracic transpleural (anterior) approach and anterior decompression. The decompression was done till the spinal cord was free of compression from all the sides.
After admission, a patient's particulars and demographics were recorded and stored. After a thorough preoperative planning, these patients underwent surgery.
Results
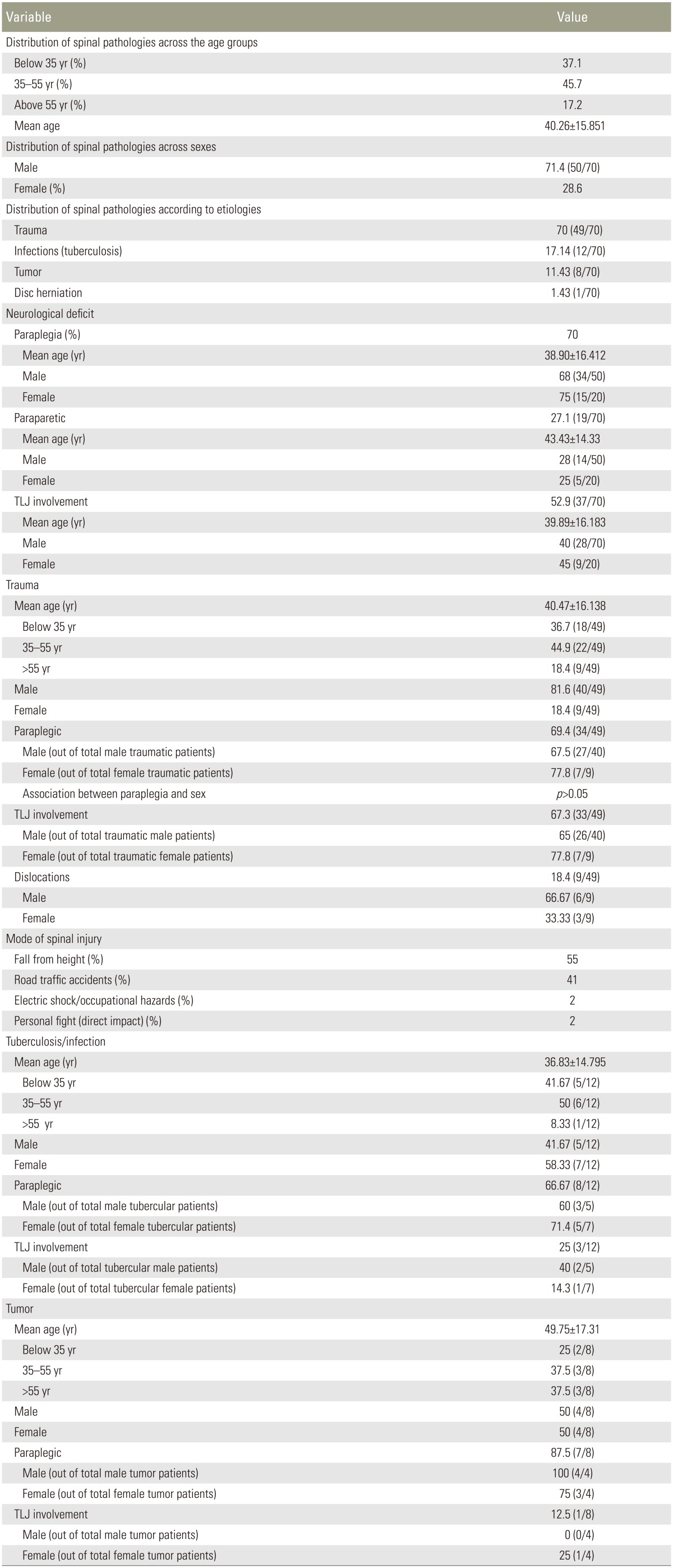
The spinal pathologies operated by anterior transthoracic transpleural approach were sorted according to various etiologies such as trauma, infection, tumors, and disc herniation. The various demographic profiles for each etiology were than studied. Using Pearson chi-squared test, the association for presence of paraplegia against various etiologies in addition to age and sex of the patients was made. With the chi-squared test, the association of the involvement of TLJ (D11ŌĆōL2) was also tested against the etiologies, age and sex of the patients (Table 1).
A total of 70 patients with a mean age of 40.26┬▒15.851 years (range, 5ŌĆō73 years) were collected in this study. The most commonly affected age group was 35ŌĆō55 years (45.7% of the total). Patients below 55 years of the age were 82.8% of the total enrollees. Males comprised 71.4% (50 out of 70 patients) and females were 28.6% of the patient pool.
Forty-nine patients (70%) were paraplegic with a mean age of 38.90┬▒16.412 years and 19 patients (27.1%) were paraparetic with a mean age of 43.43┬▒14.33 years. There was no significant association between age and occurrence of paraplegia in patients (p>0.05). The paraplegic population comprised 75% of the females and 68% of the males; however, there was no relationship between sex and the occurrence of paraplegia (p>0.05).
