Neuropathic Pain Related with Spinal Disorders: A Systematic Review
Article information
Abstract
Systematic literature review. To review the evidence from high-quality studies regarding the treatment of neuropathic pain originating specifically from spinal disorders. In general, treatment guidelines for neuropathic pain cover all its various causes, including medical disease, peripheral neuropathy, and cancer. However, the natural history of neuropathic pain originating from spinal disorders may differ from that of the pain originating from other causes or lesions. An expert research librarian used terms related to neuropathic pain and spinal disorders, disc herniation, stenosis, and spinal cord injury to search in MEDLINE, Embase, and Cochrane CENTRAL for primary research from January 2000 to October 2015. Among 2,313 potential studies of interest, 25 randomized controlled trials (RCTs) and 21 systematic reviews (SRs) were included in the analysis. The selection was decided based on the agreement of two orthopedic surgeons. There was a lack of evidence about medication for radiculopathy arising from disc herniation and stenosis, but intervention procedures, including epidural block, showed positive efficacy in radiculopathy and also limited efficacy in spinal stenosis. There was some evidence based on the short-term follow-up regarding surgery being superior to conservative treatments for radiculopathy and stenosis. There was limited evidence regarding the efficacy of pharmacological and electric or magnetic stimulation therapies for neuropathic pain after spinal cord injury. This review of RCTs and SRs with high-quality evidence found some evidence regarding the efficacy of various treatment modalities for neuropathic pain related specifically to spinal disorders. However, there is a need for much more supportive evidence.
Introduction
Neuropathic pain can occur following a lesion or a disease of the somatosensory nervous system and can result in problems of poor physical, cognitive, and psychosocial health [1]. The appropriate management of neuropathic pain, which should be specific to each patient, has proven difficult [2]. Many different treatments have been investigated; however, the literature is sizable, rapidly evolving, and lacks practical information about clinical aspects of managing patients [3]. Neuropathic pain can be caused by a number of different diseases (e.g., diabetes mellitus, herpes zoster, cancer, spinal disorders, and human immunodeficiency virus infection) as well as by interventions (e.g., chemotherapy and surgery) and trauma (e.g., spinal cord injury). The treatment varies according to the etiology and chronicity.
Spinal disorders, including radiculopathy due to disc herniation, spinal stenosis, or spinal cord injury, are common causes of neuropathic pain. However, most treatment guidelines [34] have included all etiologies that can cause neuropathic pain, and it has been rare for a review article to deal with neuropathic pain related only to spinal disorders. The purpose of the present review was to consider high-quality evidence from extensive reviews on the treatment for neuropathic pain, focusing only on spinal disorders, including radiculopathy due to disc herniation, spinal stenosis, and spinal cord injury. The treatment modalities investigated were pharmacological treatment, intervention procedures, including nerve block procedures and physiotherapy, and surgical treatment.
Materials and Methods
1. Search strategy
We used a range of sources to identify relevant literature, undertaking a comprehensive literature search of major medical, health-related, scientific, and health economic electronic bibliographic databases. We paralleled the comprehensive searches through a clearly defined search strategy using the MEDLINE, Embase, and Cochrane CENTRAL databases. The search included MeSH terms, Embase data, and free text. Only studies published in English were included. The main search was performed in January 2000 and updated in October 2015.
2. Inclusion criteria
Studies were eligible for inclusion if they were full text reports of systematic reviews (SRs) or randomized controlled trials (RCTs). The studies could include participants of any age and in any setting who were treated for neuropathic pain or chronic pain related only to spinal disorders (using the search terms “spine,” “spinal,” “cord,” “cord injury,” “radiculopathy,” “stenosis,” “disc herniation,” and “myelopathy”) and could involve any surgical, non-surgical, or interventional treatment (using the search terms “medical,” “drug,” “conservative treatment,” “intervention,” “block,” “epidural,” “intrathecal,” “nerve,” “steroid,” “injection,” and “surgery,” alone or in combination). The outcomes assessed included pain intensity, pain-related disability, analgesic use, function, mobility, activities of daily living, characteristic symptoms or indicators of disease, patient satisfaction, quality of life, views/themes pertaining to qualitative data, adverse events, and mortality.
