Introduction
Spinal tuberculosis (TB) is a destructive form of TB. It accounts for approximately half of all cases of musculoskeletal TB. The incidence of spinal TB is increasing in developing countries. Gross destruction of the vertebral bodies and discs by TB often leads to kyphotic deformity [12]. Though many patients can be cured by chemotherapy, surgery is often necessary for spinal decompression and deformity correction. Previous studies showed that surgical treatment is an important strategy for the treatment of spinal TB [34].
In 1934, Ito et al. [5] first described the anterior debridement approach for spinal TB; however, this approach may reduce the biomechanical stability of the spine, and it is common to observe residual kyphosis at the end of treatment [6]. Thus, anterior debridement combined with posterior fusion and fixation was developed, which helped arrest the disease early and prevented the progression of kyphosis as well as corrected it. However, the combined procedures were associated with longer surgeries, greater blood loss, more postoperative complications, and a longer hospital stay. The purpose of the present study is to investigate the efficacy and safety of a one-stage posterior transpedicular approach for achieving circumferential fusion.
In recent years, global TB incidence has increased because of population migration, increase in the number of patients with human immunodeficiency virus (HIV) infection, and emergence of antibiotic-resistant strains, among other reasons [78]. India has the highest burden of TB. The World Health Organization (WHO) statistics for 2014 give an estimated incidence figure of 2.2 million cases of TB for India out of a global incidence of 9 million [9]. In India, TB is not restricted to immunocompromised patients [9]. Spinal TB leads to increased pressure on the spine and therefore, causes neurological injury. The chief aim of surgical treatment is focal clearance of TB, relief of spinal nerve compression, reconstruction of spinal stability, and correction of the spinal deformity. This study reviewed patients with thoracolumbar spinal TB following one-stage fixation, debridement, anterior reconstruction, and circumferential fusion using a single posterior approach only.
Materials and Methods
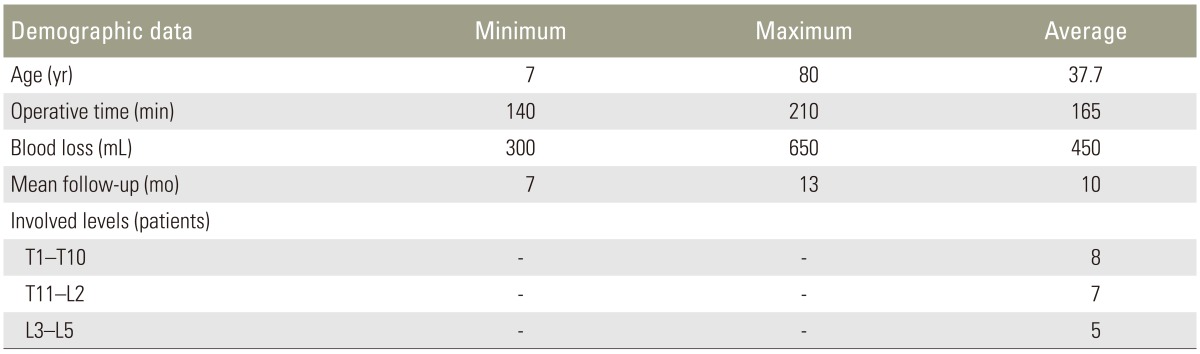
The study design of this study is a prospective case series. We have included patients whose thoracolumbar spine was affected. Patients who had levels affected in areas other than the thoracolumbar spine, those who were immunocompromised or HIV positive, or who have undergone any previous surgical interventions for the spine were excluded from our study. Twenty patients who presented with signs and symptoms of vertebral osteomyelitis of the thoracolumbar region were assessed using X-rays, magnetic resonance imaging, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels. On preoperative assessment, clinical assessment was performed using the visual analogue scale (VAS), neurological assessment was performed using the American Spinal Injury Association (ASIA) scale, and radiological assessment was performed using anterior-posterior and lateral X-rays and sagittal alignment by the measurement of the Cobb angle. We divided the patients in thoracic (T1ŌĆōT10), thoracolumbar (T11ŌĆōL2), and lumbar (L3ŌĆōL5) groups and classified the patients on the