Introduction
Low back pain has a worldwide prevalence of 30% to 40% [1,2]. The total costs due to low back pain in the United States exceed $100 billion per year [3]. Approximately 40% of all lower back pain has been found to be discogenic in origin [4]. Discogenic low back pain may result from a disc prolapse or degenerative disc disease (DDD). Successful outcomes after discectomy for disc prolapse have been reported [5,6]. However, the patients with small, contained degenerated discs have been found to be poor candidates for discectomy, as their clinical outcomes are less favorable [7].
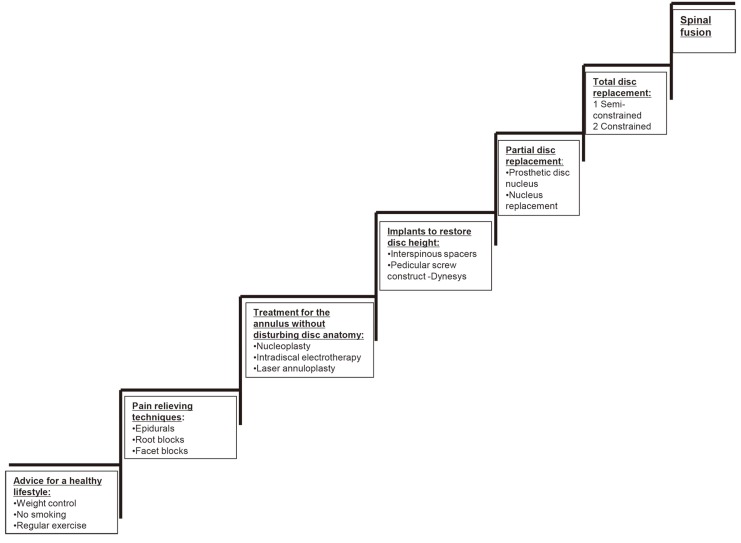
Discogenic low back pain from DDD has been traditionally managed with non-operative methods or by the major surgical interventions such as spinal fusion. In recent years, several minimally invasive techniques have been developed to treat discogenic low back pain. These techniques aim at reducing the intradiscal pressure and thus decompress the disc, which in turn relieves pressure on the nervous tissue [8]. The treatment approach for the low back pain secondary to DDD is highlighted in Fig. 1.
Nucleoplasty is a minimally invasive technique that was first approved by the US Food and Drug Administration in 2000 [9]. It aims to achieve percutaneous disc decompression through a patented coblation technology, which utilizes the bipolar radiofrequency energy to ablate and remove the disc material, with a coagulation of the adjacent residual disc tissue. There is weak evidence that nucleoplasty is effective in the treatment of radicular leg pain due to contained disc herniation. However, there is no evidence available with regards to its role in managing discogenic axial back pain [10].
Thus, the aim of our study was: 1) to evaluate the role of nucleoplasty in the management of discogenic axial back pain, which failed conservative treatments; 2) to determine the influence of concordant pain during provocative discography, presence of annular tear and loss of disc height on the outcome of nucleoplasty.
