Posterior Epidural Migration of Sequestrated Cervical Disc Fragment: Case Series
Article information
Abstract
Study Design
A retrospective study was undertaken to delineate the characteristics of non-traumatic sequestrated epidurally migrated cervical disc prolapse.
Purpose
To present first case series of eight such cases diagnosed preoperatively and to discuss their magnetic resonance imaging (MRI) characteristics and their management.
Overview of Literature
Non-traumatic spontaneous migration of the sequestrated disc fragment epidurally behind cervical vertebral body is rare. Only ten cases have been reported in literature.
Methods
Detailed clinico-radiological profiles of these 8 cases are presented. In six cases their clinical picture was suggestive of cervical myelopathy. MRI scan showed single level epidural migrated disc behind body of C4, C6, and C7 in six patients and two cases with multiple levels (C5-C6). In six cases, anterior corpectomy with excision of the disc was performed and the seventh patient underwent dorsal laminectomy. The eighth patient chose not to undergo surgery.
Results
T1 images of the MRI scan showed an isointense signal in all the 8 cases. T2 images revealed a varying intensity. In six cases who underwent anterior corpectomy, there was a rent in the posterior longitudinal ligament. Among those in two cases multiple disc fragments were seen. In the rest four cases, a single large fragment was observed. These patients improved after anterior corpectomy and disc excision. There was no improvement in the patient who had undergone dorsal laminectomy. The eighth patient who refused surgery progressively deteriorated.
Conclusions
We opine that MRI scan especially T1 images are useful in these cases. We prefer to treat these cases through anterior corpectomy with excision of the sequestrated disc which proved to result in excellent outcome.
Introduction
Cervical disc prolapse is one of the common causes for neck pain and progressive quadriparesis. Herniated disc fragments are known to migrate within the spinal canal in rostral, cervical and lateral directions [1-3]. Non-traumatic posterior epidural migration of sequestrated herniated disc fragments are rare and most cases have been reported in lumbar region [4,5]. In cervical spine, these phenomenon are even more infrequent. Manabe and Tateishi [1] classified disc sequestrations in the cervical spine into four types according to their localizations. They are disc sequestrum on the anterior surface of the dural tube, lateral disc sequestrum that causes encroachment of a nerve root, lateral disc sequestrum that causes drop attack and disc sequestrum on posterior surface of dural sac [1]. Here we report a series of 8 symptomatic rare cervical disc prolapse cases. In these cases the detached disc fragment had migrated behind the middle of the vertebral body and was compressing extradurally the anterior surface of the dural tube. These sequestrated cervical discs did not lie opposite to the intervertebral disc space. Review of literature showed only 10 such anecdotal cases including 3 cases which have been diagnosed after surgery based upon the histopathology report.
There is controversy regarding the management of these cases. Few reports have suggested excision of the disc through posterior approach via laminectomy [6-9], while others opine that it can be excised by performing corpectomy [1] or microdiscectomy through adjacent disc space via anterior approach [10]. This varied opinion led us to retrospectively analyze our 396 cervical disc prolapse cases that we had treated over a period of 7 years. Our aim was to identify the typical magnetic resonance imaging (MRI) characteristics and also the optimum treatment option for these unusual cases which pose a challenging problem in decision making in spine surgery.
Materials and Methods
Between April 2003 to December 2009, 396 cervical disc prolapses were operated. Among those there were 6 cases of extruded cervical disc meeting the above mentioned criteria. These were diagnosed preoperatively using MRI scan and were operated via the anterior approach. Case 7 was operated elsewhere via dorsal laminectomy and he came to us for follow up. Case 8 of similar nature was diagnosed in the out-patient clinic and was advised surgery but she refused. The age group of the patients ranged from 35 years to 65 years and there were 5 males and 3 females. The last patient was operated more than a year ago.
