A New Radiological Sign for Severe Angular Kyphosis: “The Baltalimani Sign”
Article information
Abstract
Study Design
Retrospective diagnostic study.
Purpose
To define a new radiological sign, “Baltalimani sign,” in severe angular kyphosis (SAK) and to report its relationship with the risk of neurological deficits and deformity severity.
Overview of Literature
Baltalimani sign was previously undefined in the literature.
Methods
We propose Baltalimani sign as the axial orientation of the vertebrae that are located above or below the apex of angular kyphosis on anteroposterior radiographs. Patients with SAK of various etiologies with kyphotic angles ≥90° were selected and evaluated for the presence of Baltalimani sign. Demographic data of the patients including age, gender, etiology, neurological status, local kyphosis angles, and the location of the kyphosis apex were recorded. Sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) of Baltalimani sign for the risk of the neurological deficits were evaluated by the IBM SPSS ver. 20.0. A p-values of <0.05 were considered statistically significant. Cohen's kappa was used for analysis of interrater agreement.
Results
The mean local kyphosis angle in all patients was 124.2° (range, 90°–169°), and 15 of 40 (37.5%) patients had neurological deficits. Baltalimani sign was seen in 13 of 15 patients with neurological deficits (p=0.001). Baltalimani sign showed a sensitivity and specificity PPV and NPV of 61.9%, 86.7%, 89.5%, and 68.8% for the risk of the neurological deficits in SAK patients, respectively. Cohen's kappa value was moderate (κ=0.506).
Conclusions
The detection of Baltalimani sign in SAK may indicate severity of deformity and the risk of neurological deficits.
Introduction
Angular kyphosis is a localized spinal deformity with a sharp angulation. It is observed in patients with congenital kyphosis, kyphosis associated with spina bifida, post-tuberculosis kyphotic deformity, and kyphosis associated with skeletal dysplasia (type 1 neurofibromatosis, Morquio syndrome or achondroplasia) [1]. Particularly severe angular kyphoses may cause paraparesis or paraplegia [1234567891011]. In addition to cosmetic problems, many patients have back pain, buttock pain, and functional disability caused by the spinal imbalance associated with severe angular kyphosis (SAK). The development of neurological deficit risk in angular kyphosis patients may be related to age, etiology, congenital pathology type, involved level, and the severity of sharp local kyphosis. Accordingly, some of these defined radiographic criteria are detected in the sagittal views [1213]. However, the evaluation of anteroposterior radiographs is as important as the that of lateral radiographs. The purpose of this retrospective diagnostic study was to define a new radiographic sign (detected in the anteroposterior radiographs) and to demonstrate its association with the severity of deformity and clinical findings (neurological deficits) in SAK patients.
Materials and Methods
In SAK, the vertebrae located immediately above or below the apex of angular kyphosis are positioned vertically or nearly vertically. In anteroposterior radiographs, they can be observed as vertebrae normally appear in axial views superimposed on the adjacent vertebrae. This new radiographic appearance is defined as “the Baltalimani sign” by the authors of this study (Figs. 1, 2, 3, 4). We used the term Baltalimani because it is the name of our center and the name of the district where our center is located. The anteroposterior and lateral standing radiographs the spine of 4,566 patients admitted to our clinic with various complaints between years 2012 and 2014 were evaluated retrospectively. Low-quality radiographs from previous years were intentionally excluded.

Schematic drawing of “Baltalimani sign”. Baltalimani sign is the axial orientation of the vertebrae located above or below the apex of angular kyphosis in the anteroposterior view.

(A, B) Anteroposterior and lateral standing view of an sample case of post-tuberculosis severe angular kyphosis. Note the marked axial orientation of the lumbar vertebra (asterisk) on the anteroposterior radiograph. We have named this “Baltalimani sign”.

(A, B) Baltalimani sign on an anteroposterior radiograph (asterisk) and a lateral radiograph in a case of post-tuberculosis severe angular kyphosis.

(A, B) Baltalimani sign on the anteroposterior radiograph (asterisk) and lateral radiograph in congenital severe angular kyphosis.
