Outcomes of Fluoroscopically Guided Lumbar Transforaminal Epidural Steroid Injections in Degenerative Lumbar Spondylolisthesis Patients
Article information
Abstract
Study Design
A prospective cohort.
Purpose
To report the short and long term outcomes of fluoroscopically guided lumbar transforaminal epidural steroid injection (TFESI) in degenerative lumbar spondylolisthesis (DLS) patients.
Overview of Literature
TFESI has been widely used for the treatment of lumbosacral radicular pains. However, to our knowledge, there has been no study which has evaluated the outcomes of TFESI in patients with DLS.
Methods
The DLS patients received fluoroscopically guided lumbar TFESI with 80 mg of methylprednisolone and 2 mL of 1% lidocaine hydrochloride. Patients were evaluated by an independent observer before the initial injection, at 2 weeks, at 6 weeks, at 3 months, and at 12 months after the injections. Visual analog scale (VAS), Roland 5-point pain scale, standing tolerance, walking tolerance, and patient satisfaction scale were evaluated for outcomes.
Results
Thirty three DLS patients treated with TFESI, who were completely followed up, were included in this study. The average number of injections per patient was 1.9 (range from 1 to 3 injections per patient). Significant improvements in VAS and Roland 5-point pain scale were observed over the follow up period from 2 weeks to 12 months. However, the standing and walking tolerance were not significantly improved after 2 weeks. At 2 weeks, the patient satisfaction scale was highest, although, these outcomes declined with time. The DLS patients with one level of spinal stenosis showed significantly better outcome than the DLS patients with two levels of spinal stenosis. Five patients (13%) underwent surgical treatment during the 3 to 12 months follow up.
Conclusions
TFESI provides short term improvements in VAS and Roland 5-point pain scale, standing tolerance, walking tolerance and patient satisfaction scale in DLS patients. In the long term, it improves VAS but limits the improvements in Roland 5-point pain scale, standing tolerance, walking tolerance and patient satisfaction scale.
Introduction
Degenerative lumbar spondylolisthesis (DLS) is a common cause of low back pain, radiculopathy and neurogenic claudication in adults. The superior vertebra slides forward on the inferior resulting in a narrowed central canal and lateral recesses which lead to a wide range of clinical presentations. There are various types of non-operative treatments for DLS such as medication, physical therapy, strengthening exercises or spinal manipulation. If the patients do not respond to such treatments within 4 to 6 weeks, they may benefit from an epidural steroid injection [1].
Epidural steroid injection has been used for the treatment of low back pains and leg pains for more than 50 years [2]. Several techniques and approaches have been developed to deliver the highest concentration of steroids to the target site of pathology without complications. Fluoroscopy with epidurography has been used to ensure the localization of needles within the epidural space. Even in experienced hands, the epidural steroid without the use of fluoroscopy or contrast media may be misplaced from the intended target in 30% of cases [3,4]. For lumbar spine, there are three approaches for epidural steroid injections, namely: transforaminal, interlaminar and caudal. According to systematic reviews, successful evidences of caudal epidural steroid injections in spinal stenosis are limited [5,6]. Fluoroscopic guided transforaminal epidural steroid injection (TFESI) has several advantages such as the accuracy, specific targeting, and safety with low volumes of injectate. For foraminal spinal stenosis, TFESI is usually selected initially and, for the stenosis of the upper lumbar central canal, the interlaminar epidural steroid injection is the first choice of treatment [7]. Currently, fluoroscopically guided TFESI is frequently being used for treatment of radicular pains in lumbar disc herniation, spinal stenosis and degenerative disc disease patients with various results. However, to our knowledge base on MEDLINE literature reviews, there has been no study which has exclusively evaluated the effectiveness of epidural steroid injections in patients with DLS.
The objectives of this study are to report the short- and long-term outcomes of fluoroscopically guided lumbar TFESI in DLS patients.
