Introduction
There is a high prevalence of depressive symptoms in patients undergoing spinal surgery [12]. Up to 25% of patients undergoing lumbar fusion surgery use some form of antidepressant medication [3]. One potential complication of serotonergic antidepressants, however, is an increased risk of significant bleeding. Serotonin is known to enhance platelet activation, and serotonergic antidepressants have been demonstrated to deplete intracellular serotonin stores, thereby impairing platelet aggregation [45]. Meta-analyses have demonstrated an increase in perioperative bleeding and transfusion rates in general, plastic, and orthopedic surgery patients receiving these serotonergic medications [67]. Allogeneic blood transfusions have been associated with increased risk of sepsis, return to operating room, surgical site infection, pulmonary embolism, as well as increased length of stay in lumbar fusion surgery [8]. A previous study on the estimated blood loss in spine surgery reported a 23% increase in blood loss associated with serotonergic antidepressants [9]. This study did not control for other risk factors, such as preoperative hematocrit or report on transfusion rates. The purpose of our study was to examine the impact of serotonergic antidepressant therapy on (1) blood loss and (2) transfusion requirements in a homogenous population undergoing posterior lumbar interbody fusion. This study uses surgical data from a single center to construct multivariate regression models to answer these questions.
Materials and Methods
1. Study design
After institutional review board approval was obtained, adult patients who underwent single level fusion surgery of the lumbar spine (posterior lumbar interbody fusion in combination with posterior instrumented fusion), were identified retrospectively through a query of Current Procedural Terminology codes. The surgeries were performed by five senior fellowship-trained surgeons at a tertiary spine center between January 2008 and December 2013. All patients were operated on a Maquet table with four poster bolsters and free abdomen in a prone position. The indications included degenerative disc disease, spinal and foraminal stenosis and degenerative spondylolisthesis. Patients taking serotonergic antidepressants (cases) were compared to patients who were not taking serotonergic antidepressants and undergoing the same procedure in the same time period (control group).
Exclusion criteria were: history of previous spinal fusion, hematologic disease, hepatic disease, history of deep venous thrombosis or pulmonary embolism, autoimmune disease, and an Amercian Society of Anesthesiologists Physical Status Classification (ASA) score of greater than 2. Furthermore, all patients taking potentially confounding medications, specifically aspirin, antiplatelet and anticoagulant agents, within a month prior to surgery were excluded to eliminate confounding. At our institution, all patients are instructed to hold non-steroidal anti-inflammatory drug (NSAID) therapy 7 days prior to surgery. Patients who held the aforementioned agents for 7 days, were included in the study. Finally, patients with missing medical records were excluded.
The data was collected and analyzed by an independent observer not involved in patient care. Patient charts, operative notes and anesthesia records were reviewed retrospectively. The following data was collected: demographics, comorbidities, medication status, perioperative blood tests, surgical details and transfusion status.
Blood loss was routinely estimated by the anesthesiologist based on the count of sponges used, the amount of blood reinfused via use of a cell salvage apparatus, and consensus of surgeon and anesthetist. The intraoperative use of cell salvage systems is standard of care at our institution for posterior lumbar fusion procedures.
Information on the regular use of medication was collected from pre-surgical screening notes. While the exact duration of medication intake could not be ascertained, all patients were on regular medication therapy for a minimum of one week. For this study we categorized antidepressants based on their inhibitory properties [10]: selective serotonin reuptake inhibitors (SSRI; fluoxetine, paroxetine, sertraline, escitalopram, citalopram, fluvoxamine), serotonin-norepinephrine reuptake inhibitors (SNRI; duloxetine, venlafaxine, milnacipran), serotonin receptor antagonists (nefazodone, trazodone), and tricyclic and other antidepressants.
2. Transfusion guidelines
Restrictive transfusion guidelines have been published by a variety of professional organizations [11], and are part of standard care at our institution. At our institution, we use multidisciplinary-derived guidelines and the final decision is based on a consensus between the medical and surgical team involved in the patient's care. Our guidelines suggest transfusion in the following cases: (1) active bleeding in a clinically unstable patient; (2) hemoglobin level below 8 g/dL, that is not due to iron, folate or vitamin B12 deficiency; and (3) hemoglobin level below 10 g/dL and one of the following: (1) coexisting cardiac, pulmonary or cerebrovascular disease, (2) symptoms of low oxygen delivery to peripheral tissues, or (3) patients on chronic transfusion regimens.
