Introduction
The most common causative organism of pyogenic spondylodiscitis is Staphylococcus aureus, and it is rarely caused by Campylobacter fetus (C. fetus). Magnetic resonance imaging (MRI) is useful in diagnosis of pyogenic spondylodiscitis; however, in the initial stage of symptoms, the specific finding of high signal usually observed on a T2-weighted image is sometimes absent. We investigated the use of MRI in the early diagnosis of pyogenic spondylodiscitis caused by C. fetus and its pathology and treatment.
Case Report
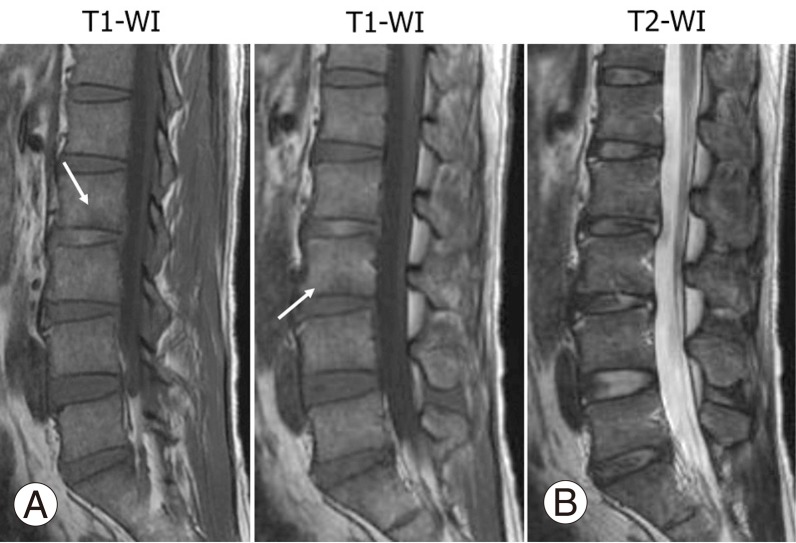
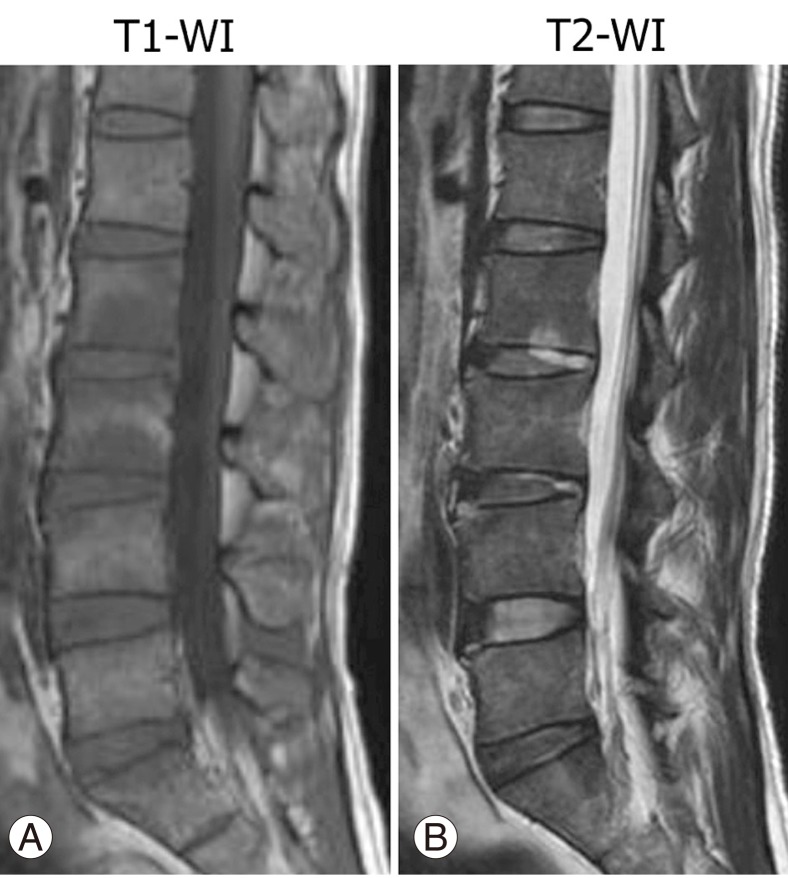
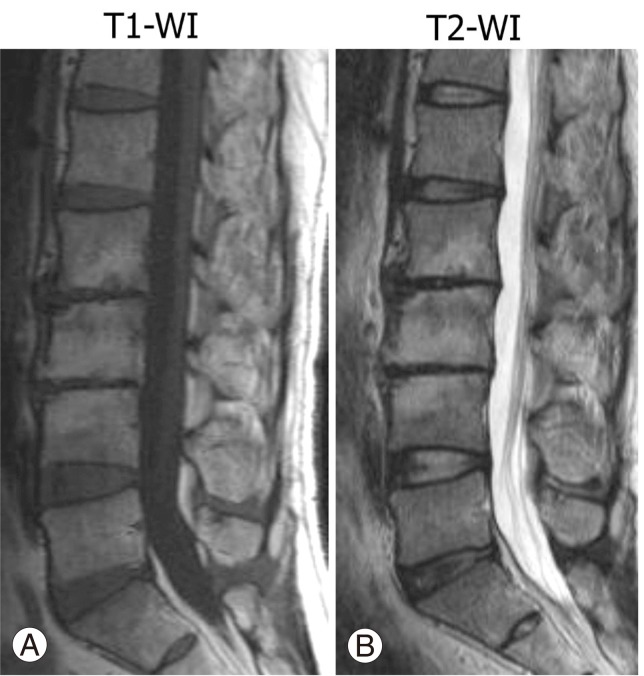
A 37-year-old male who engages in construction work (manual labor) with unremarkable medical history presented at his nearby hospital with fever (≥39℃, <40℃) that had no specific trigger nine days before the presentation. The results of a blood test were a white blood cell (WBC) count of 18,900/mm3 (<9,000/mm3) and C-reactive protein (CRP) of 0.62 mg/dl (<0.1 mg/l). He was prescribed non-steroidal anti-inflammatory drugs and oral antibiotics; however, the fever persisted and low back pain had appeared four days before the visit. Body movement became difficult, and he was hospitalized in his nearby hospital. No obvious abnormal finding was observed on lumbar MRI (Fig. 1); however, infection was suspected, and intravenous infusion of cefotiam was started. Low back pain and fever did not improve and lumbar MRI was repeated on the twenty-sixth day after onset (Fig. 2). MRI revealed abnormal signals at vertebrae and disc spaces, and blood culture at the time of hospitalization detected C. fetus. Pyogenic spondylitis was diagnosed, and the patient was moved to the internal medicine department of our hospital. Gadolinium enhancement MRI was performed by the request of our internist, and the result strongly suggested pyogenic spondylitis.
