Introduction
Transforaminal lumbar interbody fusion (TLIF) is one of the most common procedures for treating lumbar spinal pathologies such as spondylolisthesis and spondylolysis. Between 2001 and 2010, TLIF and posterior lumbar interbody fusion (PLIF) accounted for 79%–86% of all lumbar interbody fusions, and TLIF and PLIF are increasingly performed annually [1-4]. Although these procedures are generally well tolerated, the hospital cost per procedure has steadily increased, averaging more than US $50,000 per admission in 2015 [1,3].
The postoperative length of stay (LOS) is an indicator of patient comorbidities, case complexity, and perioperative complications [5-7]. Extended LOS increases costs for both patients and hospital systems [5]. Previous studies have shown increased LOS in cases associated with morbid obesity, advanced age, higher American Society of Anesthesiologists (ASA) classification, longer operative times, and perioperative blood transfusions [6-9]. However, these studies have focused on different procedures or include only specific approaches [5,8].
Although single-level TLIF may be appropriate for the outpatient setting, few studies have examined factors that prevent patients from leaving on the day of or after surgery. Analysis of these factors may aid in selecting patients who are suitable candidates for the outpatient setting, thereby reducing costs and decreasing potential complications. In this study, the national multicenter American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was used to examine the perioperative factors, complications, and readmissions associated with LOS ≤1 day in patients undergoing single-level TLIF.
Materials and Methods
Data source
Data were collected from the ACS-NSQIP dataset from 2011 to 2018. The ACS-NSQIP database is a random sample of surgical patient demographic information, perioperative parameters, and adverse events data from over 700 hospitals worldwide. The ACS-NSQIP dataset contains prospectively collected data that are audited for interobserver agreeability, as opposed to several administrative databases commonly used for neurosurgical research [10]. Because the data are de-identified and publicly available, this study is not considered a human subject research by the institutional review board at our institution; thus, it is exempt from review, and patient consent was not sought.
Inclusion and exclusion criteria for cohort selection
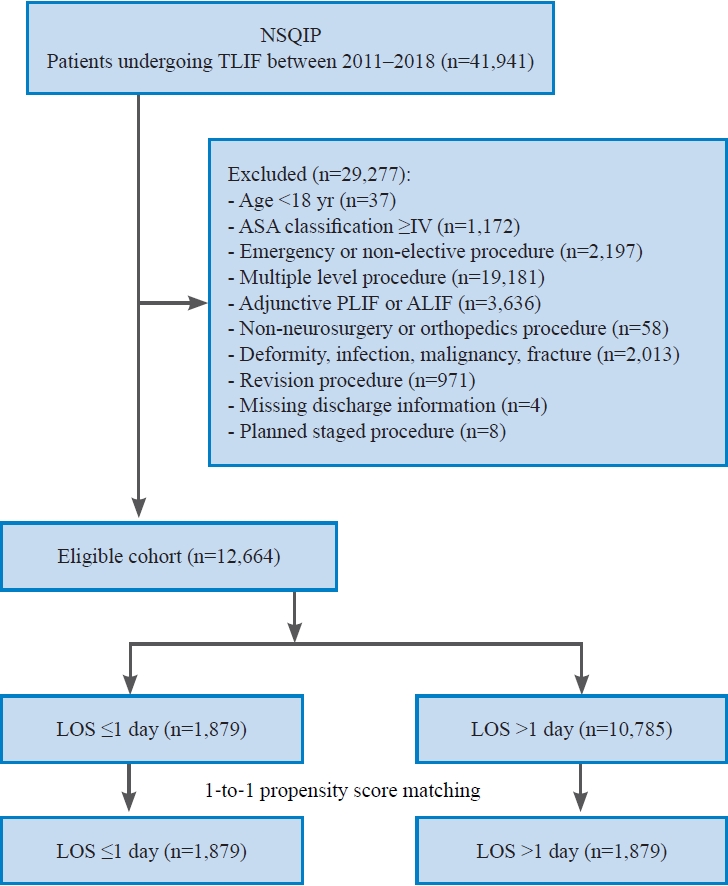
The ACS-NSQIP encodes procedures using current procedural terminology (CPT) codes and diagnoses with International Classification of Diseases (ICD), 9th or 10th Revision, Clinical Modification codes. Patients were included if they had CPT code 22612 (arthrodesis, posterior or posterolateral technique, single-level; lumbar [with lateral transverse technique, when performed]). Patients were excluded if they (1) were <18 years old; (2) had an ASA score of ≥4 because these patients are unlikely to be considered candidates for discharge on postoperative day 1; (3) underwent an emergency or nonelective procedure; (4) received a multilevel fusion (identified by CPT code 22614); (5) received an adjunctive posterior or anterior lumbar interbody fusion; (6) had undergone a procedure that was not performed by either a neurosurgeon or orthopedic surgeon; (7) had a postoperative ICD or CPT code corresponding to a deformity, infection, malignancy, or fracture; (8) had undergone a revision procedure, (9) had a missing discharge date, or (10) had undergone a staged procedure, defined as a related, planned reoperation for spinal fusion during the same admission (Fig. 1).