3. Exclusion criteria
Studies on animals and back pain related only to arthritic changes were excluded, as were any that included the following search terms: “post spinal surgery syndrome,” “failed back surgery syndrome,” “herpes zoster,” “postherpetic,” “cancer,” “oncology,” “metastatic,” “metastasis,” “chemotherapy,” “malignancies,” “malignancy,” “diabetic neuropathy,” “diabetic,” “trigeminal neuralgia,” “neuralgia,” “arthritis-related pain,” “postamputation,” “amputation,” “phantom limb,” “peripheral neuropathic pain,” “inherited neuropathies,” “occipital neuralgia,” “headache,” “complex regional pain syndrome,” “multiple myeloma,” “multiple sclerosis,” “sickle cell disease,” “AIDS,” “stroke,” and “post-stroke.”
4. Evidence and recommendation assessment
New and additional evidence was appraised using the Scottish Intercollegiate Guidelines Network protocol for SRs and the Agency for Healthcare Research and Quality methodology checklist for RCTs [56]. The recommendations were classified as A, B, C, or D based on the results of the evidence (Table 1). The final decision on the recommendation grade for each method was attained based on agreement among four raters.
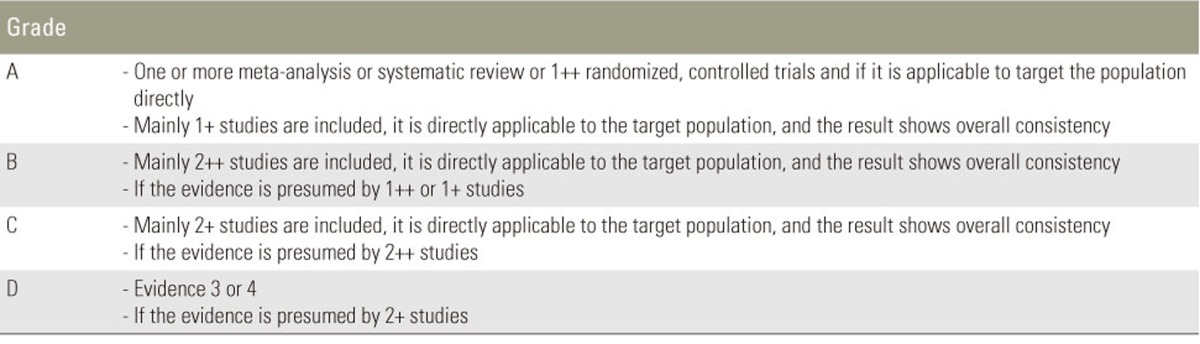
Recommendation grade
5. Study selection
Only articles with evidence rated as 1++ (high-quality meta-analyses and SRs based on RCTs or RCTs with a very low risk of bias) and 1+ (well-designed meta-analyses and SRs based on randomized or non-randomized clinical trials or RCTs with a low risk of bias) were included. Two independent reviewers applied the inclusion/exclusion criteria to the studies identified through the searches and screened the titles and abstracts followed by the full text of any reports that appeared to fulfill the inclusion criteria. Any disagreement over the inclusion of reports was resolved through a discussion.
Results
1. Search results
The database searches identified 2,313 potential studies of interest. Of these, 111 articles were retrieved for evaluation of the full text. Seven of these articles were excluded because they were treatment guidelines rather than SRs. So, 45 RCTs and 59 SRs were included. Of the 45 RCTs, one article in Spanish, 13 articles not related to spinal disease, one article about assessing fusion outcome, and four articles about postoperative assessment were excluded. Another trial was excluded because it was covered in an SR that we had already included. Of the 59 SRs, 21 articles were excluded because they were protocol designs rather than SRs, 16 articles because they were not related to spinal disorders, and one because its literature search was not comprehensive. Finally, 25 RCTs and 21 SRs were included and reviewed. All selections throughout this process were based on an agreement between two orthopedic surgeons. Fig. 1 presents a flowchart of the selection process, and the results are summarized in Table 2 [7891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253].

