Introduction
Anterior lumbar fusion surgery (ALF) for the lumbar spine has a high rate of success, although intraoperative concerns and iatrogenic complications exist [123]. Injuries to major vessels or branches of segmental arteries from the aorta are sometimes a complication, and it may be difficult to stop such bleeding. A wide range of local internal hemostatic agents has been developed to help achieve intracavity control of bleeding [4].
TachoSil (Nycomed, Linz, Austria) was developed from TachoComb (Nycomed) and TachoComb H (Nycomed) [45]. TachoComb contains equine collagen, bovine thrombin, bovine aprotinin, and human fibrinogen [5]. TachoComb H is made human thrombin in place of bovine thrombin [5]. TachoSil, in turn, contains only human fibrinogen with equine collagen as a carrier [5], and it does not contain aprotinin or any other components of bovine origin [5].
Efficacy of TachoSil for several types of surgery has been reported; however, use of TachoSil for ALF surgery has not been described [6]. We report on the efficacy of TachoSil used in 6 patients who underwent ALF and the vascular surgeons were trying to repair difficult vessels.
Materials and Methods
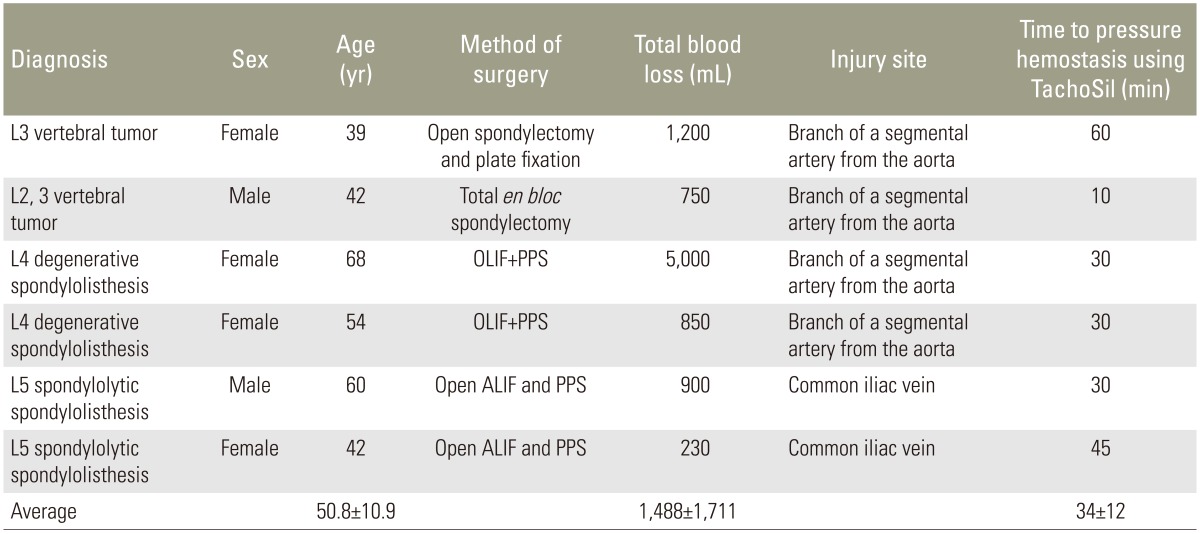
We performed 496 surgeries on the lumbar spine from April of 2012 to December of 2015 in our medical center. ALF was performed in 184 patients. Among these, 12 patients had injury to blood vessels that included the common iliac vein or a segmental artery. Vascular injury of 6 of these 12 patients (50%) could not be repaired by conventional techniques. Written informed consent was received from these 6 patients for their case reports to be published. Two man and 4 women underwent ALF as the conservative treatment was ineffective. The patients had an average age of 50.8±10.9 years (mean±standard deviation [SD]) and were diagnosed with a vertebral tumor (2 patients), L4 degenerative spondylolisthesis (2 patients), and L5 spondylolytic spondylolisthesis (2 patients) (Table 1). For L5 spondylolytic spondylolisthesis, open ALF surgery using percutaneous pedicle screws (PPS) was conducted. For L4 degenerative spondylolisthesis, mini-open anterior retroperitoneal lumbar interbody fusion methods, such as oblique lumbar interbody fusion (OLIF) [78] using PPS, were performed. For L2 and L3 vertebral tumor, L2 and L3 total en bloc spondylectomy was carried out, and for L3 vertebral tumor, open total vertebral resection with plate fixation was implemented.