Covariates
Several variables as predictors of primary and secondary endpoints were collected from the ACS-NSQIP database. The following data were collected: patient age, sex, race, height, weight, ASA classification, functional status (independent or dependent), elective admission status, diabetes, smoking, chronic obstructive pulmonary disease, congestive heart failure, hypertension, corticosteroid use for a chronic condition, hematocrit, sodium, partial thromboplastin time (PTT), international normalized ratio (INR), platelets, and leukocyte count. Age was categorized at the 25th and 75th percentiles for the eligible study population, which resulted in age groups 18–54 years, 55–71 years, and >71 years. Anemia was defined as <41% in males and <36% in females. Platelets were categorized as <150,000/µL or ≥150,000/µL; leukocytes as ≥12,000/µL, <4,000/µL, or in between; albumin as ≥3 g/dL or <3 g/dL; sodium as ≥135 mEq/L or <135 mEq/L; PTT as >40 seconds or ≤40 seconds; and INR as >1.4 or ≤1.4. Height and weight were used to calculate the body mass index (kg/m2) and then categorized into World Health Organization (WHO) class I obesity (30–34.9 kg/m2), WHO class ≥II obesity (≥36 kg/m2), and nonobese. Each patient’s primary postoperative diagnosis, reported with ICD codes, was collected from the registry and categorized into the following groups: spinal stenosis, degenerative disk disease (DDD), disk displacement, spondylosis, and spondylolisthesis.
Numerous procedural/hospital characteristics were also analyzed. Information regarding the surgeon’s specialty, operation length, and use of a graft (CPT codes 20930, 20931, and 20936–20938) was also collected. Operative time was categorized by selecting the 30-minute intervals nearest to the 50th and 75th percentiles of the eligible study population (150 minutes and 220 minutes, respectively). The graft type was categorized as allograft or autograft.
Outcomes
The primary outcome of interest was LOS, measured as the number of calendar days between the day the procedure was performed and the day of discharge. The study specifically focused on patient characteristics and operative factors that resulted in LOS of >1 day; therefore, the study population was divided into cohorts of individuals having LOS ≤1 day and LOS >1 day. Based on this categorization, patients in the LOS ≤1 day cohort were either discharged on the same day of the procedure or after 1 night of overnight observation.
A concern in discharging patients early or performing procedures in the ambulatory setting is that those who experience complications may not be immediately recognized and treated. The secondary endpoints of our study were readmission rates and postdischarge complication rates within 30 days including reoperation, blood transfusion, wound-related infection (both superficial and deep incisional surgical site infections), deep venous thrombosis (DVT), pulmonary embolism (PE), sepsis (including septic shock), pneumonia, urinary tract infections, myocardial infarction, unplanned intubation, wound dehiscence, failure to wean from the ventilator within 48 hours, and acute renal failure. The predischarge complication rates were also compared to better understand which complications precluded patients from being discharged within 1 day.
Missing data
Missing data in the ACS-NSQIP database reflect laboratory values that were either not obtained preoperatively or were missing from the registry. Baseline rates of missing data were assessed for each laboratory value and were then imputed using a nonparametric multiple imputation missForest method, based on the random forest machine-learning approach [11]. Variables imputed in this manner included hematocrit, leukocyte count, platelet count, sodium, PTT, and INR.
Statistical analysis
To determine the baseline differences between patients with LOS >1 day and ≤1 day, unadjusted comparisons were first performed between groups using Pearson’s chi-square tests for categorical variables and independent two-sided Student t-tests for continuous variables. To evaluate for predictors of LOS >1 day, separate univariate logistic regression analyses were first performed to screen each covariate for its ability to predict LOS >1 day; thereafter, covariates with a p-value of <0.20 in the univariate analysis and present in >1.0% of the study population were entered into the final multivariate logistic regression model.