Flowchart illustrating the selection process for the published literature. RCT, randomized controlled trial; SR, systematic review.
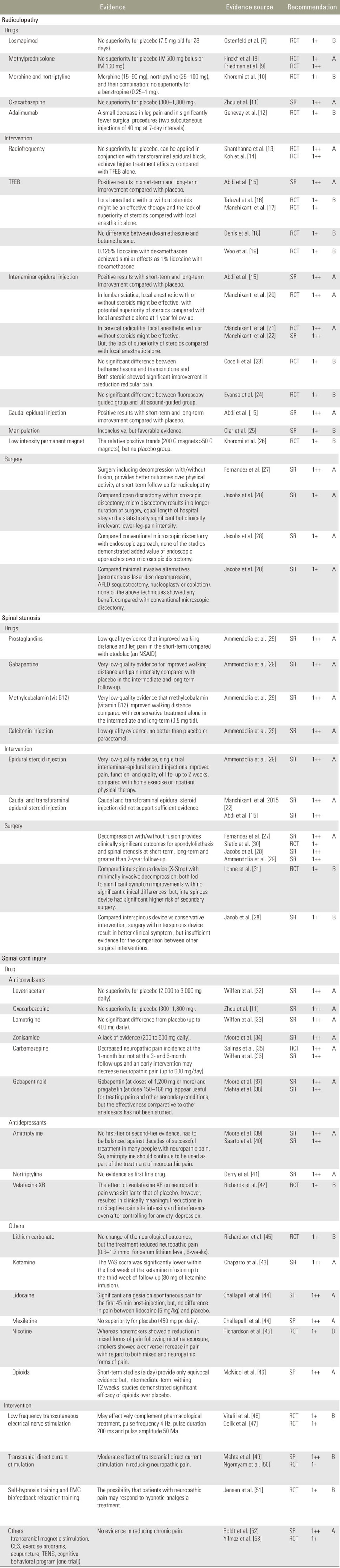
Summarization of enrolled studies
2. Results of spinal disorders
1) Radiculopathy
(1) Drugs
The systemic short-term use of losmapimod, which acts as a selective inhibitor of the enzyme family known as p38 mitogen-activated protein kinases, at a dose of 7.5 mg twice a day for 28 days could not be differentiated from placebo in terms of an acceptable quality of analgesia [7]. A single systemic injection (intramuscular or intravenous) of methylprednisolone could not be differentiated from the use of placebo in terms of analgesia for acute (within 6 weeks) discogenic sciatica, and its effects showed insufficient evidence to recommend its use for acute sciatica despite a suggestion of its use in a young population with radiculopathy being beneficial [89]. The result of a short-term trial showed that 15 mg of oral morphine, 25 mg of nortriptyline, and their combination may be ineffective in the treatment of lumbar radiculopathy compared with an active placebo (benztropine); these results suggest that nortriptyline, morphine, and their combination has limited effectiveness in the treatment of chronic sciatica [10]. The long-term follow-up results of one SR provided moderate quality evidence that in comparison with a placebo, oxcarbazepine could neither significantly relieve pain nor improve patients' global impression scale [11]. The result of a short-term RCT provided low-quality evidence that 70 mg of adalimumab via two subcutaneous injections at 7-day intervals resulted in a small decrease in leg pain and significantly fewer surgical procedures [12].
(2) Interventions
The results of two RCTs provided high-quality evidence that the 42℃ radiofrequency therapy applied to dorsal root ganglia over 120 seconds for radiculopathy could not be differentiated from placebo in terms of analgesia [1314]. In comparison with a transforaminal epidural injection alone, the application of radiofrequency therapy in conjunction with a transforaminal epidural injection achieved higher treatment efficacy [14].
