Prevalence and Correlates of Low Back Pain in Primary Care: What Are the Contributing Factors in a Rapidly Developing Country
Article information
Abstract
Study Design
Cross-sectional.
Purpose
The purpose of the study was to determine the prevalence of low back pain (LBP) in the primary care setting with emphasis on the socio-demographic contributing factors and impact of LBP on lifestyle habits.
Overview of Literature
LBP is one of the most common medical conditions seen in the Primary Health Care Clinic.
Methods
A representative sample of 2,600 patients were approached and 1,829 subjects agreed to participate in this study (70.0%). Data on socio-demographic characteristics, life style habits and type of treatment were collected through a questionnaire.
Results
The prevalence of LBP in the study sample was 56.5% (95% confidence interval, 54.2-58.8). LBP was more prevalent among women (53.9%) compared to men (46.1%). There was significant difference between male and female patients of LBP in terms of ethnicity (p<0.001), marital status (p=0.010), occupation (p<0.001), monthly household income (p=0.004), and cigarette/sheesha smokers (p<0.001). The percentages of different aspects of functional disabilities were statistically significantly higher among females compared to male patients with LBP. Almost a quarter of female patients with LBP (26%) and 18% male patients with LBP reported pain in the arms and legs (p=0.002). In addition, gastrointestinal complaints such as abdominal pain and food intolerance were significantly higher among female patients with LBP as compared to males (31% vs. 24.6%, p=0.018; and 25% vs. 18%, p=0.008, respectively). Complaints about headache and fainting were also significantly higher among female patients as compared to male LBP patients (43% vs. 36%, p=0.029; and 26% vs. 20%, p=0.016, respectively). The multivariate logistic regression revealed that being female, prolonged standing, prolonged sitting, heavy weight lifting, weakness in the legs, regular exercise, and cigarette/sheesh a smoking had a significant effect on the presence of LBP.
Conclusions
LBP is highly prevalent among both genders and in older age. Also, weakness in the legs, smoking, prolonged standing and sitting had a significant effect on LBP. Furthermore, the current study findings support the fact that LBP continues to be an important clinical, social and economic, burden and a public health problem affecting the population of the entire world.
Introduction
Chronic low back pain (LBP) is a serious medical and social problem, and one of the most common causes of disability, and nearly everyone at some point suffers from LBP that interferes with work and recreational activities [1,2]. Nearly everyone gets LBP at least once in their lifetime, making the effective treatment of this common complaint become of widespread interest [1]. It is the most common reason for middle-aged people to visit their family doctor. In a few cases, there is a serious cause, but generally, it is not possible to identify a specific cause of the pain [3,4,5]. LBP is well documented to be an extremely common health problem; however, its burden is often considered trivial [3,4,5,6,7,8,9,10,11]. It is the leading cause of activity limitation and work absence and it causes enormous economic burden on individuals, families, communities, industry and governments [3]. In the past, it was documented that LBP is a common complaint in general practice in primary care settings [1,2,3,4,5,6,7,8,9]. The exact cause of pain cannot be identified in most instances. Recent studies continue to confirm that LBP is a common disorder in western and developing nations [3]. It is estimated [5] that about 80% of all populations will experience LBP at some period during their lifetime, and about 18% of the population experience LBP at any given moment each year, and 7% of the adult population consult their general practice with symptoms. The intercultural differences between nationalities in pain perception or pain reporting may be an explanation for the variation in prevalence rates among countries [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. It was largely thought of as a problem confined to western countries, but at the moment, due to the extensive amount of research on this problem, it has been demonstrated that LBP is also a major problem in low and middle income countries [1,2,3,4,5,6,7,10,11,12].
Bener et al. [10,11,12] reported in their previous study that LBP can have a substantial negative impact on the quality of life. Risk factors of LBP are multi-factorial, and include physical factors, social demographic characteristics, habits and psychological factors. The aim of the study was to determine the prevalence of LBP in the primary care setting, with emphasis on the socio-demographic contributing factors and the impact of LBP on lifestyle habits.