Materials and Methods
After approvals from our institutional review board, 38 DLS patients who underwent fluoroscopically guided lumbar TFESI during April 2009 to March 2010 were enrolled. There were 13 men and 25 women with an average age of 62 years (range, 44-81 years). All of the patients were provided with informed consents before being included in this study. The inclusion criteria were as follows: 1) patients with history of low back pain and unilateral radiating pain at least below the knee joint; 2) patients with slip grade 1 degenerative lumbar spondylolisthesis, visible on plain radiographs and one or two levels of neural compression found from the magnetic resonance imaging (MRI); 3) failures of conservative treatment by physiatrists for at least 6 weeks. These patients then received fluoroscopically guided lumbar TFESI according to the first author. The patients who had previous surgery at the lumbar spine, pars defects, previous history of epidural steroid injections, allergies to contrast media, gross neurological deficits, cauda equina syndrome or inflammatory joint diseases were excluded from the study. The patients were classified into 2 groups according to MRI findings with one or two levels of spinal canal stenosis. The patients with a single level of spinal stenosis received one level of fluoroscopically guided lumbar TFESI and the patients with two levels of stenosis, either one or two levels DLS, received two levels of fluoroscopically guided lumbar TFESI. The purpose of the different injection technique aimed to deliver the injectate as closely as possible to the pathology. Moreover, in severe lateral stenosis, the injectate could not be widely distributed.
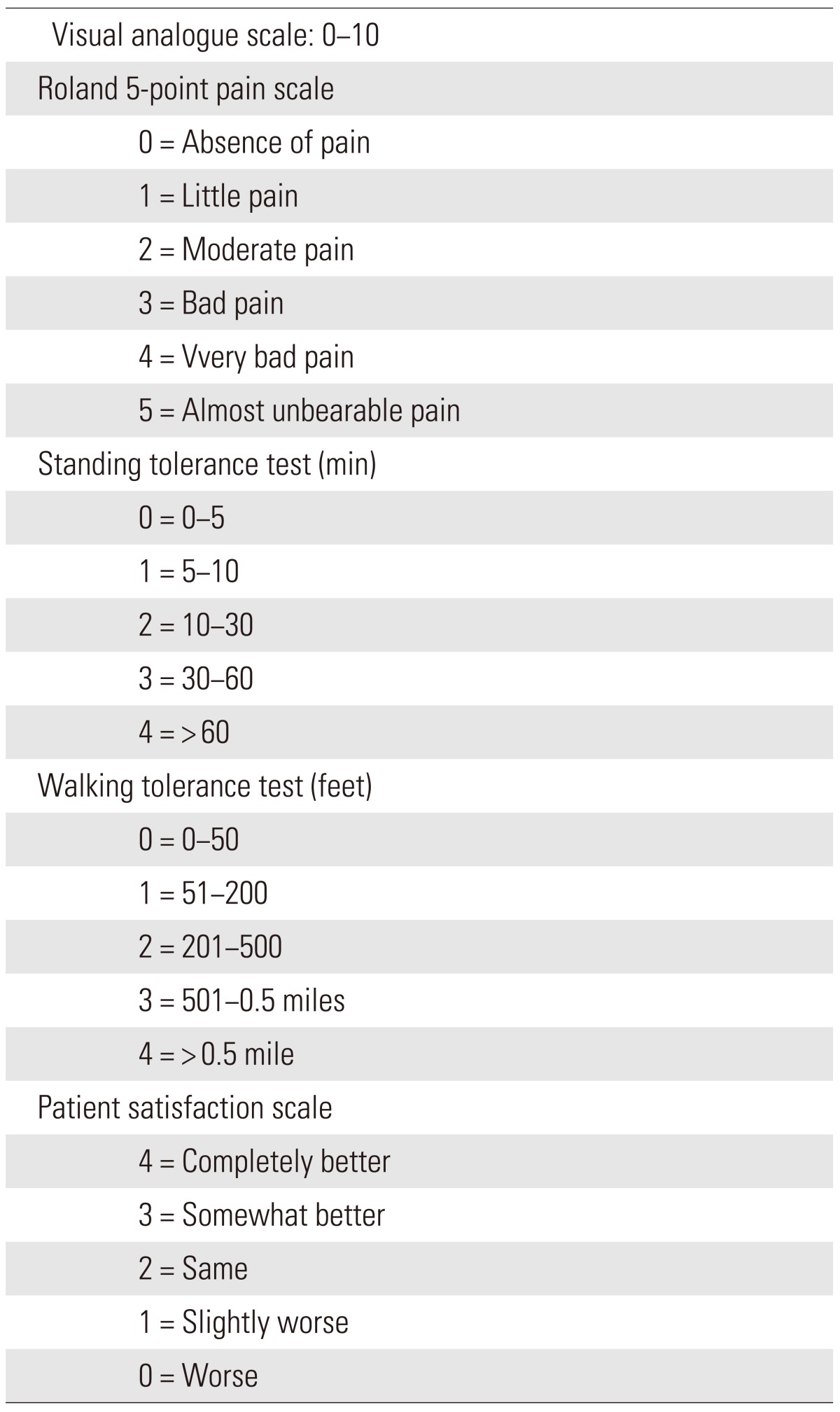
The patients were evaluated by an independent observer before the initial injection (pre-injection), at 2 weeks, at 6 weeks, at 3 months, and at 12 months after the injections. The back pain, leg pain and neurological deficit of the patients were recorded. The visual analog scale (VAS), Roland 5-point pain scale, standing tolerance, walking tolerance and patient satisfaction scale were evaluated for the outcome measurements according to Botwin et al. (Table 1) [8]. At the follow up after injection, if the patients' symptoms were not improved, the patents were treated with reinjections or received operative treatments.
1. Procedure description