To elucidate whether individuals discharged within 1 day were at greater risk for postdischarge complications, a propensity-score matching algorithm was utilized to select LOS >1 day and LOS ≤1 day cohorts for comparison using all collected covariates; therefore, the selected cohorts should be similar with respect to these characteristics. Patients from the LOS >1 day group were paired with those from the LOS ≤1 day group in a 1:1 ratio using a balanced nearest-neighbor approach. Baseline characteristics were compared in the matched groups using Pearson’s chi-square test and Welch’s two-sample t-test to ensure that differences were eliminated by matching.
Which patients who were discharged within 1 day and were most likely to be readmitted within 30 days were also sought. To accomplish this, a backward stepwise logistic regression analysis over all collected covariates with 30-day readmission as the outcome and reported readmission rates by each covariate subgroup as percentages of the population within that subgroup was performed [12,13].
A p-value of <0.05 was defined a priori to represent statistical significance; however, because 26 independent comparisons were made between matched and unmatched groups with respect to covariates, Bonferroni multiple comparisons correction was applied. After correction, the p-value for significance was adjusted to <0.002 for the entire study [14]. Accordingly, 99.8% confidence intervals (CI) were reported for all odds ratios (OR). All statistical analyses were performed using R ver. 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria), and propensity-score matching was performed using the R package MatchIt ver. 3.0.2 (R Foundation for Statistical Computing) [15].
Results
Patient selection and study cohort
A total of 41,941 patients were identified in the ACS-NSQIP database as having undergone a TLIF between 2011 and 2018. After applying all the exclusion criteria, a total of 12,664 patients were deemed eligible for the study, of whom 1,879 (14.8%) had LOS ≤1 day and 10,785 (85.2%) had LOS >1 day. The mean age of the study population was 62.3±12.8 years, with 6,966 being female (55.0%). The most common diagnostic category was spinal stenosis, followed by spondylolisthesis and DDD. A complete listing of patient demographics and comorbidities for the entire study population is presented in Table 1.
Length of stay
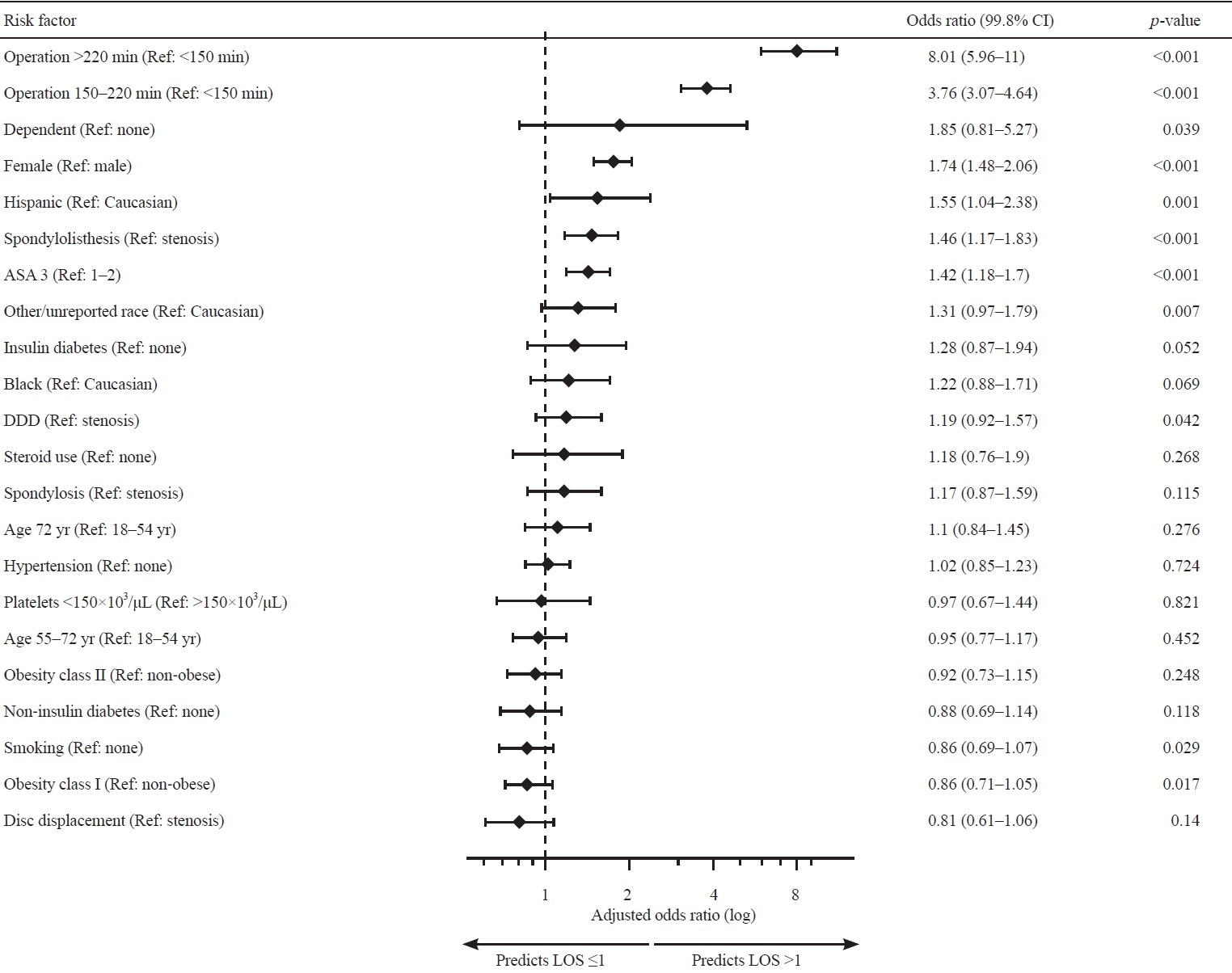