Materials and Methods
This is a cross sectional study and the study included subjects aged 15 to 65 years who attended primary health care centers throughout Qatar. The sample size was determined with the prior knowledge that the prevalence of LBP in the State of Qatar is similar to that in a neighboring country. A minimum sample size of 2,600 subjects aged between 15 and 60 years was calculated based on the prevalence of LBP in the United Arab Emirates [10,11,12] and other places, reported to be over 50%, with an allowed bound of 2.0% error of estimation and 99% confidence level. A representative sample of 2,600 patients were approached and 1,829 subjects agreed to participate in this study (70.0%). Primary health care centers are frequented by all levels of the general population as a gateway to specialist care. In order to secure a representative sample of the study population, the sampling plan was stratified with proportional allocation according to the stratum size of the Primary Health Care Clinics. The study was conducted among people who were visiting 13 health centers: 10 centers from an urban area and 3 centers from a semi-urban area, as a representative sample of the community. Data collection took place from March to December, 2012. Qualified nurses were trained to interview the patients and complete the questionnaires. The survey instrument was tested on 100 patients who visited the health centers, and thus the questionnaire was validated. The study excluded patients aged below 15 years and above 65 years, patients with any cognitive or physical impairment and those who refused to give consent to take part in the study.
1. Roland-Morris disability questionnaire
The Roland-Morris disability questionnaire (RDQ) is constructed by choosing statements from the sickness impact profile, which is a 136-item health status measure covering a range of aspects of daily living about physical and mental functioning [8,9]. This is a modified 24-item version of the Roland-Morris Scale for evaluating back disability. The scale consists of 21 yes/no items related specifically to physical functions to specifically assess the disability from LBP. The physical functions considered include walking, bending over, sitting, lying down, dressing, sleeping, self-care and daily activities. Patients are asked whether the statements apply to them that day (i.e., the last 24 hours). In the scale, one point is given for each item. The RDQ score can be obtained by adding up the number of items checked. The final score ranges from 0 (no-disability) to 21 (severe disability). The questionnaire is self-administered by the patient, it can be completed in a maximum of 5 minutes, and an unweighted score can be calculated in less than 1 minute.
The data was collected through a validated self-administered questionnaire with the help of qualified nurses. The questionnaire included socio-demographic details of the patients, associated factors like the physical life style pattern, triggering factors and type of treatment taken by patients for relief, for the data collection. Approval was obtained from the Hamad Medical Corporation Institutional Review Board for conducting this research in Qatar.
2. Statistical analysis
The Statistical Package for Social Sciences (SPSS) was used for the statistical analysis. Student's t-test was used to ascertain the significance of differences between the mean values of two continuous variables, and the Mann-Whitney test was performed for the nonparametric test. Chi-square analysis was performed to test for differences in the proportions of categorical variables between two or more groups. Stepwise logistic regression analysis was used to predict potential confounders and to rank the risk factors (determinants) for LBP (1=LBP, 2=without LBP); independent variables were a combination of continuous and categorical variables. The cut-off value for significance was considered to be p<0.05.
Results
Table 1 shows a comparison of socio-demographic and other characteristics between males and females with LBP. Among the subjects with LBP, 48% were males and 52% were females. There was a significant difference between male and female patients of LBP in terms of ethnicity (p<0.001), marital status (p=0.010), occupation (p<0.001), monthly household income (p=0.004) and cigarette/sheesha smoking (p<0.001). Nearly all the LBP characteristics were more common among females than males, particularly pain with any weakness in the leg (23% vs. 13.3%; p=0.025), prolonged standing (49.5% vs. 39.9%; p=0.026), prolonged sitting (45.4% vs. 38.1%; p=0.020), and lifting heavy weights (41.8% vs. 36.3%; p<0.039).

Socio demographic character of the low back pain patients according to gender (n=1,829)
Table 2 provides a comparison of functional disability between male and female patients with LBP. The percentages of different aspects of functional disabilities were statistically significantly higher among females compared to male patients with LBP.