basis of the Gulhane Military Medical Academy (GATA) classification developed by Oguz et al. [10]. The patients also underwent posterior transpedicular approach surgery. The details of the surgical technique have been described in the following section. Intraoperative neuromonitoring was not used. Operative time and intraoperative blood loss were recorded. All patients were confirmed to have TB by histopathology testing, sensitivity was detected by a TB gene expert [11], and culture and sensitivity of the pathological specimens were sent preoperatively. After pathological diagnosis, all patients were started on medical management of TB as per Revised National Tuberculosis Control Program (RNTCP) guidelines issued by the government (Table 1) [1213]; nine patients were already on medical management to treat TB. Patients were observed at intervals of 3 months postoperatively for clinical assessment in terms of neurological improvement and VAS, laboratory assessment in terms of ESR and CRP, radiological assessment in terms of the Cobb angle, and assessment of fusion using Lenke's classification [14]. Data were analyzed using the SPSS ver. 13.0 statistical software package (SPSS Inc., Chicago, IL, USA). The paired t-test was used to examine the statistical significance between the two groups. All test results were considered significant at p<0.05.
1. Surgical technique
All patients were operated under general anesthesia while in the prone position. Through a posterior midline approach, the lamina, facet joints, and transverse processes were exposed. Exposing the vertebral laminae of involved segments, the posterior pedicle screws were installed. Laminectomy, according to the extent of cord compression, was performed before debridement of the affected intervertebral discs and vertebrae. Facetectomy and pediculectomy were also performed at appropriate levels. To obtain a broader view, one spinal nerve on the focal side may have been sacrificed in the thoracic levels and abscesses were evacuated. Following completion of the debridement, the deformity was corrected by installing permanent rods with compression maneuvers under vision. Anterior reconstruction was achieved using an appropriate-sized cage, and autograft and posterior interbody grafts were used after ensuring that the spinal cord was not compressed.
Results
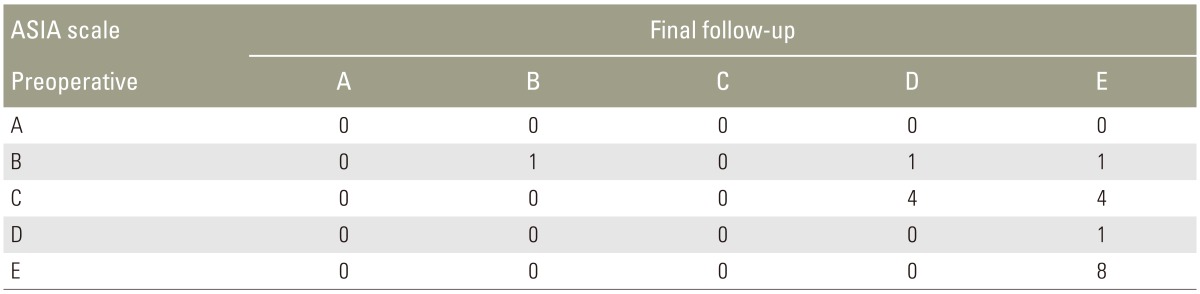
Patients aged 7ŌĆō80 years were included in the study, and the average age was 37.7 years. Of the 20 patients, 8 (40%), 4 (20%), 4 (20%), and 4 (20%) were in 7ŌĆō30, 31ŌĆō45, 46ŌĆō60, and >60 years range, respectively. In our study, 8 patients (40%) were females and 12 (60%) were males. There were 8 patients in the thoracic (T1ŌĆōT10) category, 7 patients in thoracolumbar (T11ŌĆōL2) category, and 5 patients in the lumbar (L3ŌĆōL5) category (Table 2). All patients belonged to type III according to Oguz classification [10]. No worsening of neurology was observed postoperatively or at follow-up. Better results in the ASIA scale were recorded in the patients who underwent surgery (Table 3). The ASIA scale improved in 11 of the 20 patients, while nine patients had the same scores postoperatively, and two patients who were diagnosed with nonunion showed no worsening in neurology. In one patient who presented with a pathological fracture (ASIA type B), there was no improvement in neurology.