The radiographs were obtained with 30×90-cm radio-graphic films using the same X-ray tube with a film distance of 150 cm. For the standing anteroposterior and lateral radiographs, the patients were placed in a comfortable standing position, with the hips and knees fully extended. For all subjects, the elbows were fully flexed and the fists were resting on the clavicles. We initially evaluated anteroposterior radiographs and identified of 40 patients with SAK with various etiologies but with kyphotic angles ≥90° were included in the study because Baltalimani sign can be only observed in such cases. The study did not determine the association between kyphotic angle and neurological deficits risk. For this reason, we did not include all of the angular kyphosis cases. We included only SAK because Baltalimani sign is not seen in kyphosis with <90° kyphotic angle. Among these 40 patients, 21 patients with were positive for Baltalimani sign; the remaining 19 patients were negative for it. Clinical records were reviewed for demographic data, etiology of the lesion, and Frankel grades of neurological status. Lower-extremity motor and sensorineural status, deep tendon reflexes, and pathological reflexes were assessed on examination, and patients neurological deficits were recorded according to the Frankel grading system. The criteria for the neurological deficits used in statistical analysis was assigned according to Frankel A, B, C, and D grades. The patients were then subgrouped according to SAK etiology. Flexibility was assessed using hyperextension lateral radiographs for SAK. Cobb angles and local kyphosis measurements were made using by DICOM medical imaging software (Nemaris Inc., New York, NY, USA) [14].
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of Baltalimani sign for the risk of the neurological deficits were evaluated by the IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA). A p-values of <0.05 were considered statistically significant. Cohen's kappa was used for analysis of interrater agreement.
Results
Of the 40 SAK patients with kyphotic angles ≥90°, 14 were male (34%) and 26 were female (65%). Demographic characteristics can be seen in Table 1. Neurological deficits were detected in 15 of 40 (37.5%) patients. Baltalimani sign was seen in 13 of 15 (86.7%) patients with neurological deficits. According to the Frankel grading system the neurological status was Frankel E in 25 patients (62.5%), Frankel D in 12 (30.0%), and Frankel C in 3 (7.5%). Among the 13 patients with positive Baltalimani sign (Baltalimani [+]), the etiology of neurological deficits was post-tuberculosis kyphosis in five patients (38.4%), neurofibromatosis in four (30.8%), and congenital kyphosis in four (30.8%). In these patients, the levels of the apex of kyphosis was T4 in one patient, T7 in two, T8 in one, T9 in three, T10 in one, T11 in one, and T12 in four. The etiology in the two patients with neurological deficits but with a negative Baltalimani sign (Baltalimani [–]) was post-tuberculosis kyphosis. The apical vertebrae of the deformity in these patients were T4 and T5.
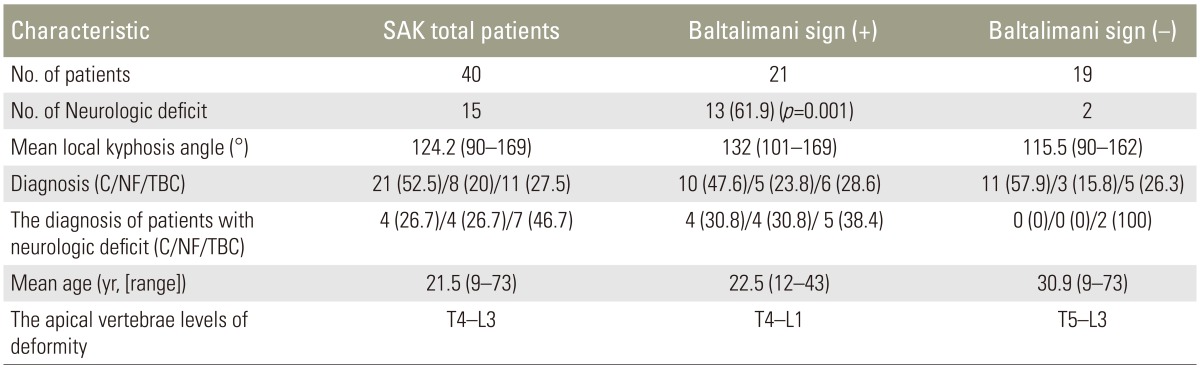
Demographic characteristics
Baltalimani sign showed a sensitivity and specificity PPV and NPV of 61.9%, 86.7%, 89.5%, and 68.8%, respectively, for the risk of the neurological deficits. Cohen's kappa value was moderate (κ=0.506).
The percentages of etiological factors were similar between the total patient group (40) and Baltalimani sign (+) group (21); in addition, local kyphosis angles were also similar between the two groups. Thirteen patients out of 15 with neurological deficits had a positive Baltalimani sign. In addition, all the levels of kyphotic apex in patients with neurological deficits were in the thoracic spine (T4–T12, spinal cord). The post-tuberculosis kyphosis and neurofibromatosis with Baltalimani sign have a more neuro-aggressive etiology than congenital kyphosis with Baltalimani sign.
