Introduction
With the increasing geriatric population, there has been a rise in the incidence of spinal diseases. Of the many spinal anatomical parameters, an understanding of the spinopelvic alignment has become important [1-4]. According to Gelb et al.'s study [5] of 100 adult normal volunteers aged over 40 years, an increasing age correlated with a more forward sagittal vertical axis with a loss of distal lumbar lordosis, and no increase in thoracic or thoracolumbar kyphosis. However, their study had only a small cohort of 36 men more than 50 years of age. Hammerberg and Wood [6] examined 50 subjects with an average age of 76 years (range, 70 to 85 years), and reported that the anterior positioning of C7 was positively correlated with age and decreasing lordosis with age above 70. Although many studies have described spinal anatomical alignment in older age groups [5,7-12], to the authors' knowledge, there are few reports describing the changes in the detailed segmental sagittal parameters in subjects more than 50 years of age.
This study evaluated prospectively the sagittal standing radiographs of the whole spine including the pelvis in 132 Korean adult male volunteers aged over 50 years. These parameters in the 6th, 7th and 8th decade groups were compared and any age-related variations were examined.
Materials and Methods
The study was performed prospectively from March 2007 to June 2009 after gaining Institutional Review Board approval. Only male volunteers were examined because our hospitals deal mainly with male subjects. The subjects had no history of trauma, spinal disease, history of spinal surgery or pain in the spine and lower extremity in two hospitals. The radiographic measurements were obtained in accordance with published techniques on standing radiographs [13,14]. They were taken on 36 inch film, in the position of hip and knee joint extension with both hands on the clavicle. Subjects with more than 10° of scoliosis or spina bifida in the coronal view; spondylolisthesis, monosegment intervertebral disc space narrowing, monosegment wedge-shaped vertebral body in sagittal view, and subjects with a history of thoracoabdominal surgery were excluded.
The total number of subjects was 132. The subjects were divided into 3 groups according to age. Group 1 was composed of 45 volunteers in their sixth decade (range, 53 to 60 years). Group 2 contained 65 volunteers in their seventh decade (range, 61 to 68 years). Group 3 comprised of 22 volunteers in their eighth decade (range, 71 to 83 years).
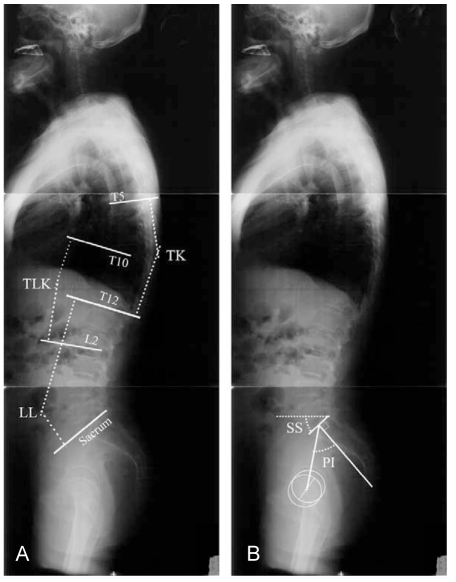
For the radiological parameters, the horizontal perpendicular distance from the posterosuperior endplate of the sacrum to the plumb line of C7 was measured as a global sagittal balance. The positive or negative values meant forward or backward translation in reference to the posterosuperior endplate of the sacurm. The angular parameters were thoracic kyphosis (T5 upper end plate [UEP]-T12 lower end plate [LEP]), thoracolumbar kyphosis (T10 UEP-L2 LEP), total lumbar lordosis (T12 LEP-S1 UEP) and lower lumbar lordosis (L4 UEP-S1 UEP). The sacral slope and pelvic incidence were measured for the pelvic parameters. The sacral slope was defined as the angle between the superior plate of S1 and a horizontal line. The vertical and horizontal sacrum is described by a low and high value, respectively. The pelvic incidence was defined as the angle between a line perpendicular to the endplate of sacrum at its midpoint and a line connecting this point to the axis of the femoral head (Fig. 1).
Statistical analysis was performed using ANOVA to assess the difference in the continuous measures between the three groups. Distribution of the variables is reported as the mean, range, and standard deviation (±). A p-value < 0.05 was considered significant. The bivariate correlation between the variables was examined using the Pearson correlation coefficient. p-values < 0.05 and < 0.01 were considered significant. Simple linear regression was used to test for significant correlations between these measurements and age. The data was analyzed using SPSS ver. 10.1 k (SPSS Inc., Chicago, IL, USA).