Materials and Methods
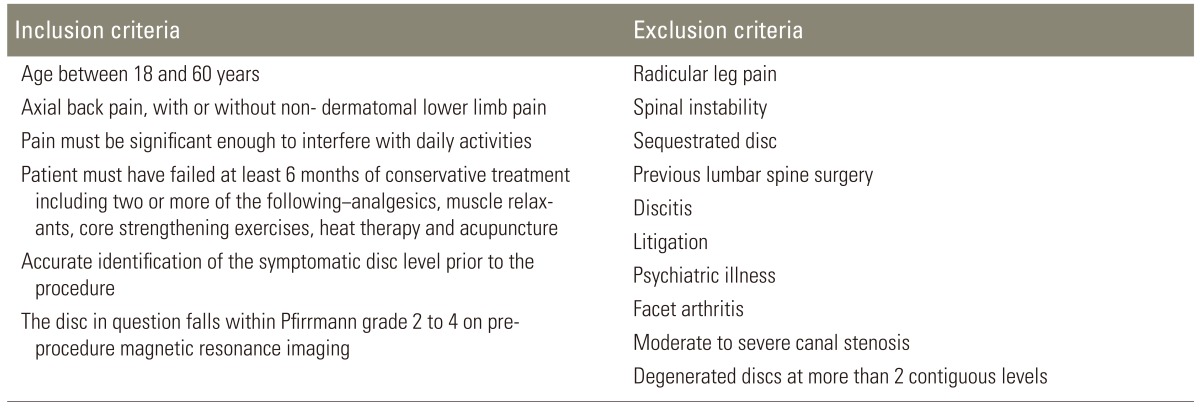
The Institutional Review Board's approval was obtained prior to the commencement of the study. Patients presenting to the senior author (N.S.K) with discogenic axial back pain were identified. The discogenic nature of the problem was ascertained clinically and radiologically. The patients who satisfied the criteria detailed in Table 1 were offered nucleoplasty for their symptoms. They were also informed that the discography would precede the nucleoplasty procedure. All the patients who accepted nucleoplasty for their symptoms were included in the study. Between October 2008 and December 2009, 30 such patients were recruited and followed up prospectively. None of the patients were lost to the follow-up at 12 months. Magnetic resonance imaging (MRI) of the recruited patients were analyzed for the following: the level at which the degenerate discs were present; severity of the disc degeneration according to the Pfirman's grading [11]; and the presence of annular tear and loss of disc height. All patients were assessed for pain, functional disability and quality of life using 100 mm visual analogue scale (VAS), Oswestry Disability Index (ODI) and Short Form-36 (SF-36), respectively, prior to the procedure.
1. Procedure
All patients were managed in the short-stay ward. A prophylactic dose of 1 g cefazolin was administered intravenously 1 hour prior to the procedure. Discography preceded nucleoplasty in every case. With the patient in a prone position, the procedure was carried out under local anesthesia with sedation and under the image intensifier guidance. A 17-gauge needle was introduced via a posterolateral approach towards the identified disc level and advanced into the central third of the disc. After confirming the position of the needle tip, a nonionic contrast dye (Omnipaque 350, GE Healthcare, Cork, Ireland) was injected into the disc. Concordance of pain was noted at the level in question and was validated with a control disc. After the discography, a coblation bipolar device (Perc DLG SpineWand connected to ArthroCare System 2000, Arthrocare, Sunnyvale, CA, USA) was inserted into the disc through the same needle. Disc decompression was achieved through 6 standard coblation channels, which were created by advancing the coblation bipolar device in the ablation mode and retracting it in the coagulation mode. After the withdrawal of the coblation bipolar device, 2 mL of 0.25% bupivacaine was injected into the nucleoplasty tract, but not intradiscally. All patients were observed for 24 hours postoperatively for any development of neurological deficit or other procedure-related problems.
Periodic reviews were performed at 6 weeks, 3 months, 6 months, and 12 months. At the 6 months and 12 months follow-up, patients were assessed for the residual and/or new symptoms, and their outcome scores were evaluated.
The minimum clinically important difference (MCID) for each of the three clinical outcome indicators was defined as follows: 1) A decrease in VAS score by 30 points or more [12]. 2) A decrease in ODI score by 12.8 points or more [13]. 3) An increase in SF-36 score by 5 points or more [13].
The overall clinical outcome was defined as: Excellent, clinically significant improvement in all three clinical outcome indicators (VAS, ODI, SF-36); Good, clinically significant improvement in any two outcome indicators; Fair, clinically significant improvement in any one outcome indicator; and Poor, no clinically significant improvement in any of the outcome indicators.