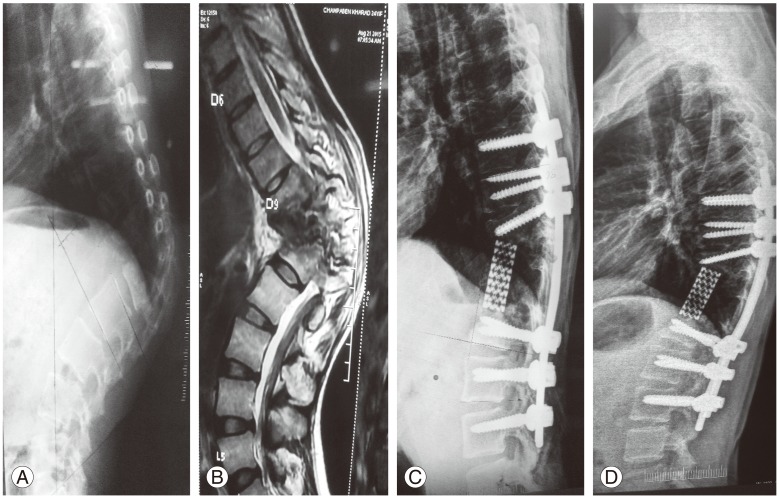
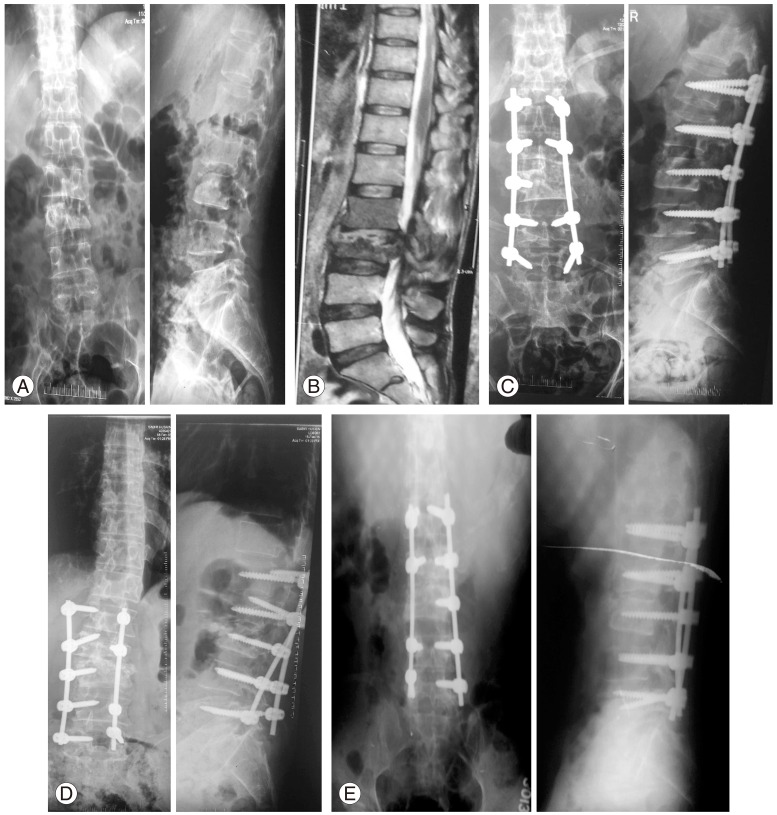
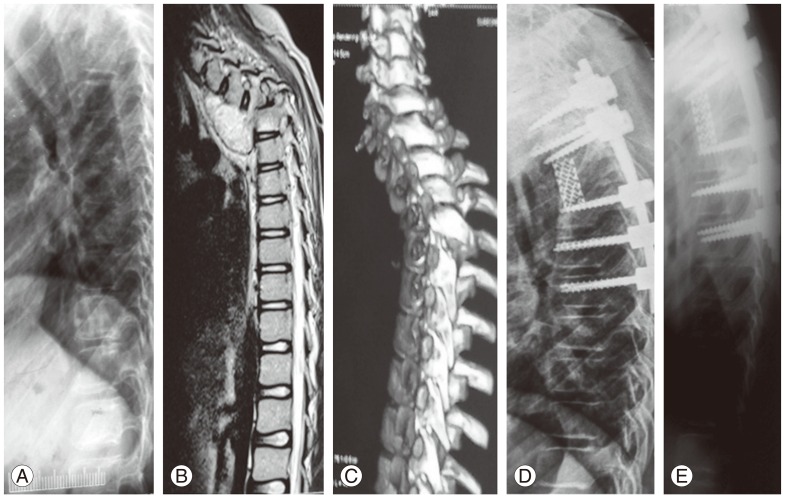
Bony fusion was achieved in 90% of the patients. Fusion was assessed according to the Lenke classification of X-ray fusion [13]. The Cobb angle improved from an average of 27.5┬░ (10┬░ŌĆō85┬░) preoperatively to a postoperative angle of 6.25┬░ (0┬░ŌĆō25┬░) and a mean 6.95┬░ at the final follow-up (Figs. 1, 2, 3).
Discussion
Spinal TB prevails in many parts of the world and is a severe orthopedic problem [15], usually presenting with kyphosis, neurological deficit, and even paraplegia [1617]. Thoracolumbar lesions, the junctional region of thoracic and lumbar lesions, have the highest propensity to develop morphological changes likely to predispose to deformity progression in patients with spinal TB [6]. Early therapy has become important for the treatment of thoracolumbar spinal TB. Although anti-TB chemotherapy effectively inactivates TB, vertebral collapse may continue. Kyphosis requiring extensive reconstructive procedures is a common complication of spinal TB in patients treated with chemotherapy alone [1819]. Surgery for TB spondylitis is generally considered to be an adjuvant of effective chemotherapy. Indications for surgery are neurological deficit, spinal instability, severe and/or progressive kyphosis, no response to chemotherapy, and nondiagnostic and large paraspinal abscess [1617].
Various surgical methods have been used to treat patients with spinal TB, but few studies have been reported on the use of one-stage posterior decompression, interbody grafts and transpedicular instrumentation, and circumferential fusion for the treatment of patients with thoracolumbar spinal TB. Because the inflammation is usually located in the anterior aspect, anterior debridement and strut grafts are