One SR with high-quality evidence showed strong evidence of a short-term benefit and moderate evidence of a long-term benefit of transforaminal epidural steroid injections in comparison with a placebo [15]. Two trials with acceptable evidence demonstrated that using steroids in transforaminal epidural injections was not superior to using local anesthetics alone [1617]. One RCT did not show a significant difference between dexamethasone, a nonparticulate corticosteroid, and betamethasone, a particulate corticosteroid, in reducing radicular pain [18]. One trial on the use of local anesthetics showed that using 0.125% lidocaine with dexamethasone achieved satisfactory effects similar to those using 1% lidocaine with dexamethasone, concluding that the use of low-dose lidocaine in cervical transforaminal injection may reduce the incidence of rare but fatal complications [19].
Another route for epidural injections is an interlaminar epidural block. One SR with high-quality evidence showed strong evidence of a short-term benefit and moderate evidence of a long-term benefit pertaining to interlaminar and caudal epidural steroid injections for radiculopathy compared with those pertaining to placebo [15]. Lumbar interlaminar epidural injections of local anesthetics with or without steroids may be effective in lumbar discogenic sciatica, with steroids shown to be potentially superior to local anesthetics alone based on a long term follow-up [20]. One RCT and one SR with high-quality evidence showed that cervical interlaminar epidural injections of local anesthetics with or without steroids may be effective but presented evidence that steroids were not superior to local anesthetics alone [2122]. One trial found no significant difference between betamethasone and triamcinolone in reducing radicular pain in the lumbar spine, but both steroids resulted in significant improvement in the reduction of radicular pain in the short term (within 6 weeks) [23]. One trial found no significant difference between fluoroscopy-guided and ultrasound-guided lumbar interlaminar epidural injections [24].
In physiotherapy, one SR showed inconclusive favorable evidence for spinal manipulation and mobilization in treating sciatica and back-related leg pain. However, there was only limited high-quality evidence for the effectiveness of manual therapy, with most evidence being low-to-moderate quality and inconsistent because of substantial methodological and clinical diversity [25].
The use of low-intensity permanent magnets has been studied in patients with chronic neck and osteoarthritic joints, showing a relative treatment effect of 200 G magnets, which appeared to exhibit a positive trend of benefit for lumbar radicular pain [26]. However, that study did not include a placebo group.
(3) Surgery
Two SRs involving a short-term follow-up showed that surgery, including decompression with or without fusion, provided better outcomes for radiculopathy than physical activity [2728]. When open discectomy and microscopic discectomy were compared, there was moderate-quality evidence pertaining to minimally invasive discectomy resulting in a longer duration of surgery, equal length of hospital stay, and a statistically significant but clinically irrelevant improvement in the intensity of lower leg pain. No studies demonstrated any added value of endoscopic approaches over microscopic discectomy [28]. One RCT with moderate-quality evidence compared minimally invasive alternatives (percutaneous laser disc decompression, automated percutaneous mechanical lumbar discectomy sequestrectomy, nucleoplasty, and coblation neucleoplasty) and concluded that none of these techniques showed any long-term benefit in comparison with conventional microscopic discectomy [54].
2) Spinal stenosis
(1) Drugs
One SR with high-quality evidence reported that the use of prostaglandins improved walking distance and leg pain in the short term compared with an active placebo (etodolac, a nonsteroidal anti-inflammatory drugs [NSAIDs]), but the trial provided only low-quality evidence [29]. In addition, intermediate and long-term follow-up results showed that gabapentin and methylcobalamin could improve walking distance and leg pain compared with placebo, but the two studies were graded as providing very low-quality evidence. A calcitonin injection could not be differentiated from placebo in terms of analgesia [29].
(2) Interventions
Epidural steroid injections may improve pain, function, and quality of life for up to 2 weeks compared with home exercise or inpatient physical therapy [29]. Another SR reported that caudal epidural steroid injections showed only limited evidence of benefit for low back pain and radiculopathy [15]. One RCT showed positive results of the usefulness of these injections for cervical spinal stenosis, but this was a preliminary report [22].