3. Statistical analysis
The dependent variables examined in statistical analysis were blood loss and allogeneic blood transfusion. The statistical analysis was performed using the statistical software R (ver. 3.2.3, R Foundation for Statistical Computing, Vienna, Austria) [12]. A p-value of less than 0.05 was used to indicate statistical significance. Continuous variables are expressed as mean┬▒standard deviation and categorical variables as counts and percentages. Bivariate associations between variables were assessed with the chisquare or Fisher exact test and t test or Mann-Whitney U test, as applicable, while correlations were assessed with the Kendall rank correlation coefficient.
A linear regression model was developed for the logtransformed variable estimated blood loss with the purpose to examine the effect of SSRIs. In order to account for known confounding factors [1314], the linear regression model was adjusted for age, gender, body mass index, operative time, preoperative hematocrit and platelet count. Observations with missing variables were excluded from analys.
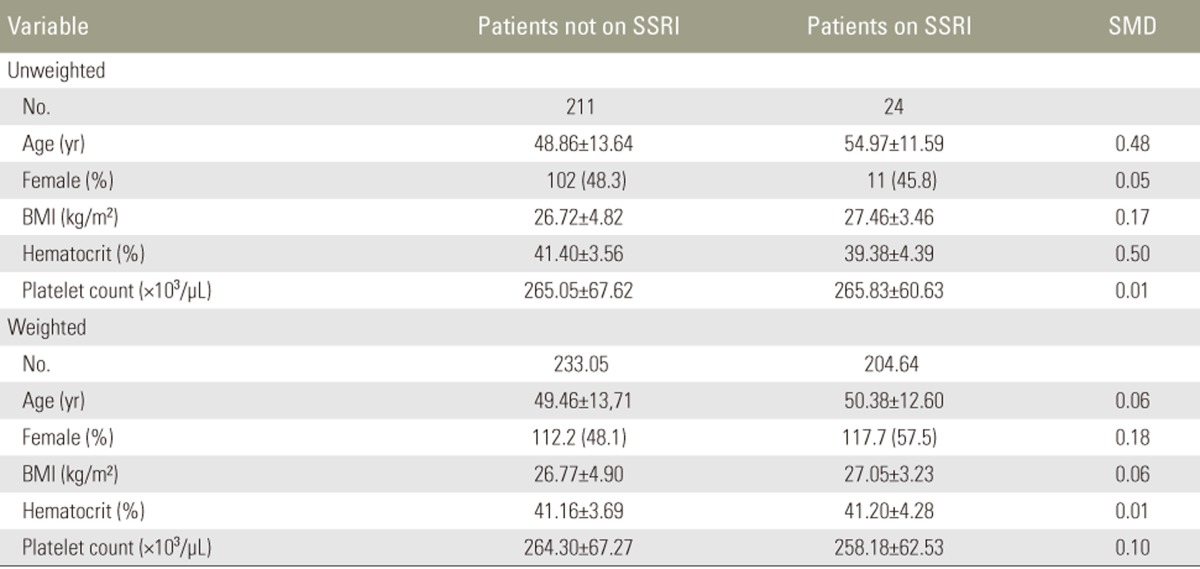
Weighted logistic regression models were developed for the outcome variable allogeneic blood transfusion. Antidepressant treatment in this patient population was not assigned randomly. In order to account for this selection bias and the confounding effects of known risk factors, propensity score analysis was performed. Propensity scores for the intake of SSRI were calculated using logistic regression analysis based on risk factors for the outcome variable allogeneic transfusion, including the following variables: age, gender, body mass index and preoperative hematocrit [815]. Inverse probability weights for the average treatment effect, defined as 1/propensity score for patients on SSRI and 1/(1ŌĆōpropensity score) for the control group, were calculated. Weights were trimmed at the 99th percentile. Balance of propensity score weighting was assessed by calculating the standardized mean difference. A value equal to or below 0.1 was used to indicate appropriate balance [15]. Variables that were found to be imbalanced were included in the final weighted logistic model to adjust for any residual confounding effects. Logistic regression analysis for the outcome variable allogeneic blood transfusion was then weighted using these inverse probability weights [15].