2. Statistical analysis
Patient's demographic and baseline clinical data were analyzed descriptively. The VAS, ODI, and SF-36 scores at 6 months and 12 months after the nucleoplasty procedure were compared with the respective pre-procedure scores using paired t-test. The mean reduction in VAS and ODI scores and mean improvement in SF-36 scores were estimated, and the point estimates with 95% confidence interval (CI) were reported. The influence of concordant pain during provocative discography, presence of annular tear and loss of disc height on the clinically significant improvement in any of the three outcomes (VAS, ODI, and SF-36) were evaluated, using the generalizing estimating equations (GEE) model. All statistical analyses were performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
Results
1. Patient demographics
A total of 30 patients were recruited for the study, which included 25 (83.30%) males and 5 (16.70%) females. The mean age of the study population was 35 years (range, 20-57 years). Nineteen (19/30, 63.30%) patients had nondermatomal lower limb pain along with axial back pain. Majority of the patients (23/30, 76.70%) were symptomatic for more than 12 months. Fifteen (50%) patients had a loss of disc height, and 11 patients (36.70%) had annular tears at the disc level in question on the preoperative MRI. Nucleoplasty was performed at single level in 24 patients and at two levels in six patients. Thus a total of 36 discs were treated as follows: L2-3 disc, one; L3-4 disc, one; L4-5 disc, 13; and L5-S1 disc, 21. Concordant pain during discography was seen in 19 (19/30, 63.33%) patients.
2. Pain reduction (VAS)
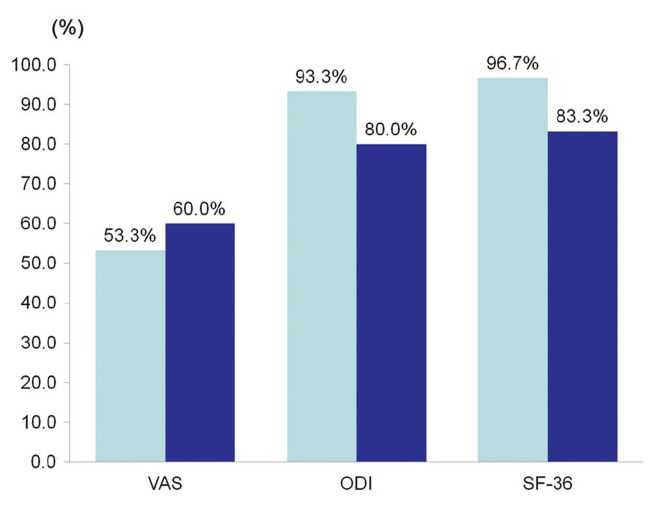
Clinically significant pain reduction was seen in 53.30% and 60% of the patients at 6 months and 12 months after the procedure, respectively (Fig. 2). The mean reduction in VAS score was 31.03 (95% CI, 26.73-35.34, p<0.05) and 29.03 (95% CI, 23.66-34.40, p<0.05) at 6 months and 12 months, respectively (Fig. 3). The scores indicated a statistically, but not clinically, significant mean improvement. The baseline VAS score significantly influenced the post procedure improvement in the VAS score (p=0.010).
3. Functional disability reduction (ODI)
Clinically significant reduction in the functional disability at 6 months and 12 months was seen in 93.30% and 80% of patients, respectively (Fig. 2). The mean reduction in ODI score was 24.53 (95% CI, 21.15-27.92; p<0.05) and 20.600 (95% CI, 16.90-24.30; p<0.05) at 6 months and 12 months, respectively (Fig. 3). The mean reduction in ODI score was both statistically and clinically significant. Baseline ODI score did not influence the post procedure improvement in the ODI score significantly (p=0.109).
4. Improvement in quality of life (SF-36)
Clinically significant improvement in quality of life at 6 months and 12 months was seen in 96.70% and 83.30% of patients, respectively (Fig. 2). The mean increment in the SF-36 score was 13.58 (95% CI, 11.41-15.75; p<0.05) and 12.30 (95% CI, 9.50-15.11; p<0.05) at 6 months and 12 months, respectively (Fig. 3). The scores indicated both statistically and clinically significant mean improvements. The baseline SF-36 score did not influence the post procedure SF-36 score significantly (p=0.590).
5. Correlation between other variables and clinical outcome after nucleoplasty
The GEE model demonstrated that none of the following variables-concordant pain during discography, presence of annular tear or presence of loss of disc height-influenced clinically a significant improvement in any of the 3 outcomes (p=0.882, 0.213, and 0.170; respectively). However, the patients with a loss of disc height improved 7.5 points more in ODI (95% CI, 0.50-10.38, p<0.05), compared to the patients with preserved disc heights, across both time points.
