Does Vertical Ground Reaction Force of the Hip, Knee, and Ankle Joints Change in Patients with Adolescent Idiopathic Scoliosis after Spinal Fusion?
Article information
Abstract
Study Design
Comparative cross-sectional study.
Purpose
We measured the vertical ground reaction force (vGRF) of the hip, knee, and ankle joints during normal gait in normal patients, adolescent idiopathic scoliosis (AIS) patients with a Cobb angle <40° and in AIS patients with spinal fusion. We aimed to investigate whether vGRF in the aforementioned joints is altered in these three groups of patients.
Overview of Literature
vGRF of the lower limb joints may be altered in these groups of patients. Although it is known that excessive force in the joints may induce early arthritis, there is limited relevant information in the literatures.
Methods
We measured vGRF of the hip, knee, and ankle joints during heel strike, early stance, mid stance, and toe-off phases in normal subjects (group 1, n=14), AIS patients with Cobb angle <40° (group 2, n=14), and AIS patients with spinal fusion (group 3, n=13) using a gait analysis platform. Fifteen auto-reflective tracking markers were attached to standard anatomical landmarks in both the lower limbs. The captured motion images were used to define the orientations of the body segments and force exerted on the force plate using computer software. Statistical analysis was performed using independent t-test and analysis of variance to examine differences between the right and left sides as well as those among the different subject groups.
Results
The measurements during the four gait phases in all the groups did not show any significant difference (p>0.05). In addition, no significant difference was found in the vGRF measurements of all the joints among the three groups (p>0.05).
Conclusions
A Cobb angle <40° and spinal fusion did not significantly create imbalance or alter vGRF of the lower limb joints in AIS patients.
Introduction
Ground reaction force (GRF) is an important element acting on the joints of the lower limbs. Lower limb or spinal deformities may change the normal biomechanics of the human body and alter GRF of the knee, hip, and ankle joints. The lower limbs, pelvis, and spine are intimately interconnected and form a single body unit. Normal gait requires normal and balanced functioning of muscles acting on mobile hips and knees as well as functional spinal segments and pelvis [12345].
Spinal deformity, particularly scoliosis, is a relatively common condition. Adolescent idiopathic scoliosis (AIS) alters the alignment of the trunk, and in severe cases, the affected patients require spinal fusion for deformity correction. Spinal fusion involving a significant number of vertebral levels may interfere with the biomechanics of the hip, knee, and ankle joints because it restricts the normal “orchestraic” movement of the spinal segments, disturbs the normal distribution of load across the joints, and causes early degenerative changes in the joints in long run [16]. A reduction in muscle efficiency and excessive energy expenditure [57] have also been reported to contribute to these changes.
Vertical GRF (vGRF) is an important force component that thrusts the joints upward during walking. vGRF is directly proportional to the body weight as it counters the overall body weight. The measurement of gait parameters and vGRF has been widely used to analyze abnormal lower limb loading [8910], because such measurements provide objective information for analysis of joint loading during normal gait.
The reports on GRF acting on all major joints of the lower limbs involving normal subjects, normal AIS patients, and AIS patients with spinal fusion in a single study are rare. The present study investigated the effects of scoliosis deformity and spinal fusion on vGRF acting on all major joints of the lower limbs. We postulated that an alteration of spinal alignment and movement will result in significant biomechanical changes in the joints, which, in the long run, may induce early degenerative arthritis.
Materials and Methods
This is a comparative cross-sectional study conducted in our gait laboratory using an optical motion capture system comprising six high-resolution digital cameras.
The subjects included both males and females with an age range of 8–25 years. All subjects fulfilled the inclusion criteria. Patients with non-idiopathic scoliosis, lower limb and other spinal pathologies, postoperative complications, and back pain were excluded from this study. All scoliosis patients were diagnosed based on their clinical and radiological assessments. All subjects were treated surgically without orthosis because of the curve severity at presentation.
The subjects were categorized into three groups: group 1, subjects without any spinal deformity (Cobb angle <5°); group 2, subjects with AIS (Cobb angle, 20°–40°); and group 3, subjects with AIS who had undergone spinal fusion at least 1 year before the assessment. The subjects' weight, height, and bilateral thigh circumference were measured and recorded.
The subjects were briefed on how to perform a standardized gait on the gait analysis platform, and a video of the procedure was demonstrated to them for learning purpose. Reflective tracking markers were attached to the subjects' right and left iliac crests, anterior superior iliac spines, greater trochanters, hips and medial and lateral knees, medial and lateral ankles, heels, and 2nd and 5th metatarsal heads [11]. Then, the subjects were asked to walk as naturally as possible, following the walking speed recommended in a previous study that also involved a similar study population[12]. The captured motion images were used to define the orientations of the body segments and the force exerted on the force plate during the gait analysis using computer software (Qualisys Track Manager, visual 3D; Qualisys, Gothenburg, Sweden). We measured vGRF of the hip, knee, and ankle joints of the subjects from all three groups. Following this, we analyzed the effect of scoliosis deformity and spinal fusion on vGRF of the aforementioned joints using the normal group as control. vGRF measurements at four different gait phases—heel strike, early stance, mid stance, and toe-off—were performed.