Results
1. Demographics
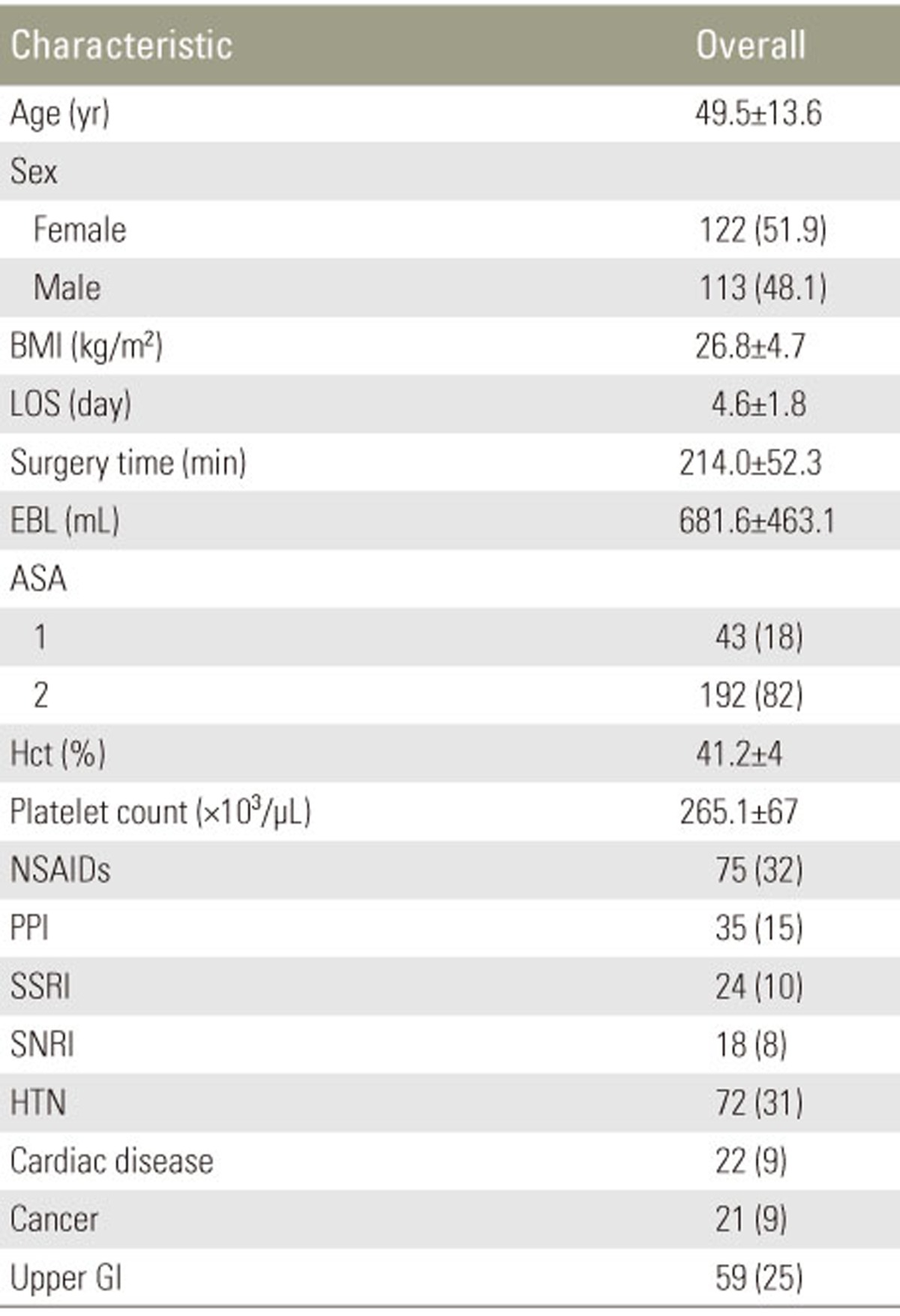
A total of 374 patients were identified of which 116 patients were excluded due to comorbidities, medication use, or based on ASA score, and 23 due to missing medical charts. Finally, 235 patients were included in the study. Of these patients, 122 (52%) were female. The mean age was 49┬▒14 years and the mean body mass index 27┬▒5 kg/m2. Review of operative charts showed a mean preoperative hematocrit of 41┬▒4%, a mean platelet count of 265,000┬▒67,000/┬ĄL, and an average surgery time of 214┬▒52 minutes. The mean blood loss was 682┬▒463 mL. The mean length of stay was 5┬▒2 days. NSAIDs were taken until one week before surgery by 75 (32%), proton pump inhibitors were prescribed in 35 (15%), SSRI in 24 (10%), SNRI in 18 (8%), serotonin receptor antagonists in 6 (3%) patients, and other antidepressants were taken by 13 (6%) patients (Table 1). Only SSRI and SNRI use were examined in further analysis, because of the low numbers in the other antidepressant groups.