recommended by some surgeons [20]. This method can provide direct access to the disease focus, effective debridement of the lesion, and decompression of the spinal cord. However, the procedure may result in the progression of kyphosis as a consequence of failure of the bone graft [202122].
In view of the complications of this method, isolated posterior instrumentation [23] or additional posterior instrumentation, which is applied to reduce kyphotic deformities and prevent correction loss and graft failure, has been applied by some surgeons [2425]; however, this combined procedure has a longer operation time and healing duration and higher surgical trauma. We preferred the posterior approach because it reduces total operative time and morbidity and allows early mobilization, which reduces the complication risk of long-term bed rest and decreases hospitalization cost. In addition, a posterior approach offers good access to the spinal canal for efficient decompression of the neural elements, particularly in cases of epidural suppuration, and renders good clinical results [2627].
Afterwards, a postoperative regimen of anti-TB drugs allows the drugs to effectively enter pathologic sites to kill tuberculomyces and recover the areas of bone that are infiltrated by, but not necrotic with, tuberculous disease and to resolve possible remaining abscesses that cannot be completely drained by posterior decompression [28]. Of the 20 patients, nine were already on medical management of spinal TB. The reasons for failure of medical management were a delay in the diagnosis or treatment, noncompliance of patients, involvement of more than two vertebrae, increase in the duration of the disease, decrease in the immunity of the patient to fight the disease, and unacceptable sagittal malalignment leading to pain in spite of a healed lesion.