The results of the multivariable logistic regression model for LOS are presented in Table 2. Associations were noted between increased LOS and female sex (OR, 1.74; 99.8% CI, 1.49–2.06; p<0.001), Hispanic identity (OR, 1.55; 99.8% CI, 1.04–2.38; p=0.001), diagnosis of spondylolisthesis (OR, 1.46; 99.8% CI, 1.17–1.83; p<0.001), ASA category 3 (OR, 1.42; 99.8% CI, 1.18–1.7; p<0.001), and operation lengths of 150–220 minutes (OR, 3.76; 99.8% CI, 3.07–4.64; p<0.001) and >220 minutes (OR, 8.01; 99.8% CI, 5.96–11.0; p<0.001) (Fig. 2).
Propensity-score matching
All baseline differences between the study cohorts were completely eliminated by propensity-score matching, and the resulting matched groups were similar in all collected characteristics (Supplement 1). In terms of predischarge complication rates, patients who had LOS >1 day were more likely to have received intraoperative or postoperative blood transfusions (0.3% versus 4.5%, p<0.001) and were more likely to have undergone reoperations (0.1% versus 0.6%, p=0.004), although the latter did not reach statistical significance upon multivariable logistic regression (Table 2). No significant differences in the postdischarge complication rates were found between the matched cohorts.
30-Day unplanned readmission
Table 3 presents the results of the stepwise logistic regression model for 30-day unplanned readmission for patients with LOS ≤1 day. The factors that demonstrated the strongest associations were female sex, dependent functional status, hypertension, chronic steroid use, and thrombocytopenia. Of these, dependent functional status was the only significant predictor of readmission in the cohort of patients who were discharged on or before postoperative day 1 (OR, 8.4; 99.8% CI, 1.75–30.41; p=0.001).
Discussion
This study presents a review of patient and intraoperative factors and complications associated with LOS ≤1 day for single-level TLIF between 2011 and 2018 using the ACS-NSQIP database. In this study, female sex, Hispanic ethnicity, diagnosis of spondylolisthesis, ASA classification 3, and operation lengths of 150–220 minutes and >220 minutes were found to be associated with LOS >1 day. Patients with LOS >1 day who received intraoperative or postoperative blood transfusions were more likely to undergo a reoperation. However, no differences were found for the 30-day readmission rates or postdischarge complication rates between the LOS ≤1 day and LOS >1 day cohorts. In the LOS ≤1 day cohort, dependent functional status was significantly associated with unplanned readmission within 30 days.