(3) Surgery
Three high-quality SRs and one RCT showed that surgery, including decompression with or without fusion, provided better clinical outcomes for spondylolisthesis and spinal stenosis than physical activity at the short-term and long-term follow-ups and at a follow-up after more than 2 years [27282930]. One RCT compared the effect of an interspinous process device (X-Stop) with that of minimally invasive decompression in patients with neurogenic intermittent claudication due to lumbar spinal stenosis, demonstrating no significant clinical differences between them in terms of pain relief or functional improvement, although the interspinous process device posed a significantly higher risk of secondary surgery [31]. Another SR reported that the interspinous process device appeared to result in better Zurich Claudication Questionnaire scores and a greater mean improvement of symptom severity compared with conservative interventions, but there was insufficient evidence pertaining to comparisons with other surgical interventions [28].
3) Spinal cord injury
(1) Drugs
One SR with high-quality evidence reviewed the efficacy of anticonvulsant drugs, concluding that levetiracetam [32], oxcarbazepine [11], and lamotrigine [33] were not more effective in reducing neuropathic pain than placebo and that zonisamide [34] also lacked evidence indicating pain relief in patients with neuropathic pain. One RCT demonstrated that an early intervention with carbamazepine for a group of patients with acquired spinal cord injury reduced the incidence of neuropathy found at the 1-month but not the 3- or 6-month follow-up; it did not reduce the incidence or intensity of neuropathic pain for long term in comparison with a placebo [35]. One SR concluded that carbamazepine is probably effective for some people with chronic neuropathic pain, although there were caveats and caution was needed when using it [36]. Recently, gabapentinoids, a type of anticonvulsant, have been widely used. Two SRs showed that gabapentin at doses of 1,200 mg or more was effective for some people with some painful neuropathies OR painful conditions, even potentially important residual biases [37], and that gabapentin (at doses up to 3,600 mg/day) and pregabalin (up to 300 mg/day) appeared to be useful for treating pain and other secondary conditions after spinal cord injury, although their effectiveness compared with other analgesics has not been studied [38].
Antidepressants can be used to treat neuropathic pain in patients with spinal cord injury. However, two SRs found that there was a lack of evidence regarding amitriptyline successfully treating any neuropathic pain condition [3940]. The lack of supportive unbiased evidence for a beneficial effect is disappointing, but this should be balanced against decades of successful treatment in many people with neuropathic pain, and amitriptyline should continue to be used as part of the treatment of neuropathic pain. The results of one SR did not support the use of nortriptyline as a first-line treatment. Effective medicines with much greater supportive evidence are available [41]. One RCT of adequate quality showed that the effect of venlafaxine XR on neuropathic pain was similar to that of placebo; however, its use resulted in statistically significant and clinically meaningful reductions in the intensity of nociceptive pain and interference even after controlling for anxiety and depression [42]. Venlafaxine XR could, therefore, complement current medications and procedures for treating pain after spinal cord injuries with nociceptive features.
Other drugs may be available for neuropathic pain after spinal cord injury. One trial with adequate evidence showed that the use of lithium carbonate did not change neurological outcomes but reduced neuropathic pain [55]. One SR on the systemic injection of analgesics showed that intravenous injections of 80 mg ketamine showed positive analgesic results for neuropathic conditions, but intravenous injections of lidocaine and mexiletine (an anti-arrhythmic medicine that is a non-selective voltagegated sodium channel blocker) were not more effective than placebo. Lidocaine exhibited significant analgesic effects on spontaneous pain for the first 45-minute post-injection; however, there was no difference when compared with placebo [4344]. One interesting RCT demonstrated the usefulness of nicotine in patients with spinal cord injuries [45]. Following nicotine exposure, non-smokers showed a reduction in mixed forms of pain; conversely, smokers showed an increase in both mixed and neuropathic forms of pain, indicating the need of smoking cessation counseling among smokers with a spinal cord injury [45]. However, the small population and the results in just one article need for attention to interpretation.
Another pharmacological drug option is opioids. One SR of high quality showed that short-term studies provided only equivocal evidence regarding the efficacy of opioids in reducing the intensity of neuropathic pain. Intermediate-term studies demonstrated significant efficacy of opioids over placebo, but these results were likely to be subject to significant bias because of the small size and short duration of the studies and their potentially inadequate handling of dropouts. The analgesic efficacy of opioids for chronic neuropathic pain was subject to considerable uncertainty. Adverse events related to opioids were commonly reported, but these were not life-threatening [46].