There was no significant change in the clinically significant improvements achieved in all 3 outcomes at the end of 6 months and 12 months (p=0.478).
While assessing the overall clinical outcomes, Good to Excellent results were seen in 28 patients (28/30, 93.33%) at the end of 6 months and were sustained in 22 patients (22/30, 73.33%) at the end of 12 months.
Discussion
The biomechanical and biochemical effects of nucleoplasty on the intervertebral discs have been well established. Chen et al. [14] showed in a human cadaveric study that nucleoplasty reduced the intradiscal pressures significantly, especially in the younger, healthy discs. In 2003, Chen et al. [15] demonstrated the safety of nucleoplasty in a porcine model. He showed that the procedure achieved a volumetric reduction of the target disc tissues without overt thermal or structural damages to the adjacent tissues. Lee et al. [16] reconfirmed the safety of nucleoplasty in the sheep intervertebral discs. In 2004, O'Neill et al. [17] demonstrated the significant biochemical changes in the degenerate porcine discs after nucleoplasty in the form of a decrease in Interleukin-1 and increase in interleukin-8. These changes were consistent with the mechanism of pain relief.
Several studies have found favorable results with nucleoplasty in the treatment of leg pain without axial symptoms. Bokov et al. [18] found that nucleoplasty provided a significant relief of leg pain and faster recovery compared to microdiscectomy in patients with contained disc herniations. Mirzai et al. [19] prospectively evaluated the results of nucleoplasty in 52 patients with disc herniations causing leg pain, with respect to pain reduction, patient satisfaction, functional disability and analgesia requirement. They reported a mean reduction in pain by >50%, patient satisfaction >80% and good results in the functional disability improvement and analgesia requirement. Gerszten et al. [20], in their study of 67 patients with primary radicular leg pain due to disc herniations, concluded that nucleoplasty is a safe and viable minimally-invasive technique that improved leg pain and quality of life in patients with contained disc herniations. In contrast, a smaller study on 16 patients with leg pain by Cohen et al. [21] concluded that nucleoplasty was not an effective treatment of lumbar radiculopathy, as the mean pain scores did not improve significantly and only one patient achieved >50% reduction in the VAS score. Despite these encouraging studies, it is imperative to note that nucleoplasty is still not considered a substitute for microdiscectomy and is suitable for patients with the relatively small and contained disc herniations.
In addition to the use of nucleoplasty in the pure radicular leg pain, several studies have included axial back pain along with leg pain in the inclusion criteria. In 2002, Singh et al. [22] studied 67 patients with contained disc herniations and concluded that nucleoplasty is effective in treating discogenic back and/or leg pain in patients who failed conservative management and are not candidates for open surgery. Their conclusion was based on significant improvements at 12 months in pain and function. Al-Zain et al. [23] conducted a prospective study on 96 similar patients treated with nucleoplasty and found that 73% of the patients achieved a >50% improvement in the VAS score at the early follow-up, with a decrease in the analgesia requirement, disability and work incapacitation. However, the improvements in the outcomes decreased over time.
There is a paucity of literature focusing on the success of nucleoplasty in the treatment of the isolated discogenic axial back pain. In 2004, Singh et al. [24] published a prospective study involving 47 patients with predominantly axial back pain secondary to disc herniation, treated with a nucleoplasty and followed up for 12 months. They found significant improvements in pain and function at all follow-ups, although the ratio of patients showing significant improvements decreased over time. Our study endeavors to provide further evidence substantiating the role of nucleoplasty in the treatment of isolated discogenic axial back pain.
The effectiveness of nucleoplasty in the treatment of discogenic axial back pain is demonstrated in our results. Statistically significant improvements in VAS, ODI and SF-36 scores were seen at 6 months and 12 months. In addition, a majority of our patients achieved MCID in each of the three clinical outcome indicators as defined by us. Good to excellent results were seen in 93.33% and 73.33% patients at the end of 6 months and 12 months, respectively. Our findings contrast with those of Gerges et al. [9], who have reported that nucleoplasty may be less effective for patients with discogenic back pain without radicular symptoms.