2. Antidepressants and estimated blood loss
Bivariate analysis showed a significant association between estimated blood loss and gender (male: 821 mL vs. 552 mL, p<0.001), body mass index (Žä=0.229, p<0.001), surgery time (Žä=0.250, p<0.001), preoperative hematocrit (Žä=0.130, p=0.004), preoperative platelet count (Žä=ŌĆō0.118, p=0.010), history of hypertension (792 mL vs. 632 mL, p=0.024) and intake of SSRI (857 mL vs. 661 mL, p=0.014). SNRI (497 mL vs. 697 mL, p=0.065) were not found to be significantly associated with estimated blood loss. Applying restrictive variable selection criteria, SNRI were not included in multivariate regression analysis.
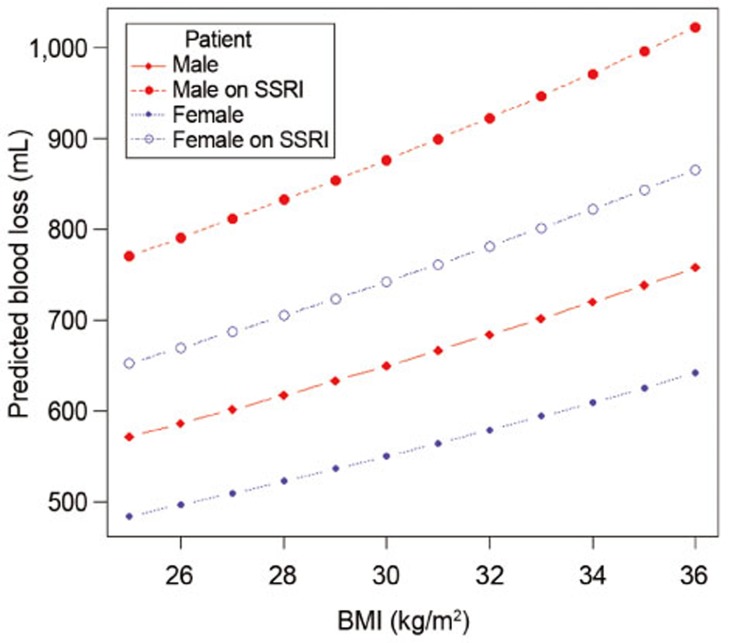
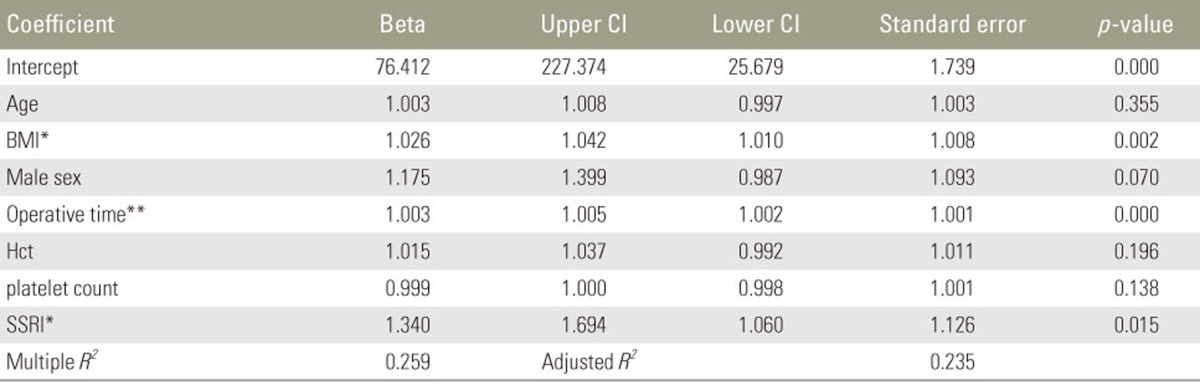
Linear regression analysis showed that body mass index (average of 2.6% increase per unit body mass index, b=1.026, p=0.002), surgery time (average of 0.3% increase per minute operative time, b=1.003, p<0.001) and intake of SSRI (average of 34% increase, b=1.340, p=0.015) were significant predictors for blood loss (Table 2). A total of 7 observations were not included in linear regression due to missing variables. Fig. 1 shows the effect of SSRI on predicted blood loss based on linear regression analysis
3. Antidepressants and blood transfusion
Bivariate analysis showed a significant association between blood transfusion and age (56 years vs. 48 years, p=0.030), preoperative hematocrit (38% vs. 41%, p=0.001), intake of SSRI (p<0.001), and disease of the upper gastrointestinal tract (p=0.016). Serotonin norepinephrine reuptake inhibitors (p=0.375) and the use of cell salvage apparatus (p=1.000) were not found to be significantly associated with transfusion, and were dropped from further analysis (Table 3).
