Introduction
The apex of the odontoid process develops from a separate ossification center, the ossiculum terminale, which usually appears by three to six years of age and continues to enlarge, fusing with the body of the odontoid process by 12 years of age [1]. These synchondroses are potential weak regions that are susceptible to traumatic disruption. The neurocentral synchondrosis between the dens and the body of C2 ossifies around age seven and represents a site vulnerable to injury in young children [23]. Because this injury occurs at the epiphysis, it is usually amenable to halo immobilization for a period of at least ten weeks [45]. Internal fixation and fusion should be reserved for the 20% of cases of pediatric odontoid fractures that do not fuse with external immobilization, and surgical procedures for atlantoaxial (C1–C2) fusion in children are relatively uncommon. We report on a case of atlantoaxial instability caused by os-odontoideum in association with quadriparesis and respiratory paralysis in a five-year-old girl. The instability was treated by halo immobilization, followed by C1–C2 transarticular screw fixation using a computed tomography (CT)-based navigation system.
Case Report
Informed consent was obtained from the parents of the patient. The patient was a 5-year-old girl with no history of Down Syndrome or systemic bone disease. One week before her hospital visit, she was playing with her elder sister and holding hands, and they had fallen together. After the incident, she started to complain of neck pain and her extremities gradually started to lose strength. From one day before admission at an affiliated hospital, she was unable to rise on her own and using food chopsticks that fell from her right hand. She visited the emergency unit of an affiliated hospital, and a severe paralysis of right side of body was observed.
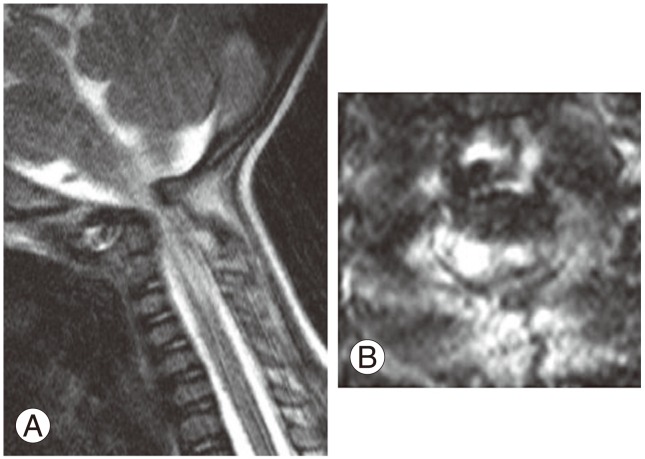
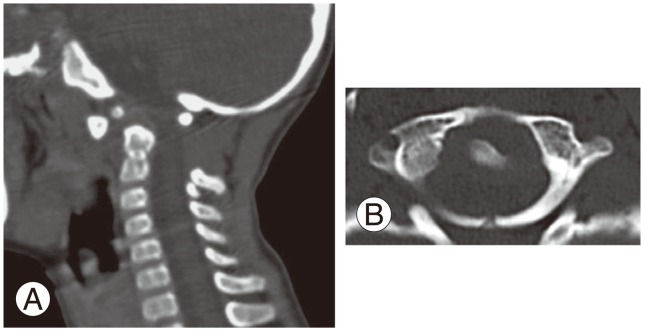
When performing a magnetic resonance imaging (Fig. 1), the patient became drowsy. Percutaneous oxygen saturation had decreased to 60%–70%, judged to be due to respiratory dysfunction caused by respiratory paralysis. She was intubated to start artificial respiration control and was admitted to the intensive care unit. Plane radiographs and CT images (Fig. 2) revealed atlantoaxial instability caused by odontoid epiphysiolysis, and the atlantoaxial spine could be repositioned only in the maximum extension position. Manual muscle test of right upper/lower extremity and left upper/lower extremity were 1–2 and 3–4, respectively. The patient was introduced and admitted to our hospital on day 8 of disease occurrence.