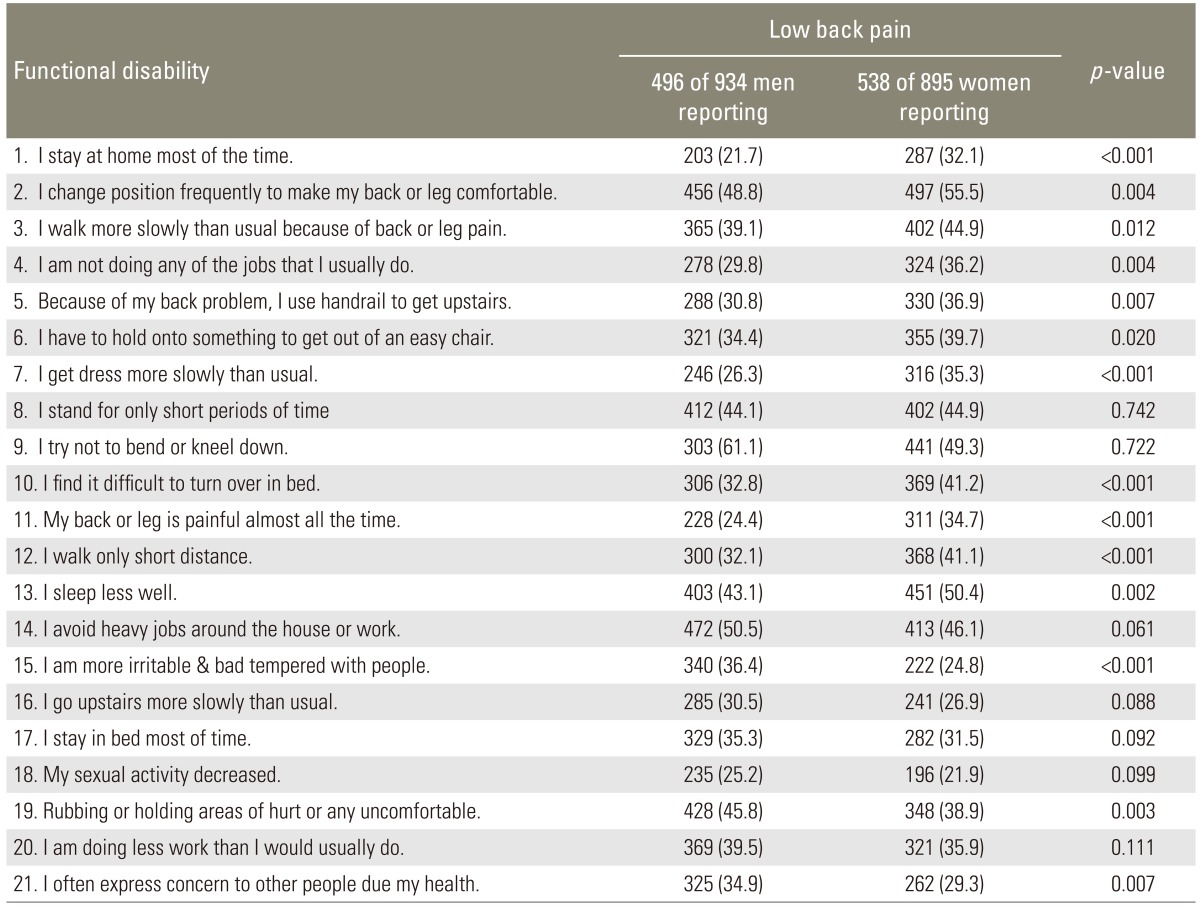
Functional disability in patients with recent onset of low back pain by gender (n=1,829)
Tablet 3 shows lifetime prevalence of somatization symptoms between male and female patients with LBP. Almost a quarter of the female patients with LBP (26%) and 18% of the male patients with LBP reported pain in the arms and legs (p=0.002). In contrast, a significantly higher proportion of male patients with LBP as compared to females complained about shortness of breath (26.2% vs. 20.4%; p=0.028) and palpitations (25.2% vs. 18.6%; p=0.010). In addition, gastrointestinal complaints such as abdominal pain and food intolerance were significantly higher among female patients with LBP as compared to male patients (31% vs. 24.6%, p=0.018; and 25% vs. 18%, p=0.008, respectively). Complaints about headache and fainting were also significantly higher among female patients as compared to male patients with LBP (43% vs. 36%, p=0.029; and 26% vs. 20%, p=0.016, respectively).