(2) Interventions
Two RCTs showed that low-frequency transcutaneous electrical nerve stimulation may effectively be used to complement pharmacological treatment in patients with spinal cord injury and neuropathic pain [4748]. However, a low number of participants and the lack of investigation of long-term effects could be constraints of these studies. One RCT and one SR showed that transcranial direct current stimulation exhibited a moderate effect in reducing neuropathic pain among individuals with spinal cord injury; however, this effect was not maintained at follow-up. Because of the limited number of studies and lack of follow-up, more evidence is required before treatment recommendations can be made [4950]. One RCT showed the effectiveness of 10 sessions of self-hypnosis training and EMG biofeedback relaxation training, suggesting that patients with neuropathic pain respond to hypnotic analgesia treatment alone; however, the improvement was not maintained at the 3-month follow-up [51]. One SR and one RCT investigated other interventions (transcranial magnetic stimulation, cranial electrotherapy stimulation, repetitive transcranial magnetic stimulation, exercise programs, acupuncture, and cognitive behavioral programs) and concluded that none of these techniques showed any benefit over the use of placebo [5253].
Discussion
This comprehensive literature review included RCTs and SRs of high (1++) or acceptable (1+) quality that considered treatments for neuropathic or chronic pain related to spinal disorders. Because all the reports were of high or acceptable quality, our levels of recommendation for treatment modalities about them were all graded A or B according to the grading system used [5]. Our search terms about spinal disorders causing neuropathic pain were divided into three categories: radiculopathy due to disc herniation, spinal stenosis, and spinal cord injury. However, the treatment modalities were not evenly distributed across these three spinal disorder categories in our search results, and we were unable to compare each treatment modality between the three spinal disorders. Nevertheless, this review provided evidence of a high quality and was specifically focused on the evidence regarding treatment for neuropathic pain caused by spinal disorders. Most treatment guidelines for neuropathic pain cover all of its various causes, including medical diseases (diabetic, infectious, etc.), peripheral neuropathic pain, and cancer. The natural history of neuropathic pain originating from these causes may differ from that of the pain originating from spinal disorders; thus, this review may be more specific for neuropathic pain of the spinal origin.
All the selected medications for radiculopathy were not commonly used and lacked evidence for their efficacy in managing neuropathic pain. This means that evidence supporting commonly used drugs for radiculopathy, including NSAIDs, anticonvulsants, antidepressants, and opioids, has not been demonstrated and effective medicines with much greater supportive evidence are not available until now. In case of spinal stenosis, one SR [29] reported that prostaglandin, gabapentin, and methylcobalamin (vitamin B12) showed some improvement in pain and functional outcomes, but each article was graded as providing low-quality or very low-quality evidence. However, even with only low-quality evidence, these could provide medical treatment options for spinal stenosis to improve pain and function. Patients with spinal cord injury commonly suffer from chronic neuropathic pain. This pain has been treated pharmacologically, but long-term medication could often be refractory and associated with adverse effects. In our review, most of the traditional anticonvulsant drugs showed no evidence of treatment efficacy in patients living with spinal cord injury [32333436]. One anticonvulsant, carbamazepine (at up to 600 mg/day), was able to reduce the incidence of neuropathic pain for up to 1 month; thus, early intervention for patients with spinal cord injury reduces their pain [36]. However, the benefits and risks of carbamazepine should be considered, especially with regard to its long-term use. Recently, gabapentinoids have increasingly been used and evidence of their effectiveness for neuropathic pain has been increasing. Two SRs [3738] with high-quality evidence demonstrated the effectiveness of gabapentin and pregabalin and showed that these were well-tolerated with fewer adverse effects compared with those of traditional anticonvulsants and could be used as first-line medication. Antidepressant drugs could also be a good option for treating neuropathic pain, but there was a lack of evidence regarding their effectiveness over that of a placebo. However, some drugs have shown some effects even when evidence is lacking; based on our results, amitriptyline [39] and venlafaxine XR [42] could be considered for use as part of multimodal medication to treat neuropathic pain in spinal cord injury. Another option for treating neuropathic pain after spinal cord injury is to use opioids and strong pain killers, especially for severe and chronic neuropathic pain. However, their long-term use is controversial owing to concerns about addiction and their effectiveness is not always consistent. One high-quality SR [46] found that intermediate-term (around 12 weeks) studies demonstrated significant efficacy of opioids over placebo. This evidence could be helpful in case of long-term users of opioids, and the adverse effects of their long-term use, such as abuse, addiction, hormonal abnormalities, and paradoxical hyperalgesia, should also be considered. Ketamine, an N-methyl-D-aspartate receptor antagonist, could also be an option for patients with intractable pain even proactive medicatin or opioid-induced hyperalgesia.