TLJ (D11ŌĆōL2) was involved in 52.9% (37 out of 70) of patients across all the pathologies. There was no significant association between involvement of TLJ and sex or age (p>0.05 for both cases). In the trauma cases, 67.3% were confined to TLJ, which was significant (p<0.05). Ten percent of the fractures were associated with fractures of two or more non-consecutive vertebrae. Males made up 81.6% of the trauma patients. Among the male trauma patients, 12.5% were above 55 years of age; on the contrary, among the female trauma patients, 33.33% were above 55 years of age.
Unstable burst fractures were 83.7% of the fractures, while the rest was rotational types. For the trauma patients, 69.4% (34 out of 49 patients) were paraplegic while 26.5% (13 out of 49 patients) were paraparetic. For the paraplegic patients, 40% (13 patients) had upper dorsal fractures (up to D8 vertebra) while among paraparetic patients, 30.8% (four patients) had upper dorsal fractures.
Tuberculosis is documented to most commonly affect the lower thoracic and TLJ (66.67%) in both males and females. Mid dorsal spine (D6ŌĆō7) is also equally involved as that of lower thoracic in case of females. Males 35ŌĆō55 years old were the more common age group (60%) in compare with the younger or older age groups while in the females, those below 55 years of the age were the more common group. For the patients, 66.67% had paraplegia while 33.33% had paraparesis.
Among the patients with tumor pathologies, the different etiologies were hemangioma, plasmacytoma, giant cell tumor and metastasis from carcinomas of prostate, thyroid, breast and kidney. Metastasis from breast carcinoma was more common than other etiologies. Almost equal number of males and females were affected. For these patients, 87.5% were paraplegic. There was a male patient 38 years old having D6ŌĆō7 disc herniation with paraplegia.
Discussion
To date, demographic representation of spinal pathologies, which required operative decompression, has not been studied in great detail. This was an attempt to know the demographic picture of patients with compressive myelopathy due to various spinal pathologies being treated at a tertiary center in a developing country.
Trauma is still the most common ailment affecting the spine. Very little literature is available on the epidemiology of traumatic spine injuries in developing countries [1]. As there is a growing incidence of trauma, multiple level spinal fractures and associated injuries are increasing being treated. Generally fractures around TLJ constitute one of more common fractures in multiple level spinal injuries as in our study.
The very rigid thoracic spine is sandwiched by two very flexible junctions. When a deceleration/acceleration force acts on the spine, the rigid thoracic spine is well protected by the support of the rib cage, while the junctions absorb most of the force, which explains the higher frequency of fractures at these junctions. Thoracolumbar fractures are more frequent in men, and the peak incidence is observed between 20 and 40 years of age [2]. While the same age group was also prominent in our study, for our series, thoracolumbar fractures were more common in females than males. This may be explained by an increasing prevalence of trauma in females, as they are also actively involved outside the house for daily activities as well as working in rural settings. The increased prevalence of TLJ fractures in females can be explained by the assumption that the TLJ is more flexible in females, but this needs to be studied further to explain the difference of flexibility at the TLJ for the different genders.
When the mid-section of the thoracic spine is injured in a young patient, it is almost guaranteed that the cause must have been a high-energy trauma [3]. There is also associated blunt trauma to chest or abdomen with mid dorsal spine injuries. In our series, out of 18 patients with upper and mid thoracic fractures only four patients were of older age. All these patients were victims of vehicular accidents.
Increased prevalence of fractures in females over 55 years may be affected by occurrence of osteoporosis. The increased incidence of traumatic fractures in females in the older age group is related to the higher incidence of osteoporosis in this gender and age group in developing nations.
The male to female ratio in the present study was 4.43:1, and it was lower than that of Chacko et al. [4] in 1986 (male to female ratio of 13.5:1) but higher than Singh et al. [5] in 2001 (male to female ratio of 2.96:1) and others [6].
From different studies, neurological injury complicates 20%ŌĆō36% of fractures at the TLJ [7]. The chances and extent of neurological deficit depend on the type of fracture. In this study, though it was not statistically significant, the proportion of females who were paraplegic was higher than that of males and this can be explained by a supposedly smaller spinal canal in the females than that of males though there have been no study comparing thoracic and lumbar spinal canals across the sexes in an Indian/Asian population. In our series since only those patients have been studied who were operated upon, the prevalence of neurological deficit could not be studied but a higher prevalence of paraplegic patients than paraparetic ones indicate a higher probable occurrence of high velocity trauma in the accident cases.
Paraplegia in spinal tuberculosis cases occurred in a higher majority of female patients than those of male patients; this can again be explained by a smaller spinal canal diameter and lesser immunity of females against the infection. While unlike trauma, there was equal involvement of mid dorsal spine and TLJ among the females and this suggests that the increased motion at the TLJ is not an important predisposing factor to increasing the risk of tuberculosis at the TLJ, and that there may be other factors contributing to this effect.
Conclusions
Spinal pathologies are increasing in the female population and explaining this, may have to do with the differences in flexibility of TLJ and differences in spinal canal diameters between the two sexes. Further epidemiological under-standing of spinal pathologies can lead to a better appreciation of the potential impact of health care management strategies and health policies to prevent and minimize consequences from such injuries [8]. A recent worldwide review found that sound epidemiological information on spinal injuries was only available in 41 countries, mostly for high-income European countries [9]. Thus, detailed epidemiological data from a large number of countries are still needed to fully understand the global burden of spinal pathologies, especially that from the developing and Asian countries.