Furthermore, a clinically significant improvement in ODI was seen in 93.30% patients at 6 months and 80% patients at 12 months. Similarly, a clinically significant improvement in SF-36 was demonstrated in 96.70% patients at 6 months and 83.30% patients at 12 months. Although all patients demonstrated some degree of improvement in the VAS score, the ratio of patients achieving a clinically significant improvement was lower for VAS score (53.30% at 6 months and 60% at 12 months) as compared to the ODI and SF-36 scores. In addition, a clinically significant mean improvement was not sufficiently demonstrated for the VAS scores in our study as per the MCID defined by us. A larger sample size may provide a more conclusive evidence of a clinically significant improvement in the VAS scores after nucleoplasty, based on the values adopted by us. Sharps and Isaac [25] defined a clinically significant improvement in the VAS scores as a reduction in the score by two points. If our study defined the MCID of VAS as 20 points instead of 30, 86.70% of patients would have achieved a clinically significant improvement in the VAS at 6 months, and 76.70% at 12 months. The mean improvement in the VAS scores would also be clinically significant at 6 months and 12 months.
We noted a slight worsening in all three clinical outcome indicators at 12 months compared to 6 months. This finding is comparable to that of the aforementioned studies [23,24]. Moreover, this slight worsening in scores was not statistically significant.
1. Role of discography, annular tear and disc height in predicting outcome after nucleoplasty
Concordant pain during provocative discography has been described by several authors as a predictor of discogenic low back pain and has been used as an inclusion criterion for nucleoplasty [24,25]. Lim et al. [26] concluded that fissured or ruptured discs and the extension of contrast into or beyond the outer annulus on the computed tomography (CT) discography were associated with concordant low back pain. Sharps and Isaac [25] recommended that concordant pain during provocative discography should be an inclusion criterion for nucleoplasty, as these patients had a significant reduction in the VAS scores after nucleoplasty. However our results showed no significant correlation between the concordant pain during discography and a clinically significant improvement in any of the three outcome indicators.
According to Bokov et al. [18], a total annulus disruption significantly influences the results of nucleoplasty. Patients with a total annulus disruption compared to those with contained disc herniation showed a significant decrease in the success rate and total pain relief. Our results, however, demonstrate that the annular integrity may not be a critical factor in determining the success of nucleoplasty, as there was no significant correlation between the annular tear and clinically significant improvement in any of the three clinical outcome indicators.
Chen et al. [14] found that the change in the intradiscal pressure after nucleoplasty was negligible in the older and degenerated discs with loss of disc height, whereas intradiscal pressure was markedly reduced in the younger and healthy discs. Based on this study and the postulated mechanism of action of nucleoplasty in the treatment of axial back pain, Mirzai et al. [19] utilized the disc height of ≥50% as an inclusion criterion for nucleoplasty. In our study, patients with a loss of disc height showed a statistically greater improvement in the ODI scores across both time points compared to patients with preserved disc heights.
A small sample size and short follow-up are the drawbacks of our study. Nevertheless, our study does offer some significant findings. By not limiting our inclusion criteria to only those discs that show pain concordance, relatively preserved disc heights and an intact annulus, we have been able to show that these factors do not influence the outcome of nucleoplasty. In other words, the benefits of nucleoplasty may be extended to a greater proportion of patients with discogenic axial back pain that fail conservative treatments.
Conclusions
Nucleoplasty produced statistically significant improvements in pain, functional disability and quality of life in patients with discogenic axial back pain after failed conservative treatments at 6 months and 12 months. Clinically significant improvements were seen in the functional disability and quality of life at both 6 months and 12 months after nucleoplasty. Good to excellent results were seen in the majority of the cases at 12 months. Concordant pain during provocative discography, presence of annular tear and loss of disc height did not influence any of the outcomes after nucleoplasty in patients with discogenic axial back pain. Nucleoplasty may benefit a larger proportion of patients with discogenic axial back pain, if the inclusion criteria are appropriately modified.