All these 8 patients complained of neck pain of varying duration of 1 week to more than 2 years. All had repeated episodes of neck pain, which were managed conservatively without relief of pain. Six of these patients presented with gradual onset of difficulty in walking which worsened over a period of 6 months to 2 years. Two patients suffered neck pain only. There was no history of trauma in any of these patients. Two patients used to carry buckets of water for their house hold chores regularly for more than 10 years. They never carried them over their head. Initial clinical examination of all the eight patients revealed restriction of neck movements. Six of them had clinical evidence of bilateral pyramidal tract involvement in the form of spasticity with varying motor power between Grade 3/5 to Grade 4/5 in the upper and lower limbs. They had brisk deep tendon reflexes with bilateral plantar extensor. Varying degrees of mild sensory impairment of touch and pain below C4 and C5 with impaired posterior column sensation in both the upper and lower limbs were present. This group of patients had spastic gait with Romberg's sign being positive. There was no autonomic disturbance in any of these patients. Thus in these six cases their clinical picture was suggestive of predominantly symptomatic motor involvement than of sensory disturbance. In other two cases there was no focal sensori-motor deficit except for one patient having depressed deep tendon reflexes. Among these 8 cases, two patients had associated diabetes mellitus and hypertension. Nurick Grade of Disability was applied before and after treatment and on follow up (Table 1) [11]. Preoperative status at the time of first clinical examination showed that we had one case in Grade 0, 1, 4, and 5 and two cases each in Grade 2 and 3 (Table 1).
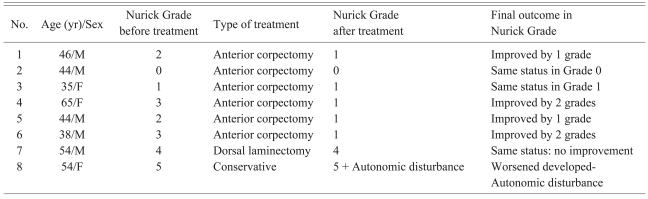
Showing the preoperative and postoperative status as evaluated using Nurick Grades of Disability with final outcome of the 8 cases treated
Radiographs of the cervical spine were taken in all these patients. MRI of the cervical spine was done using 1.5 Tesla MRI scan (Signa HDx, GE Healthcare, Waukesha, WI, USA) and sagittal T1, T2, axial gradient echo, axial T1 GRE sequence images were studied. Contrast study was not performed in any of these cases. In 6 patients, the disc had migrated behind one cervical vertebral body (C4, 2 cases; C6, 2 cases; C7, 2 cases) (Figs. 1-4). In two other patients the disc was found lying behind two vertebral bodies (C5 and C6) (Fig. 5). In all cases, T1 images revealed an isointense signal behind the body of cervical vertebra similar to the disc material in the intervertebral disc space (Figs. 1, 2, and 5). In T2 images the signal intensity varied from isointense to hyperintense (Figs. 3 and 4). In two of our cases in sagittal sections of T1 image, the disc was seen clearly as multiple fragments compressing the spinal cord (Fig. 1).

Magnetic resonance imaging T1 sagittal section showing the multiple fragments of the disc behind the body of C6 cervical vertebra appearing as isointense signal density.

Magnetic resonance imaging T2 sagittal section showing the disc behind the body of C4 cervical vertebra appearing as hyperintense signal density.

Magnetic resonance imaging T1 sagittal section showing the disc behind the body of C5 and C6 cervical vertebra seen as iso-intense signal density.

Magnetic resonance imaging T1 axial section showing the disc behind the body of C6 cervical vertebra seen as isointense signal density.

Magnetic resonance imaging T2 sagittal section showing multiple fragments of the disc behind the body of C6 vertebra seen as isointense signal density.
1. Inclusion criteria for selection of patients
Patient's preoperative MRI scan pictures should show the posterior migration of the disc material behind the body of the cervical vertebra above or below the intervertebral disc space.