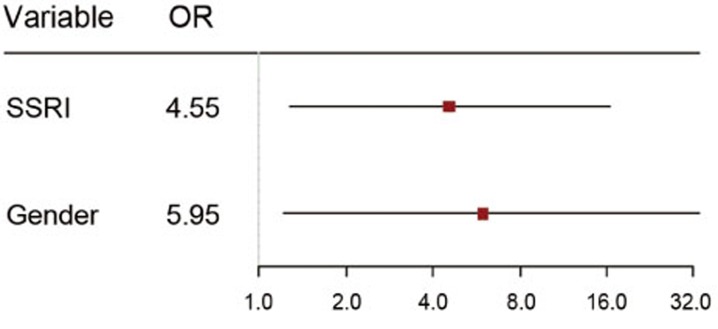
Logistic regression with inverse probability for treatment weighting was performed. Balance diagnostics showed that the covariate gender was imbalanced and thus it was adjusted for in the final logistic model (Table 4). Female gender (odds ratio [OR], 5.952; p=0.029) and intake of SSRI (OR, 4.550; p=0.029) were found to be significant predictors for blood transfusion. A total of 2 controls were excluded due to missing values (Table 5, Fig. 2).
Discussion
The results presented in this study suggest that intake of SSRI is a risk factor for increased blood loss and allogeneic transfusion in patients undergoing single-level posterior lumbar interbody fusion. Multivariate analysis showed a statistically significant association of serotonergic antidepressants, blood loss, and risk of allogeneic transfusion. Intake of SSRI was found to significantly increase blood loss and increase the risk for allogeneic blood transfusion.
1. Antidepressants and estimated blood loss
Our findings regarding blood loss are supported by several reports in the literature. The estimated blood loss of 682 mL observed in this study is comparable to 521 mL [16] in single-level posterior lumbar interbody fusion, reported previously.
Patients on serotonergic antidepressants were found to have an increased blood loss when undergoing general, orthopedic and plastic surgery in several different studies [671718]. In patients undergoing percutaneous endoscopic gastrostomy, intake of SSRI increased the risk of post-procedural bleeding 4-fold, while aspirin and clopidogrel did not [18]. A study of hip arthroplasty patients demonstrated that patients on serotonergic antidepressants had a 17% increase in blood loss [17]. Patients undergoing elective orthopedic surgery had a 75% increase in blood loss associated with antidepressant use [19]. In a study on patients undergoing spinal surgery, serotonergic antidepressants caused an increase of 23% in blood loss, as well as an increase of over 200 mL in posterior lumbar fusion specifically [9]. This study, however, did not control for the confounding effects of factors such as gender or age. Similar findings have been reported in a meta-analysis indicating that serotonergic antidepressants might increase the risk of perioperative bleeding (OR, 1.21 to 4.14) [6]. In accordance with these findings, our analysis indicates that intake of SSRI is associated with a 34% increase in blood loss (b=1.340, p=0.015). The differences in effect size can be explained by variations in study design. Similar to other studies [7171819], our results indicate that only serotonergic antidepressants with high affinity for serotonin reuptake transporters, such as SSRI, can have an effect on platelet action. Other antidepressants, such as SNRI with low affinity for serotonin transporters, did not show this effect in our study, nor other studies [7171819].
Body mass index is a known risk factor for significant intraoperative bleeding in spinal surgery. In patients undergoing lumbar fusion surgery, higher body mass index can increase the risk of significant blood loss [13], with blood loss doubled in obese patients (440 mL vs. 798 mL) [20]. Similarly, in our study an increase of 1 unit in body mass index resulted in a 2.6% increase in blood loss.