Results
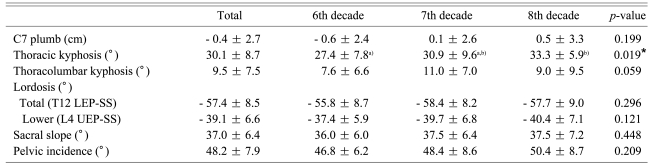
The average height, weight and body mass index was 1.67 ± 0.056 m, 67.0 ± 9.9 kg and 24.0 ± 3.1, respectively. There was no significant difference between the 3 groups (Table 1).
The average horizontal perpendicular distance from the posterosuperior endplate of the sacrum to the plumb line of C7 was - 0.4 cm (range, - 7.2 to 9.6 cm, ± 2.7 cm). The difference between the three groups was not significant (Table 2).
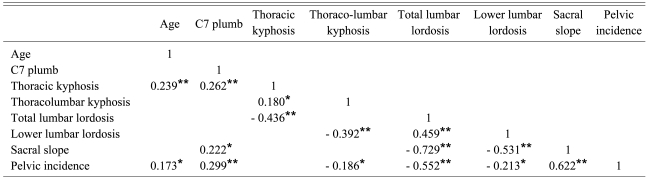
In the sagittal angular parameters, the average thoracic kyphosis (T5 UEP-T12 LEP) was 30.1° (range, 8.0 to 54.0°, ± 8.7°): 27.4° (range, 8.0 to 43.0°, ± 7.8°), 30.9° (range, 9.0 to 54.0°, ± 9.6°) and 33.3° (range, 22.0 to 46.0°, ± 5.9°) in groups 1, 2 and 3, respectively, with a significant difference between the three groups (p = 0.019). Thoracic kyphosis showed a correlation with age (r = 0.239, p < 0.01). The average thoracolumbar kyphosis (T10 UEP-L2 LEP) was 9.5° (range, - 12.0 to 33.0°, ± 7.5°) with no significant difference between the three groups (p = 0.059).
The average total lumbar lordosis (T12 LEP-S1 UEP) and average lower lumbar lordosis (L4 UEP-S1 UEP) was - 57.4° (range, - 80.0 to - 28.0°, ± 8.5°) and - 39.1° (range, - 58.0 to - 23.0°, ± 6.6°), respectively. There was no significant difference between the three groups except for thoracic kyphosis (Table 2).
With regard to the pelvic parameters, the mean sacral slope and the mean pelvic incidence was 37.0° (range, 21.0 to 51.0°, ± 6.4°) and 48.2° (range, 29.0 to 71.0°, ± 7.9°), respectively. There was no significant difference in the sacral slope (p = 0.448) and pelvic incidence (p = 0.209) between the three groups (Table 2).
Strong correlations were observed between the total lumbar lordosis and sacral slope (r = - 0.729, p < 0.01), as well as between the sacral slope and pelvic incidence (r = 0.622, p < 0.01). There were moderate correlations between the total lumbar lordosis and thoracic kyphosis (r = - 0.436, p < 0.01), lower lumbar lordosis (r = 0.459, p < 0.01) and pelvic incidence (r = - 0.552, p < 0.01). Lower lumbar lordosis also showed a moderate correlation with the sacral slope (r = - 0.531, p < 0.01) (Table 3).
Discussion
The incidence of reconstructive spinal surgery is increasing with the rising geriatric population. Some authors asserted that surgical planning should accommodate the anticipated age-related changes in sagittal alignment [5,15]. Therefore, it is important to document age-related sagittal contour changes that occur in a normal aging spine.
The normal indices for segmental spinal angulations have been described previously for pediatrics, adolescents, and somewhat older populations in an effort to characterize some of the natural changes that occur with advancing age [5,7-12]. However, there have been few studies focusing on subjects older than 50 years. Kobayashi et al. [16] performed a 10-year longitudinal study of 100 adult healthy volunteers aged over 50 years, and reported that not all subjects had normal values at the final follow-up. However, their study was limited in that it only showed potential natural courses in normal spines, but did not analyze the characteristics of a normal spine in the time of the study. Hammerberg and Wood [6] examined the cross sectional sagittal spinal alignment in asymptomatic adult volunteers with a relatively narrow age range from 70 to 85 years only. This had the tendency to skew the results against those of the general elderly population. However, there are no reports focusing on subjects 50 years and older, which is the age group in which the majority of degenerative spinal surgery procedures are performed. The ages of our volunteers ranged from 53 to 83, and to the best of our knowledge, this is the first sagittal alignment study of normal subjects from the beginning of old age with the same ethnic background. In addition, the confounding factors of postmenopausal osteoporosis were removed by excluding female subjects.