The disc prolapse should cross the middle of the cervical vertebral body in the sagittal section and obliterate the anterior subarachnoid space.
Prolapsed disc should make an indentation over the anterior aspect of the cervical cord causing reduction in the cord diameter to less than 8 mm measured either in the sagittal or axial sections.
These MRI findings should also be supported by the intraoperative findings of sequestrated and migrated disc.
Only such clinically symptomatic cervical disc prolapse cases which met the above criteria were included in the study.
2. Exclusion criteria
Patients in whom the MRI scan shows the sequestrated disc fragments lying opposite to the intervertebral disc space only and compressing the thecal sac are excluded.
Patients having disc fragments that had migrated dorsal to the posterior surface of the spinal cord and intradural disc cases were excluded from the study.
Patients with cord or nerve root compression from posterior osteophytes were also not included in this study.
Prior to surgery all our hospital anesthetic protocols were followed. Among these 8 cases, 6 agreed for surgery through the anterior approach. The seventh patient after the diagnosis underwent dorsal laminectomy in a different hospital. Eighth patient refused surgery. In the first two cases through the transdiscal route, the authors tried to remove the migrated disc material using microhooks and microcurette but could not succeed in removing them completely. Hence they decided to convert it into corpectomy and observed a large residual fragment lying behind the body. The fragment was excised. On that experience, the authors decided to directly perform anterior corpectomy in the last four patients.
3. Surgical technique
General anaesthesia was given after fiber optic intubation. Flexometallic endotracheal tube was used in all cases. Throat packing was done as a routine in all cases. The patient was placed in supine position with the neck extended and rotated for 15° to the left side. Traction was not applied. The required vertebral body level was localized using image intensifier (Siemens, Erlangen, Germany). Horizontal incision was made on the right side of the neck for single level corpectomy and vertical incision for two level corpectomies. Using the standard anterior retropharyngeal approach (Smith-Robinson technique) [12] the anterior aspect of the vertebral body was exposed. Intervertebral disc space levels were reconfirmed using image intensifier. Initially, partial discectomy of the intervertebral disc spaces above and below the level of the proposed excision of the vertebral body was performed. Then Caspar retractor was applied at each disc level. Further dissection was performed under operating microscope (Zeiss, Jena, Germany). Complete microdiscectomy was done till the posterior longitudinal ligament (PLL) was clearly seen. After reapplying the Caspar retractor pins above and below the intended level of corpectomy and fully distracting the space, midline corpectomy of the respective level was performed using high speed microdrill system (Aesculap, Tuttlingen, Germany). Minimum 5 mm thickness of the lateral walls of the vertebral body was retained on either side to support the graft. The PLL was exposed along its entire length and the defect through which the disc had prolapsed was identified. The PLL was completely excised and the sequestrated disc was exposed in its entire extent both cranio-caudally and mediolaterally. All the sequestrated disc fragments were identified and their borders were clearly delineated. Each sequestrated disc fragment was initially dissected free from the anterior aspect of the dura using bayonet shaped flat tipped microdissector and ball tipped microdissector. In cases where the disc was densely adherent to the dura, gentle outward traction was given by holding the adherent disc material with 2 mm disc forceps and dissecting it free from the dura using microscissors and microdissector. The freed discs were removed using 2 mm cup tipped microdisc punches till the dura was clearly seen. Separate incision was made over the right side iliac crest and appropriate sized tricortical iliac crest graft was taken and impacted firmly in the vertebral space. Further anterior stabilization was done using anterior cervical plating and fixation using cervical spinal locking plate (CSLP or Vectra, Synthes Co., Waldenburg, Switzerland).