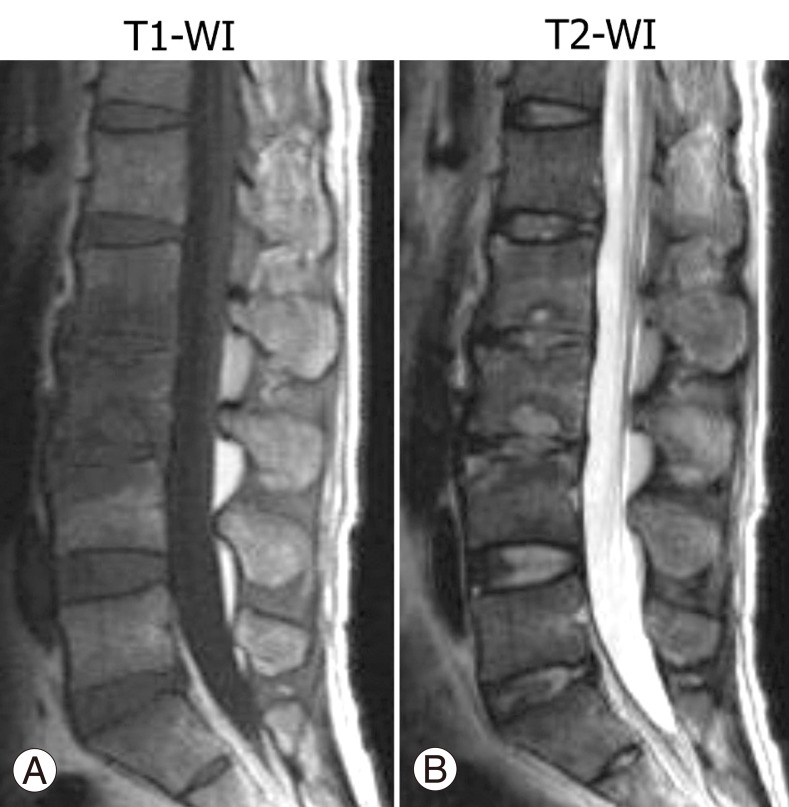
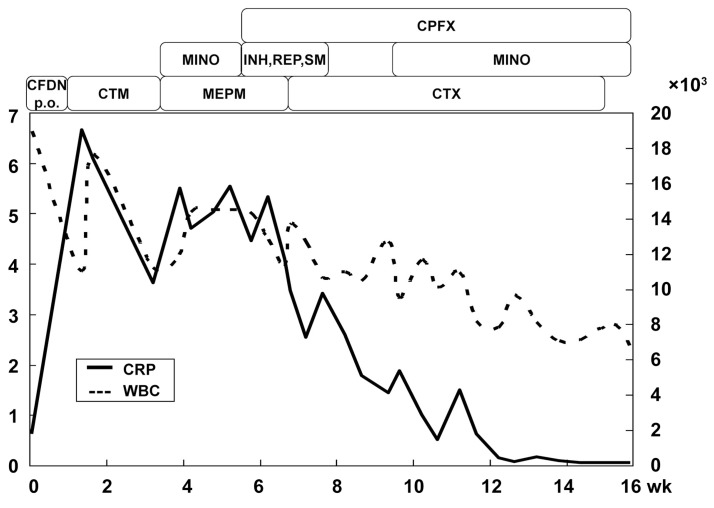
He underwent combination therapy of broad spectrum antibiotics; however, the inflammatory reaction did not mitigate after six weeks. To clarify if other causative organisms were involved in the inflammation, computed tomography (CT)-guided biopsy was performed after four days' cessation of antibiotics. Biopsy revealed negative results for tuberculosis, atypical mycobacterium, eumycetes, and cultivation of bacteria. He was transferred to our orthopaedic department at 8 weeks, and C. fetus was speculated to be the causative organism (Fig. 3). He was treated with intravenous infusion of cefotaxime, ciprofloxacin, and minocycline, and rested with a brace. At 13 weeks after the start of treatment, WBC was in the normal range. At 14 weeks, CRP was negative (Fig. 4), low back pain was improved, and MRI showed reduction of the lesion; thus, the treatment was changed to oral ciprofloxacin and minocycline and the patient discharged. He received outpatient antibiotics, choosing one or two drugs out of ciprofloxacin, minocycline, and erythromycin for 11 months. CRP temporally became negative after 14 weeks of onset, then CRP increased and became negative repeatedly. Finally, CRP was completely negative after 15 months of onset. Lesions had almost disappeared on MRI after one year, and the vertebral body showed high signal intensities on both T1- and T2-weighted images (Fig. 5). Activities of daily living were permitted without restriction after the discharge. Light work and general work was permitted after 6 and 9 months, respectively. After 13 months, back pain had almost disappeared and he performed hard labor without problems.
