Introduction
Of all the diseases that are diagnosed and treated at out patient departments, lower back pain is the second most prevalent and it has a great effect on increasing medical expenses every year [1-3]. The lumbar facet joints of the lumbar spine are one of the major causes of chronic lower back pain and it may causes lumbar spine pain. It may also cause referred pain [4-6]. The primary treatments for lower back pain commonly include bed rest, medication and physical therapy. Despite these treatments, there are many cases in which the chronic disease progresses without improvement of the symptoms [7]. Spinal facet block has been performed as one of the methods of conservative treatments in these patients. This has also been reported to be a valuable modality for the treatment of multiple pathologic lesions or for determination of surgical sites [8]. Spinal facet block has generally been performed under fluoroscopy or computed tomography (CT) guidence. Side effects have been reported to occur in the eye, genital system and skin following this frequently performed procedure and due to the increased radiation exposure [9]. In recent years, the application of ultrasonography has increased to diagnose and treat the musculo-skeletal system [10,11]. Yet in the field of vertebral surgery, the application of ultrasonography has been limited in scope. Any medical literature about the use of ultrasonography when performing spinal facet block is scarce at best. At our department, spinal facet block has been performed using a fluoroscopy-guided method since 1992 in the patients who complained of low back pain. Since January of 2008, ultrasonography-guided spinal facet block has been concomitantly performed. Given this background, we compared the treatment outcomes between the two treatment modalities and we examined the usefulness and future significance of ultrasonography-guided spinal facet block.
Materials and Methods
1. Materials
During a period ranging from January to June of 2008, of the patients who visited the out patient Department of Orthopaedic Surgery with a chief complain of low back pain and referred pain and then they received a diagnosis of spinal stenosis based on findings such as central spinal stenosis or postero-lateral spinal stenosis with a more than one segment seen on their medical history, physical examination, the magnetic resonance imaging (MRI), CT and simple radiography, 133 patients showed no satisfactory improvement of symptoms following medication, physical therapy and exercise therapy for more than three months. Of them, 105 patients who could be followed up for more than six months received prospective assessement for this study. The method for guiding the spinal facet block was randomily selected. There were 26 men and 25 women in the radiation group (group 1). The mean age of this group was 56.1 years (range, 45 to 79 years). There were 21 men and 33 women in the ultrasonography group, and the mean age was 58.3 years (range, 47 to 83 years). The mean follow-up period was 9.1 months (range, 6 to 14 months) in group 1 and 8.9 months (range, 6 to 15 months) in group 2. The selection of groups 1 and 2 was done based on the randomization principle. There were no statistically significant differences in the age, gender, the preoperative visual analogue scale (VAS) score and the Oswestry disability index (ODI) between the two groups. The mean surgical time, medical expenses and complications were evaluated for both groups. The VAS score and ODI were evaluated preoperatively and at the last follow up through physical examinations and interviews.
2. Methods
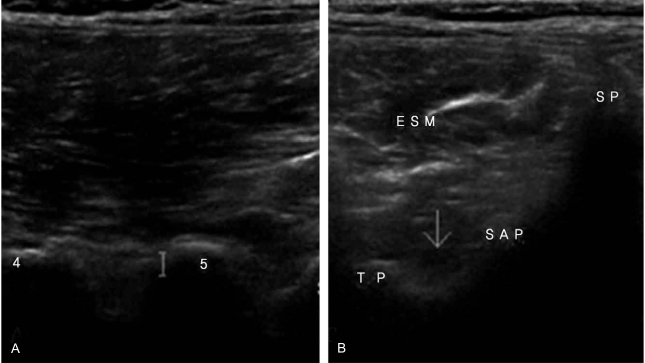
Prior to spinal facet block, an interview was performed for obtaining the past medical history. The location of the pathologic lesion and the severity of pain were evaluated by physical examinations. The spinal segments containing the pathologic lesion were determined using simple radiography, computed tomography CT and MRI scans. One segment per one-time surgery was the employed principle. The procedure was performed for the bilateral facet joints of one segment that was considered to be a cause of the pain. This was restricted to being done once a day and once for one patient. Both the ultrasonography-guided method and the fluoroscopy-guided method were performed by a single orthopaedic doctor. Spinal facet block that was performed using ultrasonography was done via a posterior approach. The patients were laid on the table in the prone position, and high-resolution ultrasonography (Aloka α5SV 60-Hz) and a linear probe were used. The posterior paraspinal sagittal image was obtained to discriminate the vertebral location (Fig. 1A). Using a linear probe, the spinous process was confirmed by employing the axial transverse image. Inferior displacement was then attempted, and meanwhile, the lamina was confirmed. The displacement was also attempted to the lateral side of the inferior border of the lamina, the lateral side and the inferior side. Thus, the facet joint was confirmed (Fig. 1B). Local anesthesia was performed on the lateral side of the linear probe. Using the axial transverse image, a 22-gauge spinal needle was inserted up to a level of the facet joint. When the spinal needle is inserted, it should be parallel with the linear probe and then forwarded towards the facet joint. When the spinal needle reached the facet joint on the ultrasonography image, dexamethasone and 2% lidocaine were mixed at a volume of 0.5 ml. This mixture was then injected to the facet joint using a spinal needle.