Lastly, surgery time has been demonstrated to be a significant predictor of blood loss in patients undergoing instrumented lumbar fusion previously [1321]. Accordingly, we found an 18% increase in blood loss for every additional hour spent in the operating room. The causal relationship of this finding is unclear and it is unknown whether this is related to the tendency for higher blood loss to slow the progression of surgery, or whether this reflects a standard blood loss per hour extrapolated over a longer period of time.
2. Antidepressants and blood transfusion
Many risk factors for the requirement of blood transfusions in spinal surgery have been established [8]. In addition to these factors, studies in cardiac and non-cardiac surgery have reported an increased risk for blood transfusion in patients on serotonergic antidepressants [1922]. These studies reported an odds ratio of 2.24 and 3.71 to be exposed to allogeneic transfusion when taking serotonergic antidepressants. Studies on antidepressant use and transfusion rates in coronary artery bypass surgery specifically, however, found no increase in transfusion rates [2324]. These findings are reflected in a recent meta-analysis, showing that with the exception of cardiac surgery, serotonergic antidepressants increase the risk for blood transfusion (OR, 1.19) [7]. Similarly, our results indicate that intake of SSRI increased the odds ratio to require an allogeneic transfusion by more than 4-fold (OR, 4.5). Female gender was also found to be a significant preoperative predictor for transfusion in our study (OR, 6.0). This is also supported by previous studies in spinal surgery indicating a higher odds ratio for females to require perioperative blood transfusion compared to males [81425]. The etiology of this observation is not well understood. It is important to note, however, that females in general have lower baseline hematocrit measurements, and most transfusion guidelines, including our own, do not factor in gender when defining transfusion cutoffs. The differences in effect size can be explained by the study design.
3. Potential explanations for the effect of antidepressants on blood loss and transfusion
Several explanations for SSRI-associated abnormal bleeding are currently being evaluated, but the exact biochemical mechanism is yet to be elucidated. One hypothesis suggests that SSRI-induced inhibition of serotonin reuptake in platelets results in a reduced serotonin-triggered platelet aggregation and vasoconstriction [4526]. Other factors, such as inhibition of thrombin induced platelet activation might play a role as well [27]. This hypothesis is supported by studies suggesting that SSRIs exert cardioprotective effects in patients with depression after myocardial infarction. In this patient population, intake of SSRIs was found to reduce morbidity and mortality due to inhibition of platelet activation [2829]. In patients undergoing surgery, prolonged bleeding due to SSRI intake has been found to increase blood loss and transfusion rates [1922].
4. Limitations
There are a few limitations to this study: (1) this study was conducted as a retrospective case-control study and data was collected from a chart review. (2) Only a small number of transfusions were observed. In order to overcome the limitations of logistic regression with a small number of cases, propensity score weighting was applied. Recent papers suggest that even as few as 5 cases per variable can be acceptable for logistic regression [30]. (3) This study does not control for other potential confounding factors, such as autologous blood donation and transfusion, smoking status and supplemental or herbal therapy. (4) Furthermore, this study does not control for the use of cell salvage systems, as it was not found to be associated with transfusion rate in bivariate analysis, or intraoperative blood pressure. This study did control for important risk factors of blood loss and transfusion, reported previously, by excluding patients with relevant disorders and adjusting and weighting in regression models. (5) Patients were treated by five different surgeons. Differences in surgical technique, however, are unlikely as all single-level posterior lumbar interbody fusion surgeries in this study were performed by senior, fellowship-trained surgeons. (6) Estimation of intraoperative blood loss by an experienced anesthesiologist, a common approach to measuring intraoperative blood loss, might under- or overestimate blood loss. In order to minimize this effect, estimates in this study were based on sponge count, blood reinfused and consensus of surgeon and anesthetist. (7) All patients were on regular medication therapy for a minimum of one week. A previous study indicated that paroxetine can exert its inhibitory effect on platelet function within a period as short as 2 weeks [4]. Finally, conclusions from this study are supported by a strong agreement of linear regression on blood loss and logistic regression on transfusion requirement.
Conclusions
The intake of SSRI is a risk factor for increased blood loss and allogeneic blood transfusion in adults undergoing single level posterior lumbar interbody fusion. Ongoing research is required before any recommendations regarding changes in drug therapy or precautions, such as autologous blood transfusion, can be made. Nonetheless surgeons and perioperative medical providers should take these findings into account when assessing a patient's risk for transfusion preoperatively.