Discussion
The sources of C. fetus infection include intake of contaminated meat or milk and contact with infected animals, and its onset is frequently observed in immunodeficiency patients including those with diabetes, human immunodeficiency virus infection, or malignant tumor [1-3]. Such infection results in various clinical symptoms and causes various conditions, including infective endocarditis, thrombophlebitis, meningitis, meningoencephalitis, enteritis, and bacteremia, and can result in miscarriage [4]. However, the bone and joint infection rate is as low as 5% or less, and the majority of bone and joint infections occurs at the hip or knee joint [1]. As a result of our search, only 2 reports of pyogenic spondylitis caused by C. fetus were found [1,5]. The patient in the present report had no obvious contact with an infection source, and the detailed systemic work-up revealed no disease that causes immunosuppression or any infectious sites other than the spine.
Sensitivity of C. fetus to antibiotics had been studied, but optimal antibiotic treatment has not yet been established [6]. Combination therapy with doxycycline and erythromycin had been reported [1,5]; however, treatment with erythromycin is not recommended in one report due to the existence of an erythromycin-resistant strain [6]. It is important to select antibiotics considering sensitivity and tissue penetration [6]. We performed intravenous infusion of cefotaxime, ciprofloxacin, and minocycline until the inflammation reaction became negative, and then orally administered 1 or 2 drugs among the three (cycling treatment). In previous reports, oral antibiotic administration was continued 3 to 5 months after the completion of intravenous administration [1,4]. It is best to comprehensively consider all pertinent clinical and inflammation symptoms and improvement of image findings before determining whether oral antibiotics should be continued.
Some cases of pyogenic spondylitis do not present remarkable clinical findings and frequently result in delayed diagnosis. MRI is the most effective tool in early diagnosis of pyogenic spondylitis, with sensitivity and specificity as high as 96% and 92% to 94%, respectively [7]. In the acute phase, T2-weighted images present high signal intensity in the peripheral region of disc and end plate and T1-weighted images present low signal intensity in the large area of inflammation or edema around the seat of the disease [8]. However, cases without abnormal finding by MRI after 2 weeks of the onset of symptoms [9] were reported, and cautious diagnosis is required. In the case of the present report, obvious abnormal findings were not found 13 days after onset; however, pyogenic spondylitis had been suspected by clinical findings and blood biochemistry. Because the low back pain had not improved, MRI was repeated 26 days after onset. Areas of low and high signal intensity were found in the vertebral body and disc on T1- and T2-weighted images, respectively, and subsequently, pyogenic spondylitis was diagnosed. In reports of MRI images of pyogenic spondylitis, the vertebral body first presented a low signal intensity on a T1-weighted image, then a high signal intensity was observed on a T2-weighted image [10,11]. Likewise, retrospective evaluation of our case revealed that the first MRI showed slight low signal intensity of the vertebral body on a T1-weighted image (Fig. 1). However, in some cases, an MRI image within 2 weeks after onset does not reveal obvious abnormal findings, and thus repeated MRI is necessary if persistent fever or low back pain is observed. In the repeated MRI after the early MRI with no abnormal findings, careful evaluation of the T1-weighted image is important.
In addition, MRI is useful for the evaluation of disease progression and judgment of the treatment. Along with the resolution of symptoms, the low signal intensity areas on a T1-weighted image and the high signal intensity on a T2-weighted image show lesions decrease and disappear [8]. During remission, the high signal intensity sometimes appears on a T1-weighted image of the vertebral body, and it is considered to show the regeneration of fatty bone marrow [12]. In our case, lesions disappeared after 1 year, and high signal intensity was observed on a T1-weighted image.
In conclusion, we reported pyogenic spondylitis caused by C. fetus, which is rarely observed. In the diagnosis of patients who present with low back pain and fever, it is important to consider pyogenic spondylitis and to look for low signal intensity regions on T1-weighted MRI images. When the initial MRI does not reveal abnormal findings, repeated MRI after one or two weeks or, more favorably, immediate gadolinium enhancement MRI, are important for patients who have persistent low back pain and fever.