The patient was put in a prone position on a radiolucent operating table. Then the C-arm fluoroscope was positioned to identify the level of spine and observe the foramen of the target level. The fluoroscopically guided lumbar TFESI level was performed using the preganglionic approach [9]. Local anesthetic (1% lidocaine HCL [Xylocaine, AstraZeneca]) was then injected to the skin, subcutaneous tissues and the muscles where the needle is usually placed. Next, a 22-gauge spinal needle was advanced in the foramen underneath the pedicle using fluoroscopic guidance. Contrast media (Iopamiro, Bracco Industria Chemica SpA, Milan, Italy) was injected to confirm the epidural spreading (Fig. 1). After that, Depo-Medral (Pharmacia & Upjohn Company, New York, NY, USA) 2 mL (80 mg) with 1% lidocaine hydrochloride 2 mL were slowly injected. Finally, the patient was observed in the recovery room under standard protocol. If the patient was free from any complications then the patient was discharged.

Anteroposterior (A) and lateral (B) fluoroscopic projection of preganglionic transforaminal epidural steroid injection in lumbar spondylolisthesis patient showing contrast outlining L4 existing nerve root and spreading into epidural space.
2. Statistical analysis
Statistical analysis was performed using the STATA software ver. 10.0 (Statacorp Lp, College Station, TX, USA). The Wilcoxon rank sum test was used for the comparison in each parameter between pre-injection and post-injection outcome measurements at various time points. Additionally the comparison among outcome measurements between one level of stenosis and two levels of stenosis were determined using analysis of variance. The difference was considered significant if p<0.05.
Results
Thirty eight DLS patients underwent fluoroscopically guided lumbar TFESI. The most common level of DLS was L4-L5 (69%). All of the patients had experienced unilateral leg pains. Six of them (16%) had no back pains. On initial neurological examination, there were no major neurological deficits found. Fourteen patients (37%) have had mild extensor hallucis longus weaknesses. During 3 to 12 months of follow up, 5 patients underwent surgical treatments (4 due to intractable pains with severe neurogenic claudication, and 1 due to weakness of ankle dorsiflexion). The four patients with intractable pains responded well to TFESI during the first 6 weeks but later developed recurring pains. Three of them had DLS with 2 levels of spinal stenosis and, one of them had DLS with 1 level of spinal stenosis. A total of 33 patients completed follow ups at 1 year and their data were collected for analysis. There were 24 patients (73%) with a one level stenosis and 9 patients (27%) with two levels of stenosis. The average numbers of injection per patient was 1.9 (range, 1 to 3 injection per patient). There were no major complications reported from patients after the injection procedures. There were 3 patients who experienced worsening leg pains after injections but these symptoms resolved spontaneously after a few days.