In four cases, single level corpectomy was performed while in two cases two level corpectomies were done and the extruded extradural cervical disc was completely excised. In six cases who underwent anterior corpectomy and disc excision, the intraoperative picture showed, under microscope, a rent in the PLL through which the disc should have migrated into the epidural space. In two cases, the discs were seen as multiple freely lying extradural fragments which corresponded with the MRI scan picture and met our criteria (Fig. 1). These were found to be densely adherent to the duramater. On further correlating the MRI scan findings of these two cases with the intraoperative findings, it was noted that in one case while intraoperative picture revealed four fragments (1 large, 3 small), MRI scan showed only 2 fragments (1 large, 1 small) (Figs. 1-3). In rest of the 4 cases, it was seen as a single large sequestrated fragment (Fig. 4). Among these in two cases there was severe indentation of the dura.
In the immediate postoperative period there was no deterioration in the neurological status in any of these patients. All the patients were discharged by the seventh day and were advised to wear hard cervical collar for a period of two months. Periodic X-rays of the cervical spine were taken on Days 1, 7, 30, and 90 in all these patients to evaluate the degree of fusion and position of the implants. The follow-up period ranged from 1 to 5 years.
Results
All the 6 patients who were subjected to anterior corpectomy and excision of the disc material improved neurologically within a span of 2 to 4 months. In 2 patients (cases 4, 6) Nurick Grade improved by two grades from 3 to 1, while in other 2 cases (cases 1, 5) there was improvement by 1 grade from 2 to 1. Case 2 and case 3 whose Nurick Grade's were 0 and 1 respectively remained in the same status (Table 1). There were no complications in any of these patients and stable fusion was achieved in all these patients by the end of 3 months (Fig. 6). All of them could carry on with their daily life without constraints and were able to return to work within a span of 3-4 months after surgery.

Postoperative X-ray showing the corpectomy graft at C5, C6 level with the implant.
The 7th patient who had undergone dorsal laminectomy in other hospital remained in Grade 4 of Nurick Disability score. His post-operative MRI scan showed persistence of the disc material (Fig. 7). Above patient, has been advised combined surgery of posterior lateral mass fixation with anterior corpectomy and discectomy of the extruded disc with anterior stabilization. Patient remains undecided regarding undergoing second surgery. The 8th patient who refused surgery progressively deteriorated over the next few months and developed autonomic disturbance in the form of bladder and bowel involvement and she remained in Grade 5 of Nurick Disability score. This patient is under observation for more than 3 years. In spite of repeated persuasion, patient was not willing to subject herself to surgical intervention. These results indicate that such type of patients should be operated and the offending disc material to be excised to achieve good outcome. Anterior cervical approach with corpectomy and stabilization is the surgical procedure of choice.

Magnetic resonance imaging sagittal section showing the disc behind the body of C6 cervical vertebra seen as isointense signal density still compressing the cord after dorsal laminectomy.
Discussion
Carvi y Nievas et al. [13] reviewed 3,000 patients with a histological diagnosis of disc herniation and found that only in 0.4% cases there was unusual migration of the disc behind the body of the vertebra. Among these 11 cases they had only one case in the cervical region where the disc had migrated posterior to the vertebral body away from the disc space [13]. Analysis of the 22 cases reported by Manabe and Tateishi [1], revealed 12 cases in the first group of disc sequestrum on the anterior surface of the dural tube. Critical review showed they had only 3 cases where the disc fragment had migrated behind the vertebral body without any connection to the disc material in the disc space, while in 7 cases it had sequestrated but was lying opposite to the intervertebral disc space, in 2 patients the particles of disc material were observed not only on the dura but also on the nerve root [1]. Medline search revealed only seven such individual cases of posterior epidural migration of sequestrated cervical disc fragments diagnosed preoperatively [1,6,8,10]. Originally in three more patients unusual sequestrated disc fragments were mistaken for another space occupying lesion and were operated. The biopsy revealed that they were disc material, thus accounting for total 10 cases reported in the entire literature by different authors [7,9,13]. The above data clearly indicate the extreme rarity of such non-traumatic extruded extradural disc in the cervical spine. Among the 396 cervical discs we treated, we had 8 typical rare cases of cervical disc prolapse which met our inclusion criteria, giving an incidence of only 2.02% indicating this is an extremely rare condition.