The blood vessels injured included the common iliac vein in 2 patients and a branch of a segmental artery from the aorta in 4 patients. We consulted a vascular surgeon to suture or repair the vessels during surgery, and although the vascular surgeon attempted to suture or repair the injury, suturing or repair was not possible. For this reason, we used TachoSil to repair the injury to the wall of vessels or to stop the bleeding. There were no guidelines about the appropriate time to pressure hemostasis for spine surgery. Therefore, the time to pressure hemostasis using TachoSil was determined by each surgeon. We evaluated the time to pressure hemostasis using TachoSil, the total blood loss, and whether vessel injuries were controlled by using TachoSil. We confirmed hemostasis in the surgical field during surgery, and inserted a suction drain at the end of surgery. We also evaluated bleeding into the suction drain for 2 days after surgery. However, we did not evaluate hemostasis using additional radiological examinations after surgery.
Results
Time to pressure hemostasis using TachoSil was from 10 to 60 minutes, with average time of 34±12 minutes (mean±SD). Total blood loss was from 230 to 5,000 mL, with average blood loss of 1,488±1,711 (mean±SD) (Table 1). Fortunately, all vessel injuries were successfully controlled by using TachoSil. We did not observe bleeding after the surgery, did not find excess bleeding into the suction drain during the 2 days after surgery in 6 patients, and all patients recovered normally.
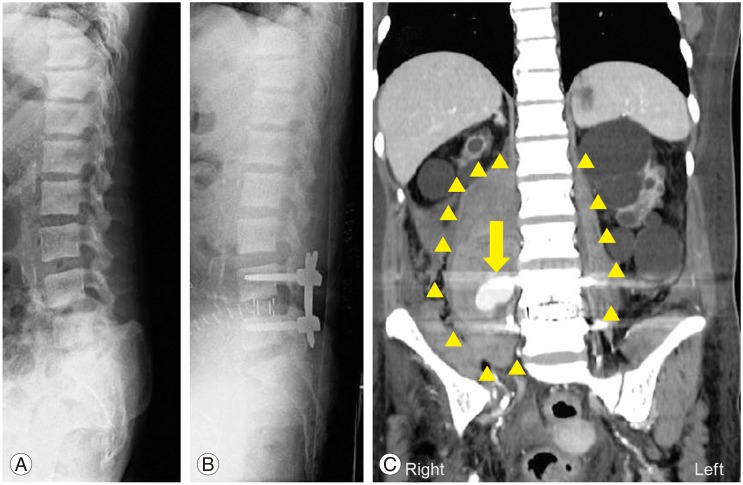
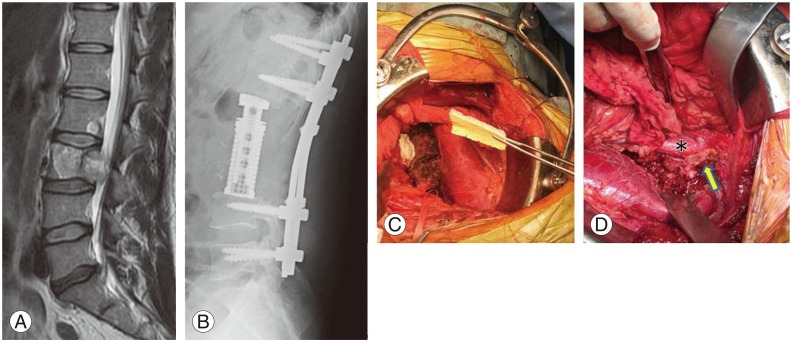
Fig. 1 shows the injury to the branch of the segmental artery from the aorta on the contralateral side after OLIF plus PPS surgery. We reoperated from the contralateral side, and were ultimately able stop the bleeding using TachoSil. Fig. 2 shows the injury to the branch of the segmental artery from the aorta during L2 and L3 total en bloc spondylectomy for the L2 and L3 vertebral tumor, and could stop the bleeding using TachoSil.