The surgical approaches are divided into posterior and anterior. Posterior approaches include transpedicular and lateral extracavitary approaches and anterior approaches include transthoracic and retroperitoneal approaches. In the present study, we performed the procedure of one-staged posterior debridement, pedicle fixation, and circumferential fusion using the transpedicular approach. In all patients, diagnosis should be confirmed by culture and sensitivity of the pathological specimen, histopathology testing, and a TB gene expert to detect sensitivity to routine drugs, according to RNTCP criteria.
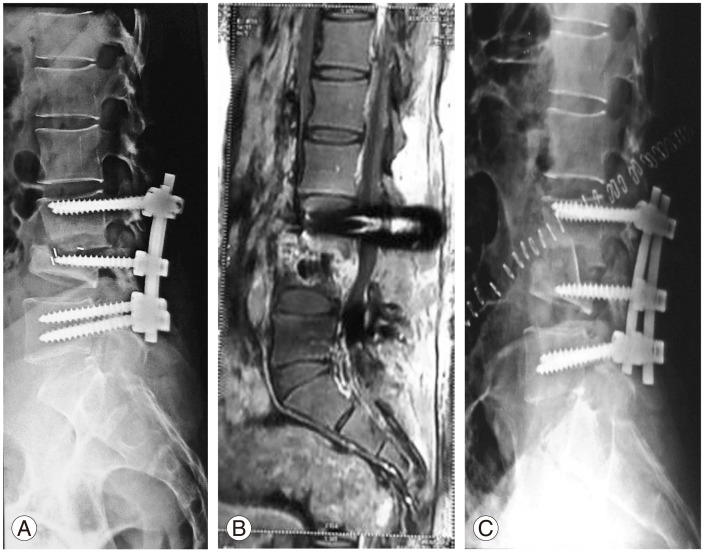
The ASIA scale scores were significantly better at the final follow-up visit than those preoperatively (p<0.05). The VAS scores of the patients decreased from 6.9 preoperatively to 2.55 at the final follow-up visit. The preoperative and postoperative mean kyphotic Cobb angle were 27.5┬░ and 6.25┬░ in the present study, and the difference was statistically significant (p<0.05). There were no intraoperative complications. Postoperatively, two patients were diagnosed with nonunion. Refixation was performed in one patient (Fig. 2), and the removal of the cage and tricortical bone grafting by the anterior retroperitoneal approach was performed on the other patient (Fig. 4). No significant loss of deformity correction was noted in any patient at the final follow-up. It was concluded from our study that the final outcome of one-stage posterior approach was satisfactory.
Advantages of one-staged posterior surgery are kyphosis correction, single-stage procedure, low rate of infection, decreased hospital stay, and low blood loss. Disadvantages of one-staged posterior surgery include a risk of damage to the cord, thereby increasing the chances of neurological deficit, inability to use a bigger cage, difficulty in anteriorly approaching the lumbar spine as the nerve roots cannot be sacrificed, and involvement of more levels for fusion.
In conclusion, the procedure of single-staged posterior debridement, transpedicular screw fixation, and circumferential fusion by a transpedicular approach is an effective and safe procedure for surgical treatment of mono- or polysegmental thoracic and lumbar spinal TB. The antitubercular treatment protocol as per RNTCP guidelines is effective in ameliorating the disease and reducing the bacterial load. Despite the satisfactory results of our series, we acknowledge some limitations. First, the duration of follow-up was only long enough for short-term results but did not provide enough time for the final result. Long-term follow-up for this procedure will be necessary to further assess its application in the treatment of thoracolumbar spinal TB. Moreover, the small sample of patients limits the power of our conclusions, and a larger, randomized, controlled trial is required to elucidate the benefits and risks of our method. However, data may serve to aid decision-making and the design of future prospective studies.