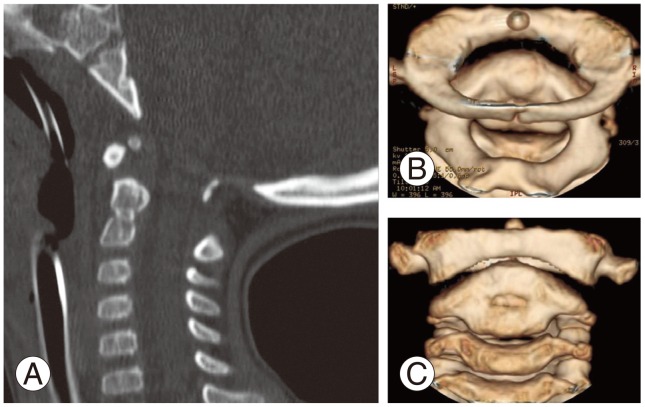
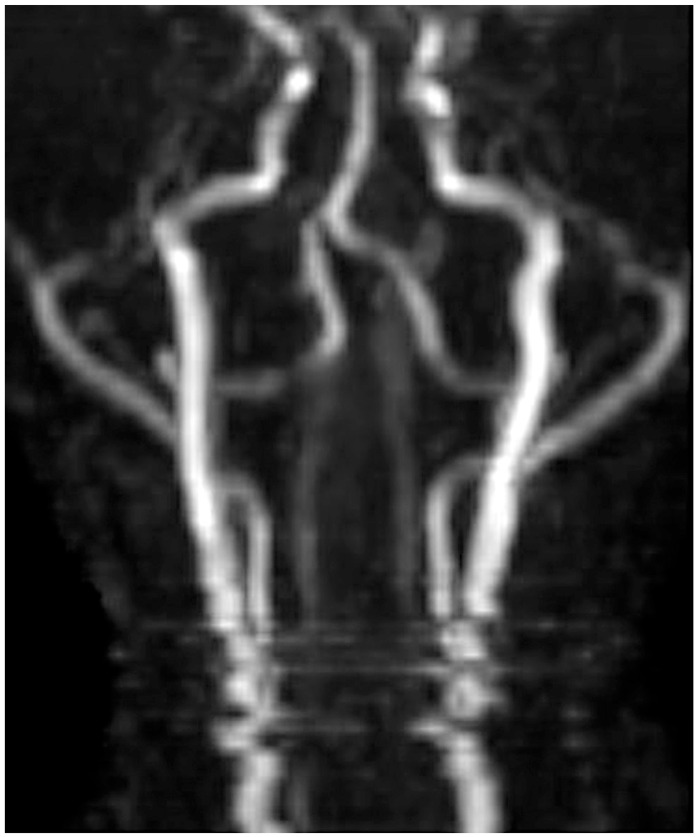
At day 9 of the occurrence, the patient was fitted with a halo vest under general anesthesia and the patient was placed in supine position with a pillow for head support; a special neckband was fitted around the neck (at the lordosis, to apply pressure to the C2 spinous process), and then reduction of atlantoaxial subluxation was performed (Fig. 3). Subsequent MR angiography confirmed that the bilateral vertebral arteries were normal (Fig. 4). At day 13 of the disease, Magerl's procedure [6] was performed with 3.0 mm cannulated screws (Synthes, West Chester, PA, USA) under a CT-based navigation system. The reference frame was placed on the C3 spinous process and the camera was placed on the cranial side. In accordance with multilevel registration procedure described by Takahashi et al. [7], registration was performed at C2 and C3. We performed registration at the following seven points: the bilateral tips of the C2 spinous process, the bilateral tips of the C2 inferior facet, a tip of the C3 spinous process, and the bilateral tips of the C3 inferior facet. The mean registration errors after point and surface registration were 5.8 mm and 0.7 mm, respectively. C1 and C2 vertebral arches were decorticated and bone graft collected from ileum were processed to tip shape and transplanted as onlay between C1 and C2 (Fig. 5).