Discussion
In the current study, we present injury to the common iliac vein in 2 patients and a branch of a segmental artery from the aorta in 4 patients. All vessel injuries were controlled using TachoSil where a vascular surgeon could not suture or otherwise repair the vessel. From our experience, we recommend the use of TachoSil for such cases.
A systematic review and meta-analysis were used to assess the clinical and radiographic outcomes and complications of ALF versus TLIF. Fusion rates and clinical outcomes were comparable between ALF and TLIF. However, major blood vessel injury occurred significantly more frequently in the studied ALF cohort compared with the TLIF cohort (2.6% vs. 0%) [9]. This outcome was not surprising, given that the anterior technique involves exposure, manipulation, and mobilization of the iliac vessels, and increases the risk of bleeding via lacerations and thrombosis [1011]. Vascular surgeons may help to approach or repair the vessel injuries; however, suturing sometimes fails.
Until now hemostatics, used most commonly in spine surgery, have included oxidized, regenerated cellulose (Surgicel), gel sponges (Gelfoam, Spongostan), and collagen fleece (Avitene) [12]. Local hemostatics should be removed at the end of the surgery, but these materials are absorbable and so they are often left in place to avoid postoperative hematomas. Another hemostatic, bone wax which is a mixture of beeswax (70%) and Vaseline (30%) is not absorbable [12]. Recently, FloSeal (Baxter Healthcare, Deerfield, IL, USA) and Surgiflo (Ethicon, Somerville, NJ, USA), have been developed for bleeding control during spine surgery [13]. However, these agents are used for bleeding from the surgical field, and are not useful for vessel injuries during anterior lumbar spine surgery.
The efficacy and safety of TachoSil in patients with lung bleeding problems, liver resection, and splenectomy have been demonstrated, and there are also a few articles related to use of TachoSil in cardiovascular surgery [141516]. Excessive bleeding represents a significant risk for the patient in cardiovascular surgery. The safety and efficacy of TachoSil compared to conventional techniques to stop bleeding were examined [17]. In the study, 20 patients underwent TachoSil treatment and 22 patients received a conventional treatment using Surgicel (Ethicon, Johnson & Johnson Medical, Neuchatel, Switzerland) [17]. In the TachoSil treated group, 75% of patients required transfusions versus 90% in the Surgicel treated group [17]. The investigators concluded that TachoSil might act as a superior alternative in various types of cardiac surgery to control bleeding and thereby reduce transfusion requirements [17]. To our knowledge, the efficacy of TachoSil for vessel injuries during anterior lumbar spine surgery has not been reported until now.
TachoSil is used for incidental durotomy, a common complication of lumbar spine surgery, with a prevalence ranging from less than 1% to 17%, according to the series reviewed and the type of surgical procedure [1819]. In March 2014, members of the Swiss, German, and Austrian neurosurgical and spine societies were asked to complete an online questionnaire regarding the management of incidental durotomy during and after lumbar spine surgery, and TachoSil/Spongostan with fibrin glue or a similar product (79.4%) and single suture repair (69.7%) were the treatments preferred by most surgeons [20]. In addition to repair incidental durotomy, we recommend the use of TachoSil for vessel injuries that vascular surgeons cannot suture or otherwise repair during ALF surgery.