1. Comparison of pre-injection and post-injection
The four outcome measurements: VAS, Roland 5-point pain scale, standing tolerance and walking tolerance of pre-injection were compared with post-injection at 2 weeks, 6 weeks, 3 months, and 12 months. Meanwhile, the patient satisfaction scale at 2 weeks post-injection was compared with 6 weeks, 3 months, and 12 months post-injection as shown in Table 2.
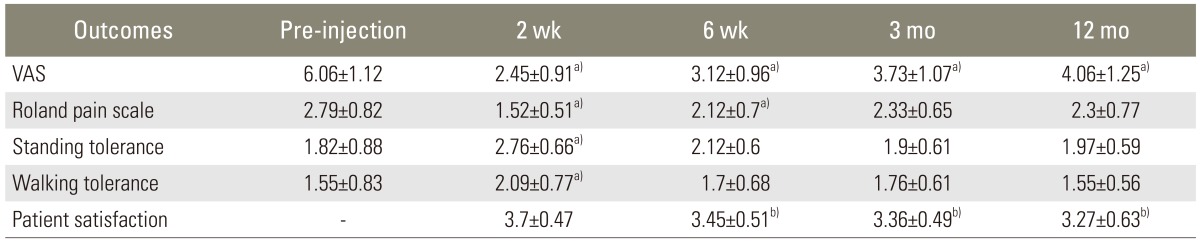
Outcomes of TFESI in DLS patients pre-injection and at 2 weeks, 6 weeks, 3 months, and 12 months follow up assessments
There were significant decreases in VAS scores between pre-injection and post-injection at 2 weeks, 6 weeks, 3 months and 12 months (p<0.001). The Roland 5-point pain scale between pre-injection and post-injection were significantly improved at 2 weeks and 6 weeks (p<0.001) respectively but were not significantly different from the pre-injection scores at 3 months and 12 months (p=0.09 and p=0.091, respectively).
For standing tolerance and walking tolerance, the significant difference was found only between pre-injection and post-injection at 2 weeks (p<0.001). At 6 weeks, 3 months and 12 months, there were no significant improvements in standing tolerance and walking tolerance, (p>0.05).
For the patient satisfaction scale, there were significant decreases in satisfaction between post-injection at 2 weeks and post-injection at 6 weeks, 3 months and 12 months (p=0.02, p=0.002, and p=0.005, respectively).
2. Comparison of one level of stenosis with two of levels stenosis
Analysis of variance was used for comparing the outcome measurements after TFESI of one level stenosis DLS patients with two level stenosis DLS patients as shown in Table 3.

Outcomes of TFESI in DLS patients when compared between one level stenosis with two levels stenosis
The VAS of both groups post-injection (2 weeks, 6 weeks, 3 months, and 12 months) were significantly lower than pre-injection (p<0.001). When compared between groups, the VAS of one level of stenosis DLS patients post-injection was significantly lower than the VAS of two level of stenosis DLS patients (p=0.012) as shown in Fig. 2.

Line graph showing the VAS of one level of stenosis DLS patients and two levels of stenosis DLS patients over time. There was a significant difference (p=0.0124) between these two groups. VAS, visual analog scale; DLS, lumbar spondylolisthesis.
The Roland 5-point pain scale of one level of steno-sis DLS patients post-injection (2 weeks, 6 weeks, and 12 months) were significantly lower than pre-injection (p<0.001) while in two levels of stenosis DLS patients, the Roland 5-point pain scale post-injection was signifi-cantly lower than pre-injection (p=0.001) at 2 weeks. When compared between groups, the Roland 5-point pain scale of one level of stenosis DLS patients post-injection was significantly lower than the Roland 5-point pain scale of two levels of stenosis DLS patients (p=0.012) as shown in Fig. 3.