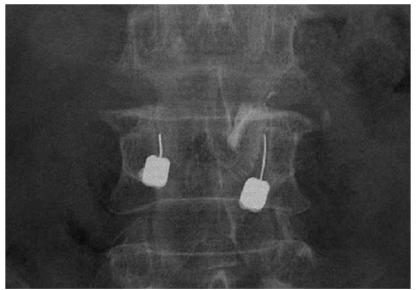
For the cases in which fluoroscopy was used, patients were laid on the table in a prone position. The location of the facet joint was confirmed under fluoroscopic guidance. Then, a 22-gauge spinal needle was inserted and this was forwarded to the facet joint. When reaching the facet joint, 0.3-ml of contrast media was infused. It was confirmed that the spinal needle was located in the facet joint capsule (Fig. 2).
Dexamethasone and 2% lidocaine were mixed at a volume of 0.5 ml, and the mixture was injected to the facet joint through a spinal needle. The locations at which the spinal facet block was performed included the L4/5 facet joint in the ultrasonography group, where it was performed 28 times and this was the most prevalent location of treatment. This was followed by L3/4 (15 times), L5/S1 (8 times) and L2/3 (3 times). In the radiation group, spinal facet block was performed 29 times for the L4/5 facet joint and this was the most prevalent location of treatment. This was followed by L3/4 (12 times), L5/S1 (8 times) and L2/3 (2 times). In both the ultrasonography group and the radiation group, spinal facet block was most frequently performed for L4/5 (Table 1).
3. The methods for interpreting the results
Following spinal facet block, the patient received approximately 30-minutes of bed rest and any abnormality was confirmed at an injection room. Following the procedure, regular follow-up was performed at the outpatient clinic on week 2, month 1, month 3 and month 6. The degree of pain improvement and the changes in the ambulation function were assessed through an interview with the patients and those changes of the findings on the physical examinations were recorded. The degree of the change of symptoms was measured using the ODI and the VAS score.
Results
1. Surgical times in the ultrasonography group and the radiation group
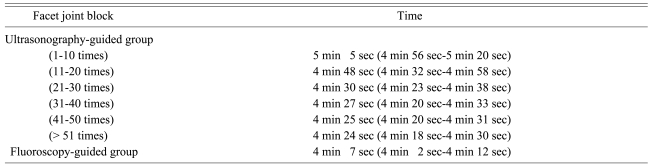
The surgical time for performing spinal facet block was defined as the time point at which the radiological images were obtained using fluoroscopy in group 1 and extending to that time at which injection of the drugs in the spinal needle was completed. The mean surgical time was 4 minutes and 7 seconds. In the group 2, the surgical time for performing spinal facet block was defined as the time point at which the ultrasonographic image was obtained using a probe and extending to that time at which the injection of drugs in the spinal needle was completed.