The measurements obtained were analyzed using IBM SPSS Software ver. 23.0 (IBM Corp., Armonk, NY, USA). vGRF between the left and right sides was compared using independent t-test and that among the three groups was compared using analysis of variance. Post-hoc analysis was performed wherever appropriate. This study was approved by the Research and Ethics Committee of School of Medical Science, Universiti Sains Malaysia (HREC code: USM/JEPeM/14100347).
Results
Of the 41 subjects included in this study, 31 were women and 10 were men. Groups 1 and 2 comprised 14 subjects each, and group 3 comprised 13 subjects. The mean ages of the subjects in groups 1, 2, and 3 were 14, 15, and 17 years, respectively; furthermore, the median body weights of the subjects were 44.9, 42.4, and 41.0 kg, respectively. No significant differences were noted in the mean weight (p=0.135) and height (p=0.929) among the groups. The median Cobb angle for groups 2 and 3 (prior to fusion) were 30.4° and 69.8°, respectively.
vGRF measurements of the hip, knee, and ankle joints for groups 1–3 are shown in Tables 1, 2, 3, respectively. In group 1, generally, vGRFs of the hip and knee joints were higher on the right side than on the left side during all gait phases except during the toe-off and heel strike phases, respectively. vGRF of the ankle joint was higher on the right side during all gait phases. However, no significant difference was noted between vGRFs of both the sides (p>0.05).

Vertical ground reaction force measurement in the hip, knee, and ankle joints in group 1

Vertical ground reaction force measurement in the hip, knee, and ankle joints in group 2

Vertical ground reaction force measurement in the hip, knee, and ankle joints adolescent idiopathic scoliosis in group 3
In group 2, vGRFs of the hip and knee joints were higher on the left side than on the right side during all gait phases except during the mid stance phase. vGRF of the ankle joint was higher on the right side during all gait phases except during the early stance phase. As in group 1, no significant difference was noted between both the vGRFs of both the sides (p>0.05).
In group 3, vGRFs of the hip and knee joints were higher on the right side than on the left side during heel strike and early stance phases. However, vGRF of the ankle joint was higher on the left side during all gait phases except during the early stance phase. As in other groups, no significant difference was noted between both the sides (p>0.05).
The vGRF measurements of all the joints among groups 1–3 did not show any significant difference (p>0.05) (Table 4). The vGRF profiles of all the joints have been presented in Fig. 1.
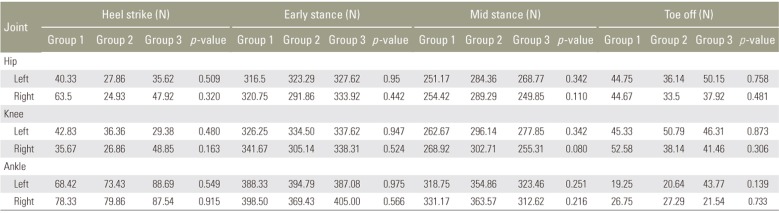
Comparison of p-values of vertical ground reaction force in the hip, knee, and ankle among the three groups using analysis of variance
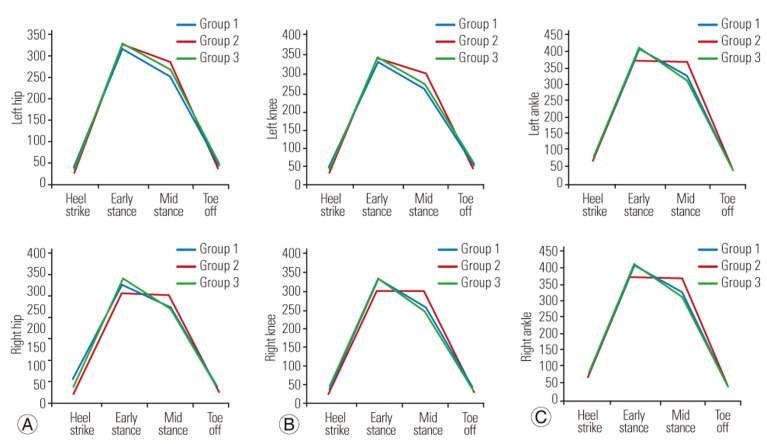
(A) vGRF profile of the left and right hips in the three study groups. (B) vGRF profile of the left and right knees in the three study groups. (C) vGRF profile of the left and right ankles in the three study groups. vGRF, vertical ground reaction force.