Line graph showing the Roland 5-point pain scale of one level of stenosis DLS patients and two levels of stenosis DLS patients over time. There was a significant difference (p=0.004) between these two groups. DLS, lumbar spondylolisthesis.
The standing tolerance of one level of stenosis DLS patients post-injection at 2 weeks was significantly higher than pre-injection (p<0.001) while in two levels of stenosis DLS patients, there was no significant differences in the standing tolerance between pre-injection and post-injection (p=0.218). When compared between groups, the standing tolerance of one level of stenosis DLS patients post-injection was significantly higher than the standing tolerance of two levels of stenosis DLS patients (p<0.001) as shown in Fig. 4.

Line graph showing standing tolerance of one level of stenosis DLS patients and two levels of stenosis DLS patients over time. There was a significant difference (p<0.001) between these two groups. DLS, lumbar spondylolisthesis.
The walking tolerance of one of level stenosis DLS patients post-injection at 2 weeks was significantly higher than pre-injection (p<0.012) while in two levels of stenosis DLS patients, there were no significant differences of the walking tolerance between pre-injection and post-injection (p=0.510). When compared between groups, the walking tolerance of one level of stenosis DLS patients post-injection was significantly higher than the walking tolerance of two levels of stenosis DLS patients (p<0.001) as shown in Fig. 5.
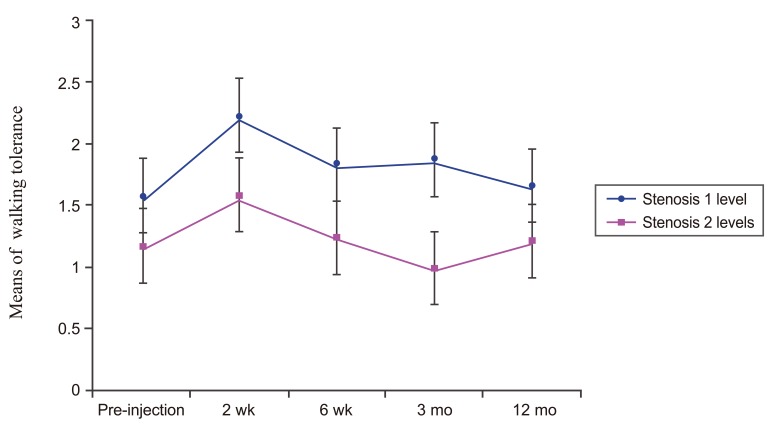
Line graph showing walking tolerance of one level of stenosis DLS patients and two levels of stenosis DLS patients over time. There was a significant difference (p<0.001) between these two groups. DLS, lumbar spondylolisthesis.
There were no significant differences of the patient satisfaction scale post-injection of both groups (p=0.2072 and p=0.023, respectively); except at 12 months, when the patient satisfaction scale was significantly lower than at 2 weeks (p<0.05). When compared between groups, there was no significant difference in the patient satisfaction scale between both groups as shown in Fig. 6.

Line graph showing the patient satisfaction scale of one level of stenosis DLS patients and two levels of stenosis DLS patients over time. There was no significant difference (p=0.058) between these two groups. DLS, lumbar spondylolisthesis.
Discussion
DLS is one of the common degenerative changes in the lumbar spine. The pathology and clinical presentation of DLS patients are different from the other degenerative changes of the lumbar spine. The pathology of DLS is overall problems of disc degeneration, facets arthrosis, central and lateral spinal canal stenosis with instability of ligaments and muscles [10,11].
Epidural steroid injection has been used for treating lumbar disc herniation, lumbar disc degeneration and spinal stenosis.