The mean surgical time for the patients in the range between 1 and 10 minutes was 5 minutes and 5 seconds. The mean surgical time for the patients with a range between 11 and 20 was 4 minutes and 48 seconds. The mean surgical time for the patients with a range between 21 and 30 was 4 minutes and 30 seconds. The mean surgical time for the patients with a range between 31 and 40 was 4 minutes and 27 seconds. The mean surgical time for the patients with a range between 41 and 50 was 4 minutes and 25 seconds. The mean surgical time for the patients with a range gerater than 50 was 4 minutes and 24 seconds. These results indicate that the degree of the reduced surgical time was not great and the difference in the surgical time from the radiation group was < 20 seconds (Table 2).
2. Assessment of the improvement of symptoms following the treatment
In the group 2, the mean ODI was significantly improved from 32.3 (range, 28 to 41) preoperatively to 23.5 (range, 17 to 26) at a final follow-up. In group 1, the mean ODI was improved from 34.2 (range, 29 to 43) preoperatively to 24.8 (range, 18 to 28) at the final follow-up (Table 3). In group 2, the mean VAS score was significantly improved from 7.5 points (range, 5 to 9 points) preoperatively to 2.8 points (range, 1 to 4 points) at the final follow-up (Table 4). The number of cases in which the pain control was shown to be < 3 points was 12. The number of cases in which the pain control was shown to be > 3 points was 42. In group 1, the VAS score was significantly improved from 7.8 points (range, 4 to 10 points) preoperatively to 2.7 points (range, 1 to 4 points) at the final follow-up (p < 0.05). The number of cases in which the pain control was shown to be < 3 points was 14. In 37 cases, the pain control was shown to be > 3 points. These results indicate that the symptoms were improved following the block procedure in both group 1 and group 2 (Table 4).
3. Complications following the block procedure
As for the complications, there were some cases in which the aggravation of low back pain, a tingling sensation, headache, chest pain and allergic reaction occurred. These occurrences were seen in four cases of group 2 and three cases of the group 1. For group 2, there was one case of superficial infection. There was another case of lower motor weakness. There were no statistically significant differences in the incidence of complications between the two groups. The superficial infection was improved within several days. The lower motor weakness was improved within one day. Excluding this, the complications were improved within several hours.
The difference in the medical expenses between the ultrasonography group and the radiation group.
In group 2, the fee was approximately KRW 38,000 with including the fees for the medical treatments and the use of ultrasonography. In group 1, this was approximately KRW 25,000 with including the fees for medical treatments and the use of ultrasonography. These results indicate that the difference in the medical expenses between the ultrasonography group and the radiation group was KRW 13,000.
Discussion
In 1911, Goldthwait [5] reported the possibility of the spinal facet joint being a cause of sciatica. The term "facet joint syndrome" has been used since the 1930s. Overload of the posterior lumbar joint, muscle imbalance and degenerative change are all associated with lumbar facet joint syndrome [12,13]. In 1941, Badgley [14] reported that the posterior joint was the cause of chronic lower back pain. According to Shealy [15], facet joint lesion was present in 82% of the patients with chronic lower back pain. Bed rest, medication and physical therapy are performed for the treatment of posterior joint-related lumbar pain. In association with this, in the patients who showed no symptomatic improvement, such invasive therapy as as open denervation [6], radio-frequency denervation [16], cryo-denervation [17] and the local injection of various drugs have been performed. Injection therapy was converted to various methods and then this performed during a long period. In 1976, Mooney and Robertson [18] first performed intra-articular injection of steroid and local anesthetics. Since then, many studies have been conducted to examine spinal facet block [19]. The previous studies have focused on the role of intra-facet joint injection as the diagnostic tool. Yet among many of the patients who received injection, the pain that was lost appeared again. According to these studies, following the injection therapy using local anesthetics, improvement of symptoms was seen in approximately 43% of the patients at follow-up that was conducted after 7.9 months. This procedure is performed under CT or fluoroscopic guidence. The block that is performed under CT or fluoroscopic guidance enhances the accuracy and success rate, but there are disadvantages such as the exposure to radiation, the large-sized equipment and the high cost as compared with ultrasonography [5,20,21]. In 1965, Pack and Davis [22] reported on cases of skin cancer due to irradiation. In Korea, Lee et al. [9] reported on a hand lesion that was damaged due to irradiation. According to Wilson [23], it is worrisome that the hand region of orthopedic surgeons who use the irradiator could be excessively damaged by the irradiation. The use of ultrasonography has recently been increasing in the field of orthopedic surgery. Musculo-skeletal ultrasonography was first introduced by Seltzer [24] in 1979, and this is a non-invasive diagnostic test. It causes no pain, which is also advantageous for dynamically assessing the interesting sites on the spot and on a real-time basis in a cost-effective manner. There are advantages such as the smaller-sized equipment, the avoidance of radiation exposure and the safety for pregnant patients. It has been used instead of radiography for the diagnosis and treatment of musculo-skeletal disorders. In recent years, it has frequently used for the diagnosis of preoperative rotator cuff tear, tendon rupture or soft tissue masses. The following matters should also be considered:
Ultrasonography has an important role in peripheral nerve block. Greher et al. [10,11] reported on the clinical usefulness of medial branch block of the spinal nerves using ultrasonography. Those authors performed spinal facet block under ultrasonographic guidance in five patients and five cadavers 28 times and 50 times, respectively. Both groups showed the excellent treatment outcomes. But the quality of the ultrasonographic images can show a difference depending on the technical expertise of the surgeons. Due to the insufficient specialized knowledge about radiology and the difficulty in accurately interpreting the anatomical structures with using 2-dimensional ultrasonography, there may be difficulty when using it. In the current study, the operator who used ultrasonography was an orthopedic surgeon who had more than 300 cases of experience with spinal block under fluoroscopic guidance. This surgeon examined the spinal structures in 30 normal healthy people prior to the ultrasonographically guided procedures. Following the procedure using ultrasonography, the difference between the surgical time in the early stage of the procedure (before 40 times) and that after 40 times was approximately 40 seconds. Based on these results, it can be inferred that spinal facet block under ultrasonographic guidance can be simply performed in an outpatient setting with a certain degree of experience and training. Yet in the current study, no evaluation was performed to examine the accuracy of spinal facet block between experienced surgeons and non-experienced ones. In regard to the accuracy of spinal block, no confirmation was performed using radiological images. Further studies are therefore warranted to compare the accuracy between the ultrasonography and spinal block. Also, in obese patients, there was a great gap between the skin and the facet joint. There is a limitation that a high-quality ultrasonographic image can not always be obtained. Also in ultra-lower-weight patients, the ultrasonographic probe cannot be closely contacted to the skin. This poses a difficulty in obtaining a high-quality image. Accordingly, in all the patients, there is difficulty to perform this procedure using ultrasonography. Due to the limitation of the range of the ultrasonographic images, it is not easy to perform nerve root block. Of the side effects that occurred following the procedure, the aggravation of lower back pain might have originated from penetrating the facet joint capsule and capsular distension due to injecting the drug in the intracapsular space. The corresponding cases mainly complained of a compressive sensation rather than pain. The tingling sensation might be caused by a nerve root due to the leakage of local anesthetics. The chest pain and headache might have originated from the side effects due to steroids. A weakness of the muscle strength in both extremities might have originated from the drug injection in the epidural space because of incorrectly locating the spinal needle in the epidural space. As a result, real-time ultrasonographic guidance could be performed without difficultly with a certain amount of training. This could produce improvement of the clinical symptoms. Spinal facet block under ultrasonographic guidance can be a useful tool for a generally invasive procedure that is performed to treat the pain associated with the vertebral spines. If the accuracy of ultrasonographic guidance can be gradually enhanced, then this modality can be used as a subsitute for irradiators and CT.
Conclusions
The surgical time for spinal facet block using ultrasonography and the irradiator showed that there was a less than a 30-second difference following a certain degree of the training.
All the spinal blocks performed through both guidance methods were effective for pain control. There was no significant difference in the incidence of complications between the guidance methods.
The medical expense following spinal facet block was relatively higher in the ultrasonography group.
Based on the above results, spinal facet block under the ultrasonographic guidance is expensive, as compared with that via irradiation, and it is also disadvantageous by producing additional complications such as superficial infection. Even in the absence of radiation exposure, it can be performed during in a short-term period following a certain degree of the training at an outpatient setting. There were also satisfactory treatment outcomes that showed no significant difference in the degree of pain control. Therefore, this might be alternative modality to irradiation when performing spinal block.