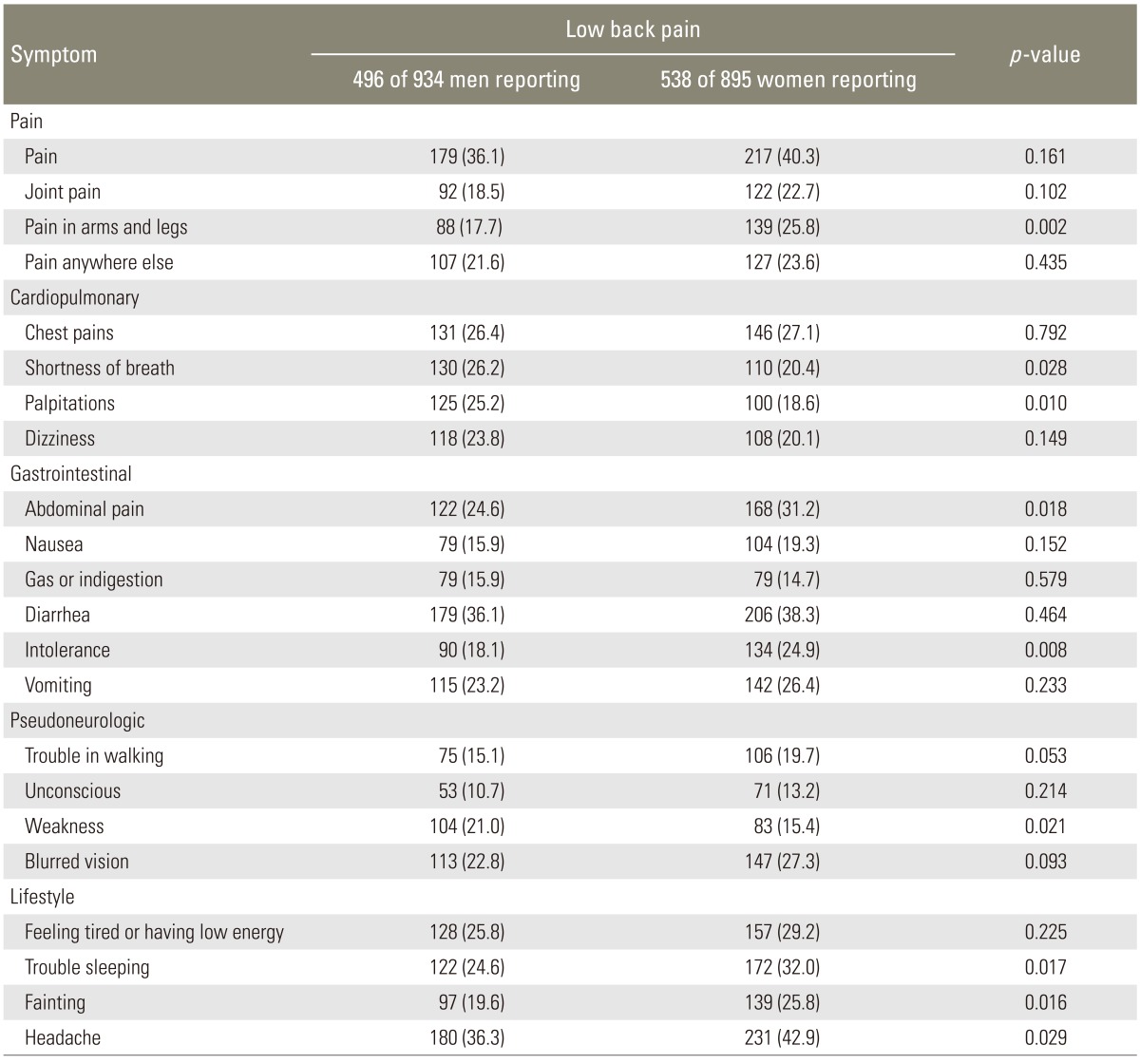
Lifetime prevalence of somatization symptoms of low back pian patients by Gender
Table 4 depicts the multivariable logistic regression analysis for the predictors of LBP. Being female (odds ratio [OR], 1.41; 95% confidence interval [CI], 1.14-1.74; p=0.001), having a lifestyle or job that demanded prolonged standing (OR, 1.70; 95% CI, 1.34-2.16; p<0.001), prolonged sitting (OR, 2.13; 95% CI, 1.62-2.80; p<0.001), heavy weight lifting (OR, 2.36; 95% CI, 1.76-3.17; p<0.001), weakness in the leg (OR, 1.52; 95% CI, 1.08-2.29; p 0.049), body mass index (BMI) more than 30 (OR, 2.31; 95% CI, 1.85-2.88; p<0.001) and cigarette/sheesha smoking (OR, 2.44; 95% CI, 2.20-2.71; p<0.001) were independently associated with LBP among the participants in Qatar.