The horizontal perpendicular distance from the posterosuperior endplate of the sacrum to the plumb line of C7 was measured as a global sagittal balance, and several authors reported that it correlated with the other parameters [5,6,9,11]. Gelb et al. [5] showed that older-aged participants tended to have a sagittal vertical axis or C7 plumb line that fell further forward but the correlation was relatively mild (r = 0.255, 0.01 < p ≤ 0.025). Vedantam et al. [11] reported that adolescents had a significantly more negative sagittal vertical axis than adults. Hammerberg and Wood [6] stated that the anterior positioning of C7 was positively correlated with age and decreasing lordosis after age 70. In this study, the mean C7 values appeared different, but there was no significant difference between the 3 groups (p = 0.199).
With regard to thoracic kyphosis, Gelb et al. [5] reported no correlation between age and kyphosis in the thoracic spine or thoracolumbar junction. However Bartynski et al. [17], in a lateral chest X-ray study, showed that the thoracic kyphotic angle increases with age. They mentioned that the posterior thoracic spines are protected by rib articulation leading to increasing kyphosis with age. Korovessis et al. [10], in his full length sagittal spinal standing radiographic study, demonstrated that thoracic kyphosis increases with age. These results demonstrated significant differences between the 3 groups (p = 0.019), and that thoracic kyphosis increases with age. Thoracic kyphosis also showed a correlation with age (r = 0.239, p < 0.01), which in our opinion is the key change in sagittal alignment in those older than 50 years.
Thoracolumbar kyphosis was believed to be straight and Vedantam et al. [11] showed that the thoracolubar kyphosis gathered from asymptomatic adolescents was 1 ± 9°, which is in contrast to compared to Jackson and Hales [18], who reported 6.3 ± 7.9° for healthy subjects aged 20-63. In the present study, the thoracolubar kyphosis was 7.6 ± 6.6°, and 9.0 ± 9.5° in the 6th and 8th decades, respectively, showing some increase with age (p = 0.59).
With regard to lumbar lordosis, there are several different opinions. Vedantam et al. [11] were unable to show a significant difference between adolescents and adults. However, Gelb et al. [5], in their study of adults aged over 40 years, reported a significant correlation between increasing age and decreasing lumbar lordosis. After the seventh decade, Korovessis et al. [10] reported that lumbar lordosis decreases dramatically, and Kobayashi et al. [16] stated that lumbar lordosis decreases with age. On the other hand, Hammerberg and Wood [6] could not establish an association between the overall lordosis and advancing age. These results showed no significant differences between the 3 groups. The lower lumbar lordosis is very important in determining the total lordosis [19]. Gelb et al. [5] reported that increasing age correlated with a more forward sagittal vertical axis with a loss of distal lumbar lordosis. In our data, lower lumbar lordosis did not decrease with age.
Regarding the pelvic parameters, Korovessis et al. [10] did not demonstrate a change in the sacral slope with age. In the present study, the sacral slope did not decrease with age. Legaye et al. [20] reported that the pelvic incidence is a fixed parameter that characterizes an individual's anatomy, and does not change with time. In the current study, the pelvic incidences were not different in the 3 groups.
There were some limitations in this study. First, it was presumed that all individuals in their respective groups had similar sagittal patterns. Although some authors [21,22] have suggested several sagittal patterns in normal subjects, that type of subclassification was beyond the scope of this study. Second, we could not demonstrate a relationship between the change in the shape of the intervertebral disc and bony remodeling of the vertebrae, which will contribute to the resulting spinal alignment. Bone mineral density measurements were not performed, and neither could the compounding factors, such as osteoporosis, be removed. However compared to previous studies, this study recruited a large number of subjects with strict criteria and homogenous characteristics. These results not only substantiate and expand existing age-related alignment changes but also demonstrate some differences with other studies.