Among the three treatment modalities, interventions included nerve block procedures, physiotherapy, exercise, and electrical or magnetic stimulation. For radiculopathy, epidural block via transforaminal, interlaminar, and caudal routes showed generally positive results in the short and long term compared with the effects shown by placebo [15]. Several reviews concluded that the use of steroids in epidural injections showed no benefit over the use of local anesthetics alone [161720], although one RCT demonstrated that their use in epidural injections could have potential benefits pertaining to lumbar sciatica [20]. Regarding which steroids are better in epidural injections, the searched studies found no differences for cervical and lumbar radiculopathy [1823], but in 2014, the U.S. Food and Drug Administration warned of rare but serious neurologic problems after epidural corticosteroid injections for pain and especially the use of particle steroids. Radiofrequency treatment showed no superiority over placebo, but higher efficacy was achieved when it was used in conjunction with block procedures compared with that when block procedures were used alone [1423]; however, more evidence seems to be needed. Epidural block procedures for radiculopathy lacked evidence of their efficacy in patients with spinal stenosis, although one SR [29] cited a single trial with very low-quality evidence, which showed that interlaminar epidural steroid injections improved pain, function, and quality of life for up to 2 weeks. There is a lack of evidence for the efficacy of physiotherapy and exercise for radiculopathy or for the application of transcutaneous or transcranial electric and magnetic stimulation in patients with spinal cord injury [52].
The articles on surgery for neuropathic pain related to spinal disorders only covered radiculopathy and stenosis. Surgery, including decompression with or without fusion, resulted in better outcomes for radiculopathy than physical activity at short-term follow-up and significantly better outcomes for spinal stenosis and spondylolisthesis over a 2-year follow-up period [27]. Regarding radiculopathy, the main conclusion from these reviews was consistent with the observation that surgery appears to lead to short-term benefits for leg pain but no short-term effect on disease-specific functioning and similar outcomes can be seen in the long term [28]. None of the studies demonstrated benefits of endoscopic discectomy or alternatives including various intradiscal procedures, such as nucleoplasty, coblation nucleoplasty, and laser decompression [28]. There was insufficient evidence that surgery for spinal stenosis using interspinous devices was superior to other surgical interventions [28]. These findings suggest that surgery can be helpful for radiculopathy and spinal stenosis, especially in the short term. However, there was a lack of evidence demonstrating any long-term benefits.
Conclusions
In conclusion, this review, which included RCTs and SRs of high and adequate quality, found that some treatment modalities had variable efficacy. There was lack of evidence for the efficacy of pharmacological treatments for radiculopathy due to disc herniation and stenosis, but intervention procedures, including epidural block, showed positive efficacy for radiculopathy but only limited efficacy for spinal stenosis. There was some evidence that surgery was superior to conservative treatments for radiculopathy and stenosis at short-term follow-up, and limited evidence for pharmacological and electric or magnetic stimulation therapies for neuropathic pain after spinal cord injury. This review showed the relative paucity in the literature of high-quality evidence regarding the treatment of neuropathic pain related only to spinal disorders. Much greater supportive evidence is needed.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.