There are several systematic reviews of TFESI in lumbar disc herniation which have shown favorable results especially in short term pain reliefs. However, in chronic axial low back pains from lumbar disc degeneration, the results of epidural steroid injections still lack well-designed studies [12,13,14]. For lumbar spinal stenosis, several studies have been published which evaluates epidural steroid injection with caudal epidural injection techniques [15,16,17,18,19], and TFESI techniques [8,20]. However, most of the population in the studies includes both spinal stenosis and DLS patients which cause inconsistent results, therefore, we chose to study the outcomes of epidural steroid injection exclusive to DLS patients.
There are many techniques of epidural steroid injection which have demonstrated different results. Schaufele et al. [21] reported that TFESI was superior to the interlaminar epidural steroid injections for treating lumbar disc herniation. Smith et al. [22] later reported no significant differences between TFESI and interlaminar epidural steroid injection for treating lumbar spinal stenosis. Abdi et al. [23] showed the evidence that lumbar TFESI is more effective than lumbar interlaminar epidural steroid injections. In the treatment of lumbar root pains, TFESI is strong for short term and moderate for long term efficacy. In contrast, the lumbar interlaminar epidural steroid injection is strong for short term reliefs and limited for long term efficacy. Botwin et al. [8] reported a prospective cohort study of 34 spinal stenosis patients who underwent fluoroscopically guided TFESI. They reported 75% of long term successful outcomes (at least 50% pain reduction post injection), a 64% improved walking tolerance and a 57% improved standing tolerance. With superior outcomes as mentioned above, we decided to use the TFESI technique for this study.
The results from our study showed that, TFESI significantly reduced VAS and Roland 5-point pain scores for both short term and long term follow ups. However, standing tolerance and walking tolerance only significantly improved in the short term (for 2 weeks), but in the long term there was no significant difference. The patient satisfaction scale for this procedure was highest at 2 weeks and declined with time.
These results may be explained by the multiple problems in the pathology of DLS as previously described. Corticosteroid has direct anesthetic effects by blocking the nociceptive c-fiber conduction and also inhibits phospholipase A2 activity which is found in injured nerves [24,25]. Therefore, it can reduce inflammatory pain which explains the reduction of VAS and Roland 5-point pain scores. However, neurogenic claudication and mechanical pain may not respond well with corticosteroid which is only shown by a fair improvement of standing tolerance and walking tolerance.
The outcome measurements were compared between one level of spinal stenosis DLS patients and two levels of spinal stenosis DLS patients after TFESI. All parameters indicated better outcome in one level of spinal stenosis patients than in two levels of spinal stenosis patients. These findings may be explained by the poor neural structures and physiology caused by double compression sites in neural elements.
The experiments by Olmarker and Rydevik [26] demonstrated that double level compressions induced more abnormal changes in nerve impulse conduction than one level. Takahashi et al. [27] studied the neural blood flow in pigs and reported that double level compressions of the cauda equina can induce impairment of blood flows at the compression site and intermediate nerve segments even at low pressures of compression which may cause dysfunctions of nerve impulse conduction. These studies support the poor results on two levels of spinal stenosis in DLS patients after TFESI.
Our study has some limitations. First, the sample size was small. We tried to select only patients with DLS who had prominent unilateral leg pains. For this homogenous group of patients, we avoided using various techniques of injections. However, some patients had DLS with one level stenosis, while the others had DLS with two levels of spinal stenosis. There has been no study for the outcomes of one needle TFESI as compared with two needles TFESI. For the benefit of the patients with two levels of spinal stenosis, we used two needles TFESI as mentioned in the methods. Another limitation was the numbers of injections were not the same for every patient. Repeated injections were done in patients with symptom recurrences.
Conclusions
The fluoroscopically guided lumbar TFESI is able to reduce VAS and Roland 5-point pain scale and improves standing tolerance and walking tolerance in the short term for DLS patients. For long term results, it reduces VAS but the improvement in standing tolerance and walking tolerance are limited. In addition, DLS patients with one level of spinal stenosis showed significantly better outcomes than DLS patients with two levels of spinal stenosis.
Notes
No potential conflict of interest relevant to this article was reported.