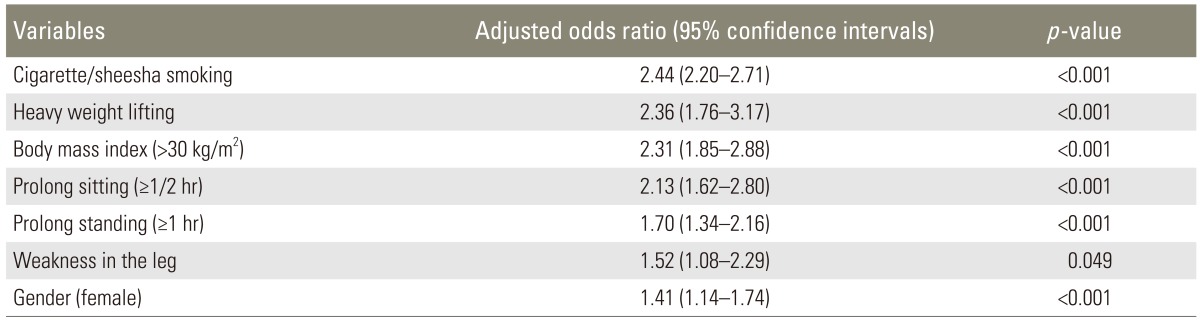
Stepwise logistic regression analysis for the predictors of low back pain
Fig. 1 examines the treatment taken by the studied LBP patients for relief. Most of them had bed rest (67.2%) followed by warm compression (47.6%), physiotherapy (47.5%), regular exercise (40%), and back plasters (33.5%).
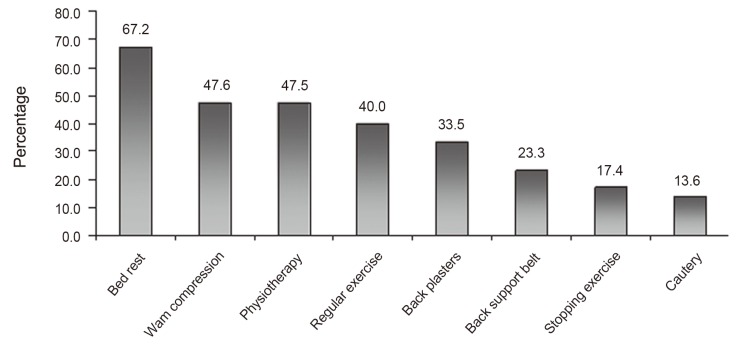
Treatment taken for relief by studied low back pain patients (n=1,034).
Discussion
This is the first study involving a primary care-based survey in Qatar. LBP is a multi-factorial disorder with many possible aetiologies. The present epidemiologic study of LBP analyzed various risk factors of LBP in a general population of Qatar. LBP is the most common health problem. Many factors have been demonstrated to be fundamental risk factors of LBP such as BMI, age, gender, occupation, socio-economic factors and other factors [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15]. The study focused on risk factors for LBP, attempting to analyse the socio-demographic characteristics, and individual and physical factors such as gender, age, nationality, BMI, lifestyle habits, physical straining, heavy lifting and postural stress. In the current study, the prevalence of LBP was 56.5 (95% CI, 54.2-58.8), which is in line with the rates observed in Denmark [13] (56%), Africa [14] (62%), and China [15] (64%). The prevalence rates observed in developed countries like Australia (25.6%) [16], Canada (28.7%) [17], the United Kingdom (36.1%) [18], and Sweden (39.2%) [19] were reasonably lower than the prevalence rate of this study. Fig. 2 compares the prevalence rate of LBP in the general populations of developed and developing countries. The prevalence rate of LBP in Qatar was much higher than the rate observed in developed countries like Canada (28.7%), the United Kingdom (36.1%), and Sweden (39.2%), and was very close to the rate in Africa (62%) and China (64%).
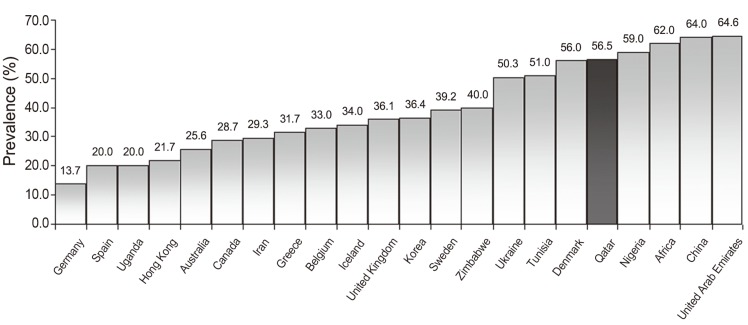
Global comparison of prevalence rates of low back pain in the general populations of developed and developing countries.