Risk factors of prolonged length of stay
Female sex, which represented 55.0% of the cohort in this study, was a significant risk factor for LOS >1 day. This may be due to an increasing number of female patients undergoing spine surgery and the gender bias in female patients using more medical care than male patients [16,17]. This finding is consistent with those of previous studies, although conflicting results have also revealed that men had a greater risk of reoperation after lumbar spine surgery [17,18]. Socioeconomic status in relation to race, insurance status, and marriage affects surgical outcomes [19]. One study of 1,896 patients undergoing cervical spine surgery showed extended LOS in patients identified as non-White, which is similar to our study population [20]. However, this finding remains controversial because other studies have not found an association between race and clinical outcomes [21].
Preoperative spondylolisthesis was associated with LOS >1 day compared with other indications for single-level TLIF. Spondylolisthes result from the degeneration of the weight-bearing facet joints, leading to the anatomical slippage of the vertebrae and altering the sagittal balance of the spine [22]. Consequently, hyperlordosis of the spine occurs as a compensatory mechanism; therefore, additional inpatient management such as physical and occupational therapy may convey a perceived postoperative benefit [6,9]. Other studies have suggested that surgical intervention for spondylolisthesis has better outcomes than other indications such as DDD or spinal stenosis, although these studies focus on long-term outcomes rather than on postoperative LOS [23,24]. Higher ASA class has been well established with longer LOS, complications, and readmission after spine surgery and was consistent with our findings [17].
Intraoperative factors of operation lengths of 150–220 minutes and >220 minutes were associated with LOS >1 day. In the LOS >1 day cohort, they were associated with receiving a perioperative blood transfusion and undergoing unplanned reoperation. Cases with longer operating times have increased complexity, leading to increased estimated blood loss and risk of complications [7,17]. Furthermore, patients who receive perioperative blood transfusions are more likely to have higher estimated blood loss and/or lower preoperative hemoglobin levels, indicating a higher likelihood of preexisting comorbidities [7]. Increased rates of unplanned reoperation may result from the increased complexity and complications in these patients [25]. Overall, these results are consistent with those of previous studies. A case series of 78 patients undergoing single-level minimally invasive (MIS) TLIF similarly found that patients who had higher estimated blood loss, lower preoperative hemoglobin levels, and longer operating times were likely to have LOS >1 day [26]. Another study of 4,995 patients undergoing single-level TLIF showed that longer operative times were associated with higher readmission rates [17].
Regardless of whether patients were discharged within 1 day or >1 day, no differences in postdischarge complications and readmissions were found. However, among patients with LOS ≤1 day, those with dependent functional status were associated with readmission within 30 days. This increased readmission rate may be explained by functionally dependent patients who are more likely to have complicated medical histories and are potentially more likely to require assistance with activities of daily living [27,28]. In cervical spine and orthopedic surgeries, a dependent functional status has been associated with increased readmission rates and worse outcomes, such as nonhome discharge, prolonged hospital stay, reoperation, and reintubation, which is consistent with our results [27,28].
Limitations
As a retrospective national database study, its limitations must be noted. In particular, the variables in the ACS-NSQIP database are predetermined and were not originally constructed to analyze risk factors associated with single-level TLIF. In addition, both open and MIS approaches for single-level TLIF use the same CPT code; thus, distinguishing between the two approaches using the NSQIP database is impossible. MISTLIF is known to have shorter LOS, fewer complications, and improved functional recovery [29,30]. As such, the analysis may bias LOS ≤1 day to incorporate more patients with MIS-TLIF compared with LOS >1 day. Furthermore, variables such as hematoma formation and screw misplacement are not quantified in the database, which may further elucidate why patients undergo reoperation. In addition, postoperative complications previously shown to significantly affect LOS, such as DVT, PE, and pneumonia had low incidence rates in the NSQIP database, indicating the need for a larger sample size to accurately quantify the risk of these complications. Similarly, data on the exact causes of certain outcomes, such as unplanned readmission or reoperation are not available in the NSQIP database, warranting additional prospective studies to identify these causes. However, surgeons may consider these perioperative factors for patients undergoing single-level TLIF as an ambulatory procedure or those requiring inpatient management.
Conclusions
This study using the ACS-NSQIP database for single-level TLIF revealed that patients with a higher ASA class, diagnosis of spondylolisthesis, female sex, Hispanic identity, and prolonged operative time were more associated with LOS >1 day. Patients with LOS >1 day were associated with perioperative blood transfusions and unplanned reoperations. For patients with LOS ≤1 day, a dependent functional status was associated with unplanned 30-day readmission. These factors should be considered when selecting patients for single-level TLIF to reduce the risk of prolonged hospitalization and associated complications.