Clinical presentation is variable presenting only as neck pain to progressive cervical myelopathy. Clinically it is not possible to differentiate non-traumatic sequestrated epidurally migrated cervical disc prolapse (NTSEMCDP) cases from the more common cervical disc prolapse. It could be done only by carefully studying the MRI scan pictures. Detailed MRI description of such type of cervical disc prolapse cases with variation in their signal characteristics have not been reported in literature [1,2,6-10,13]. Sagittal sections especially the T1 images are extremely useful in delineating the extent of the migration of the disc material behind the body. It is seen as isointense signal similar to that of the intervertebral disc space. It also helps in identifying the number of vertebral levels involved and fragmentation of the disc material (Figs. 1 and 5). Axial sections are helpful in identifying the side and degree of compression. They may also reveal the presence of multiple fragments (Fig. 2). T1 images facilitate identification of the lesion behind the vertebral body as disc material. T2 images reveal varying signal intensity from isointense (Fig. 3) to hyperintense signal (Fig. 4) mimicking a single mass like lesion behind the body of vertebra but does not clearly show the fragmentation of the disc material. Correlating with intraoperative findings it has been observed that even though the T1 images of the MRI scan may show multiple disc material behind the body, it may not show the exact number of fragments lying behind the body as occurred in one of our cases (Figs. 1 and 2). This is likely to be due to the small fragments being mistakenly identified as the same single continuous fragment while interpreting the sagittal and axial sections and inability of the MRI scan to pick up very small fragment. MRI scan pictures also clearly differentiate these types of disc prolapses from the disc prolapse opposite to the intervertebral disc space and space occupying spinal lesions.
Management of these unusual cases is controversial. Few authors have expressed that through the dorsal laminectomy or via transdiscal route these sequestrated anteriorly compressing extradural discs behind the cervical vertebral body could be excised [6-10]. Performing only the decompressive laminectomy without removing the disc is unlikely to benefit the patient, as we have observed in our 7th case where that patient remained in Nurick Grade 4 even after dorsal laminectomy. His postoperative MRI scan performed within a year after surgery, showed persistence of the extruded disc compressing the cervical spinal cord (Fig. 7). Last two cases in our series also demonstrate that spontaneous absorption of the extruded disc behind cervical body is unlikely and the disease process worsens if not treated.
Manabe and Tateishi [1] have clearly reported that corpectomy in these group of patients is less traumatic to the cord than transdiscal route. Advantage of corpectomy is that the migrated fragments responsible for causing myelopathy are not missed behind the vertebral body and complete decompression of the thecal sac could be achieved [1]. Similar findings were reported by Raynor [14] in his study using intraoperative ultrasound for evaluating the extent of decompression for cervical microdiscectomy using the anterior approach. Our results also support the above view point. Further analysis of our surgically treated six cases did not reveal any complications due to corpectomy and anterior stabilization. With the availability of the anterior cervical plates, excellent stabilization and fusion could be achieved with iliac crest graft (Fig. 7) [15]. This is the first largest series to be reported of eight cases of non-traumatic sequestrated epidurally migrated cervical disc prolapse (NTSEMCDP) whose MRI characteristics, treatment strategies and their outcome have been outlined in detail.
Conclusions
We opine that MRI scan especially T1 images are useful in identifying non-traumatic posterior epidural migration of sequestrated cervical disc fragment cases. We prefer to treat these cases through anterior corpectomy with excision of the sequestrated disc which proved to result in excellent outcome.
Acknowledgements
We wish to acknowledge Prof. Dr. P.V.A. Mohandas-Chief MIOT Hospitals, Chennai for permitting us to do the work. Dr. S. Ponraj, Senior Consultant Neurosurgeon MIOT hospitals for critically reviewing this manuscript.