Previous reported studies in the UK [18] showed that the presence of LBP was associated with socio-demographic factors, among them sex, age, education level, smoking, and occupation. The present study also disclosed significant correlations between the frequency of LBP and socio-demographic factors, which is in accordance with earlier observations [1,2,3,4,10,11,12,20,21,22,23,24,25,26]. It is possible that LBP is more likely to be reported by those with a lower economic index and lower educational qualifications [3]. Higher education and economic status may provide knowledge or resources that influences the incidence of LBP to be lower. The present study found that LBP was higher in females compared to males. This is consistent with the previously reported studies [3,10,11,12,13,22,23,24] that showed that LBP symptoms were consistently more common among females. Schneider et al. [13] and Hathorn et al. [24] stated that the risk of LBP is higher among females due to the stress of hormonal changes, gynaecological problems and childbirth.
In the study sample, subjects with an educational level of high school graduation had a higher chance of developing LBP than those with college graduation. Low educational status, below the intermediate educational level, has been shown to be associated with an increased prevalence of LBP which is similar to the study findings of Kwon et al. [25]. Also, the majority of the LBP patients had clerical jobs. Among patients with LBP, more than half of the women (53.3%) were housewives, while most of the men (47.2%) had clerical jobs with a significant difference between both the genders in their occupations (p<0.001). Economic status was very low in the studied LBP patients with a monthly income. This confirms the results of a study reported by Waddel [26] and others [3,10,11,12] that showed the prevalence of LBP may be slightly greater in those from a lower socioeconomic class.
Obesity behaved as an important predictor, in agreement with the findings in the literature [3,10,11,20,22,27,28]. Shiri et al. [27] have reported that obesity is a risk factor for LBP in both cross-sectional and cohort studies. Biomechanics and metabolic factors have been suggested to explain this relation. Obesity may cause LBP through the metabolic syndrome, and it is also possible that obesity and LBP are linked more directly via inflammatory mechanisms [3]. Obesity has been shown as a risk factor for disc degeneration [1,2,3] and may increase the prevalence of LBP in this way. Because of a worldwide increase in the prevalence of obesity, it is reasonable to assume that the prevalence of back pain will continue to increase. Obesity and overweight status were significantly higher in men and women with LBP. Stepwise logistic regression revealed that obesity (BMI>30 kg/m2) was a strong contributing factor for LBP, which is in accordance with earlier studies [10,11,12,20,22,27,29] that showed that obesity or higher BMI was associated with an increased occurrence of LBP.
Life style habits have a great influence on LBP patients. It was reported [27,28,29] that factors such as heavy physical work, prolonged sitting or standing, bending, twisting, pulling and pushing have often been associated with LBP. This is consistent with previously reported studies [1,2,3,4,5,6,7,10,11,12].
In the present study, a smoking habit was significantly higher in LBP patients, with significant difference to healthy subjects, which is similar to a study [3,10,11,12,20,21,22] that showed that smoking was found to increase the risk for LBP patients. The association between smoking and LBP may be explained by the analgesic properties of nicotine [3]. Our results showed that smoking was consistently associated with LBP [3,10,11,12,20,21,22]. This is consistent with the previously reported studies that revealed that smoking was a strong contributing factor for LBP.
This study has several important limitations. First, the replies to the questionnaires were patients' self-reports and therefore current episodes of LBP may not be accurately represented. To counteract this problem, professional nurses were given training on LBP before the data collection process and they conducted the face-to-face interviews for the data collection. Also, all efforts were made to achieve the best estimates of LBP including the current episodes. Second, elderly patients were intentionally excluded. Third, this dataset probably did not distinguish precisely between incident and prevalent cases of back pain. Therefore the factors found on logistic regression to be associated with LBP represent a combination of risk and prognostic factors.
This cross-sectional study showed that LBP is highly prevalent among both genders and in older age. Also, weakness in the legs, smoking, and prolonged standing and sitting had a significant effect on LBP to the point that it compromised patients' daily lives and work habits significantly. Furthermore, the current study's findings support the fact that LBP continues to be an important clinical, social and economic burden and a public health problem affecting the population of the entire world.
Acknowledgments
This work was generously supported and funded by the Qatar Foundation, UREP Grant No. 11-074-3-015. The authors would like to thank Hamad Medical Corporation for their support and granting ethical approval (HMC RP# 12061/12).
Notes
No potential conflict of interest relevant to this article was reported.