Discussion
The development of neurological deficit risk in angular kyphosis patients may be related to age, etiology, type of congenital pathology, involved level, and severity of sharp local kyphosis. Baltalimani sign may help to explain the relationship of these factors to neurological deficits. Congenital kyphosis is caused by a mismatch during the final stages of ossification and cartilage formation in embryological development. Ongoing growth in the posterior elements of the spine when there is a formation and/or segmentation failure in anterior structures of the spinal column may cause progressive segmental sharp kyphosis [12]. Other mechanisms, such as severe vertebral body and disc destruction in spinal tuberculosis can cause local, severe kyphotic deformity. Another mechanism for severe kyphosis is the dystrophic variation that occurs in neurofibromatosis. Therefore, as kyphosis in all SAK is very sharp, Baltalimani sign is seen in the anteroposterior plane for sagittal balancing. Specifically, the region under sharp kyphosis is curved to form severe lordosis for sagittal balance so that vertebrae are seen with an axial orientation on anteroposterior radiographs. Paraplegia may occur as a result of both direct compression and stretching of the spinal cord over the deformed region at a greater frequency in patients with Baltalimani sign than in patients without Baltalimani sign because of the presence of the posterior sharp edge of middle vertebral column in the kyphotic segment. There are many influencing factors causing neurological deficits other than those appearing on radiological images. However, our study showed that, at the least in angular kyphosis patients, Baltalimani sign was indicative of neurological deficit risk, especially in SAK.
In SAK, the spinal cord leans to the sharp edge at the posterior part of the apical vertebral body. The chronic mechanical compression and/or stretching of the spinal cord by this sharp edge of the vertebral body may lead to paraparesis or paraplegia. McMaster and Singh [1] have detected neurological injury development because of spinal cord compression in 11 of 112 (approximately 10%) congenital kyphosis cases (7 cases were type 1 kyphosis) whose mean kyphosis angle was 111°. Similarly, Winter et al. [2] have reported 12% paraparesis development in their series (all type 1 kyphosis). These data suggest that the risk of neurological deficits is predictably high in severe congenital kyphotic deformities [1213]. The literature indicates the development of paraplegia in advanced (late-stage) post-tuberculosis kyphotic deformity because of spinal cord compression [3456]. Paraplegia or paraparesis is uncommon in spinal deformities with underlying neurofibromatosis; however, SAK that accompanies existing spinal deformity may result in worsening of neurological deficits by either a compression or stretching effect on the spinal cord [7812]. Winter et al. [9] have reported six paraparesis cases with normal history within 33 cases of SAK with underlying neurofibromatosis (range, 80°–180°) [12]. These data demonstrate that regardless of etiology, the incidence of developing neurological deficits is considerably high in untreated SAK cases [1011].
Our study has shown that the incidence of developing neurological deficits in cases with local kyphosis angle >90° is high (37.5%), and closely related to severity of the deformity. Of course, other factors such as age, etiology, and level of sharp local kyphosis should not be ignored. In this study we have also concluded that the incidence of neurological deficits increased by 61.9% (p=0.001) in cases with Baltalimani sign. In addition, post-tuberculosis kyphosis and neurofibromatosis with Baltalimani sign are more neuro-aggressive etiological factors than congenital kyphosis with Baltalimani sign. This radiographic sign may guide the assessment for risk of neurological deficits in SAK.
The limitations of this study are the retrospective design, inclusion of patients with various etiologies, age of patients, number of patients, and variable apices of kyphosis. Further validation of the data can be performed with additional patients presenting with Baltalimani sign.
The development of neurological deficits risk in SAK can be related to age, etiology, type of congenital pathology, involved level, and severity of sharp local kyphosis [1213151617]. As the inverted Napoleon's hat sign in the frontal plane demonstrates severe high-grade spondylolisthesis on sagittal plane; accordingly, Baltalimani sign in the frontal plane may be useful to demonstrate SAK [18]. Specifically, the detection of Baltalimani sign on frontal views can be a beneficial diagnostic tool to predict the severity of sharp kyphosis. In conclusion, the detection of Baltalimani sign in SAK cases may contribute to the development of neurological deficit risk criteria.
Conclusions
The detection of Baltalimani sign (1) is visible on radiographs that are recorded with adequate radiation dose and quality, (2) may be a helpful diagnostic sign in SAK without the need for lateral radiographs, (3) may be a warning criterion in terms of the risk of neurological deficits, and (4) may be a prognostic indicator of developing perioperative neurological deficit risk.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.