Discussion
AIS exerts significant effects on the spinal anatomy, mobility, and balance, which may alter the locomotion of the affected individual. Attempts to correct the spinal deformity and fuse the spine are believed to facilitate the restoration of the normal center of gravity and center of the body pressure (COP). However, the excursion of COP in different gait phases may be altered due to fused spinal segments. The deformity may cause asymmetrical loading of one side of the lower limb due to the convexity or concavity of the spine. The present study intended to understand the biomechanical effect of idiopathic scoliosis on the lower limb joints, which may predispose these joints to early degenerative changes in the long run.
Currently, the most commonly preferred approach to study these mechanical changes is analyzing GRF of the joints [1314]. Gait analysis provides an insight into body balancing during normal gait. Individuals with idiopathic scoliosis may exhibit abnormal gait or abnormal body balance due to the shifting of COP. As a person walks, few major forces of a joint act to keep the center of gravity and excursion of COP in check so as to maintain the balance of the entire body [15].
vGRF is required to thrust the joints upward during walking. In this study, we observed that vGRF was lowest during the heel strike phase, with increasing trend noted during the early stance and mid stance phases and a decreasing trend up to the baseline. The asymmetrical pattern of vGRF was observed across all groups; similar findings were also reported recently by Park et al. [12]. Nearly symmetrical patterns of vGRF were observed when COP of the body shifted to the left and right during the walking phases. Although our findings showed shifting of higher vGRF between the right and left sides of the joints in normal AIS patients and in AIS patients with spinal fusion, these phenomena were not significant.
We measured vGRF of three major lower limb joints in normal subjects, normal AIS patients, and AIS patients with spinal fusion. Weight and height are the important factors affecting GRF in an individual. However, no significant differences in these parameters were found among the three study groups, which ensured uniformity among the patients across all the groups.
We found that vGRF of the hip joint was similar on both the sides throughout the walking phase in the normal group (group 1, control). Furthermore, vGRF of the hip joint was similar on both the sides among subjects in both groups 2 and 3. Moreover, vGRF of the hip joint across all three groups did not show any significant difference. Thus, the three groups with different spinal curvature and mobility did not show any significant difference regarding vGRF during all gait phases. These observations indicate that a spinal deformity of <40° did not significantly alter the hip vGRF. Even a significant number of fused spinal segments did not change the gait significantly. Our observations are in concordance with the findings of Mahaudens et al. [5]. It is expected that spinal fusion would modify the characteristics of normal gait; however, their study showed that surgery did not induce asymmetric gait or any significant differences in gait. In fact, surgery improves the gait and mechanical parameters. Similarly, for the knee joints, vGRFs on both the sides in normal AIS subjects and AIS subjects with fused spine were similar. vGRF of the knee joints did not show any significant difference across all three groups and all gait phases. Similar observations were also noted in the ankle joints. Our findings cumulatively indicate that spinal deformity and fused spinal segments did not significantly alter the function of knee and ankle joints.
There is a considerable concern that spinal deformity associated with AIS [16] and the limited spinal motion following spinal fusion [515] may predispose AIS patients to imbalance forces between the right and left lower limb joints and induce early degenerative arthritis of these joints. Our study showed minimal vGRF differences between normal AIS as well as post-fusion AIS patients and normal persons, which is in agreement with the reports of some previous studies [515]. It is, thus, indicted that these groups of patients and normal subjects are at a similar risk of developing degenerative arthritis of their joints.
The present study involved young participants aged <25 years. A significantly higher vGRF than that reported in our study was reported for older participants in a previous study, thus, indicating an increased risk of arthritis [16]. Therefore, other co-factors, including obesity and high activity levels, are probably the actual cause of an early arthritis, rather than the spinal deformity or rigidity.
There are a few limitations to this study. The number of subjects enrolled in each group was small. A larger sample size may provide a better statistical analysis. In addition, this was a retrospective study, which has its inherent weaknesses. Moreover, changes in vGRF could have been more prominent if the walking was tested at varied speeds rather than at the natural walking speed. Additional information about the muscular mechanical work power tested through a treadmill test or by conducting electromyography would also have been useful in predicting early arthritis. Therefore, a prospective study involving the same patients followed up from the time they were diagnosed until they underwent spinal fusion would be ideal for analysis in the future.
Conclusions
This study established the vGRF profiles of the hip, knee, and ankle joints in normal subjects, AIS patients with Cobb angle <40°, and AIS patients with spinal fusion. vGRFs of the evaluated joints in the subjects with spinal deformity and spinal fusion remained unaltered and were similar to those in the normal population. Scoliosis deformity <40° and spinal fusion in AIS patients does not create any significant vGRF imbalance or changes between the joints on the right and left sides in the lower limbs.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.