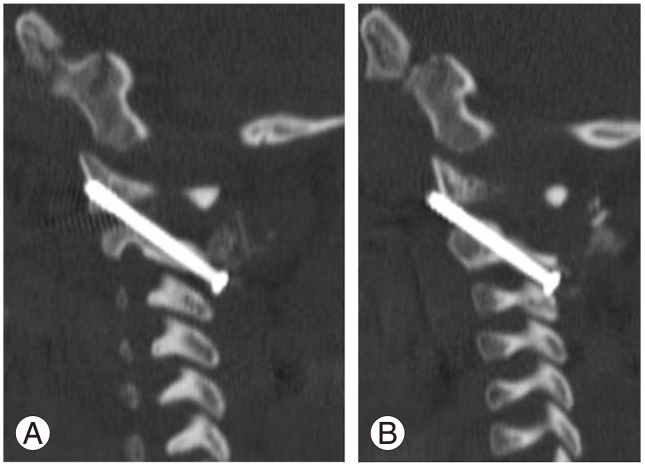
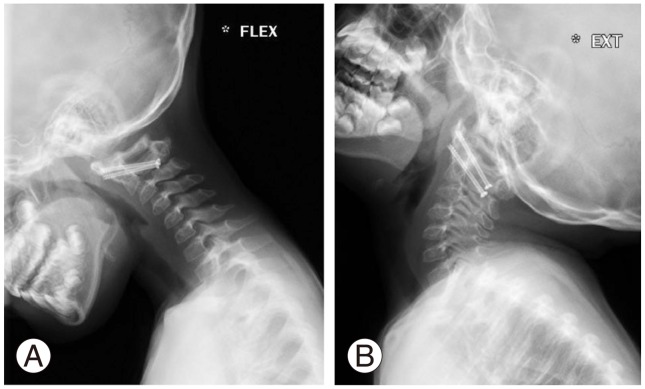
Halo vest was removed after surgery and neck collar was fixed. A day after surgery, the patient could bend both knees and fold right palm. Recovery from the quadriplegia and respiratory paralysis gradually occurred. CT image 1 week after surgery revealed that right transarticular screw was inserted to lower anterior position of anterior arch of atlas, but left screw was accurately inserted (Fig. 6). Spontaneous respiration was gradually started after surgery and the patient was extubated at post-surgery day 10. Oral food intake was started at day 19 post-surgery, and at day 25, maintaining sitting and standing positions with support became possible. At day 30 after surgery, the patient was moved to our affiliated hospital. Neck collar was completely removed at 6 months after surgery because bony union was achieved, judged by sagittal reconstruction CT and dynamic lateral radiography. Currently, at five years after surgery, neurological symptoms have almost fully recovered and the child is attending an elementary school. Dynamic lateral radiography showed no instability (Fig. 7), and sagittal and coronal reconstruction CT showed complete C1–2 bone union (Fig. 8).
Discussion
Considering the development of the second cervical vertebra, displacement of the ossiculum terminale may occur at an age when the apical odontoid epiphysis and os odontoideum remain unfused, and the synchondrosis between the odontoid process and the body of the axis has already closed [8]. A displaced ossiculum terminale should be kept in mind when evaluating a child younger than twelve years of age who has sustained a cervical injury.
Only four reports of transarticular screw fixation performed in children at 5 years of age or younger were found [9101112]. This was in a search of case series with the condition that the youngest subject was 5-years-old or less. Rekate et al. [13] have stated that the youngest appropriate age for C1–C2 transarticular screw fixation should be 4 or 5 years of age, and Haque et al. [14] performed screw fixation of the upper cervical spine in five subjects aged 5 years, or less but they employed C1 lateral mass screws and C2 pars screws. On the other hand, Gluf and Brockmeyer [10] safely placed 24 C1–C2 transarticular screws in 13 patients 4 years of age or younger (19% of their overall series), providing sufficient evidence that transarticular atlantoaxial screw fixation is safe and effective in this very young age group.
Transarticular screw, which penetrates the cortex three times, should be biomechanically robust compared to C1 lateral mass and C2 pars screw, which is technically simpler. We believe transarticular screw to be superior when the navigation plan suggests a feasible trajectory for screw insertion. In this case, postoperative use of a halo vest was not necessary to achieve bony union; however, C1 lateral mass and C2 pars screws require the use of a halo vest in most cases.
The management of upper cervical spinal instability in children continues to represent a technical challenge. Traditionally, a number of wiring techniques followed by halo orthosis have been applied; however, they have been associated with a high rate of nonunion and poor tolerance for the halo. Alternatively, C1–C2 transarticular screws and C2 pars/pedicle screws allow a more rigid fixation, but they are technically demanding and are associated with vertebral artery injuries. Thus, we employed a CT-based navigation system for planning and actual insertion of transarticular screws. Stulik et al. [9] reported a case of a 4-year-old girl who underwent Magerl fixation of C1–C2 with 2.7 mm titanium screws (Synthes), and Gluf and Brockmeyer [10] reported that they generally employ 3.5 mm screws to children 4 years of age or younger. We also judged that screws 3 mm in diameter could be inserted with halo vest and CT-based navigation. Stability was achieved and neurological symptoms were dramatically improved.
In conclusion, the authors report a case of atlantoaxial instability caused by os-odontoideum in association with quadriplegia and respiratory paralysis in a five-year-old girl. The instability was treated by halo immobilization, followed by C1–C2 transarticular screw fixation using a CT-based navigation system. At five years follow-up, the patient has made a complete recovery with solid union.