Introduction
Kyphosis is one of the most common physical disabilities seen older adults. Older adults with severe kyphosis are suggested to be at an increased risk of falls and impaired activities of daily living (ADLs) [1,2]. Kyphosis is thought to be caused by (1) vertebral fractures, (2) back and limb muscle weakness, and (3) intervertebral disc degeneration [3–5]. These factors are inseparable from aging. Japan is an aging society, with 25% of the population aged ≥65 years [6], and kyphosis-induced ADL decline is a social problem [7]. Osteoporosis is undoubtedly the main disease that triggers the factors causing kyphosis deformities. Additionally, locomotive syndrome (LS) is common in older adults, has a sufficient effect on physical performance and ADL, and causes kyphosis deformities [8].
Moreover, sarcopenia is predominantly associated with muscle weakness and causes kyphoscoliosis deformities. The kyphosis deformity has been associated with sarcopenia following surgery for spinal deformity [9]; however, the association between age-related kyphosis and sarcopenia is unclear. The Japanese Orthopaedic Association has defined LS as the condition of restricted walking. LS primarily affects older adults, characterized by reduced mobility because of locomotive organ dysfunction, such as muscles, bones, and joints. First defined by the Japanese Orthopedic Association in 2007, LS is associated with age-related musculoskeletal degeneration, such as osteoarthritis (OA), osteoporosis, and sarcopenia. LS presents a significant societal and healthcare challenge, particularly in aging societies, because it increases the risk of disability and dependency [10,11]. An association between LS-induced back muscle weakness and kyphosis deformity has been suggested in Japanese men [12].
Many musculoskeletal problems are associated with older adults; however, no studies have univocally evaluated the association between osteoporosis, sarcopenia, LS, and kyphoscoliosis deformity. Knee OA progression was more pronounced among workers in mountainous regions than in those working elsewhere because of their working environment [13]. Furthermore, compared with those living in the plains, older residents of mountainous regions have a higher prevalence of low back pain (LBP), indicating that life in mountainous areas significantly affects the limbs and lumbar spine [14]. Thus, the relationship between osteoporosis, sarcopenia, and LS and lumbar alignment may be more pronounced in residents of mountainous regions than in those living elsewhere. Examining the factors associated with kyphosis and the effect of kyphosis on the ADLs of patients aged >65 years would be substantial for the future medical care of older adults, given the increasing older population.
This study focused on older adults to examine the relationship between factors associated with kyphosis and ADL decline in the older population.
Materials and Methods
This study was based on the results obtained in a cross-sectional cohort of participants enrolled in the Good Ageing and Intervention Against Nursing Care and Activity Decline (GAINA) study. The GAINA study, which began in 2014, is a population-based cohort study of 3,352 participants from mountainous area in Japan, who received annual town-sponsored medical check-ups. In this region, 42.9% of the population was >65 years old in 2014. For the study, residents aged ≥40 years in the relevant area were sent a screening questionnaire and a consent form. In this study, enrollment was open to all participants who agreed to participate in the GAINA study from 2014 to 2018, and attendance during the study period was voluntary. For this study, individuals who (1) lived independently, (2) can walk to the survey location, and (3) agreed to provide self-reported data were included.
1. Participants
This cross-sectional study enrolled 469 inhabitants who were living in a local mountain area and underwent medical check-ups between 2014 and 2018. Of these inhabitants, 361 aged ≥65 years (mean age, 75.0 years) were included.
This study was conducted in compliance with the principles of the Declaration of Helsinki. The study’s protocol was reviewed and approved by the institutional review board of Tottori University (IRB approval no., 2354; February 26, 2014). All participants provided written informed consent. Survey items included kyphosis index [15], body mass index (BMI), back pain prevalence, back pain Visual Analog Scale (VAS) score, Oswestry Disability Index (ODI), walking speed, grip strength, skeletal mass index, osteoporosis (% young adult mean [YAM]), and LOCOMO 5 score.
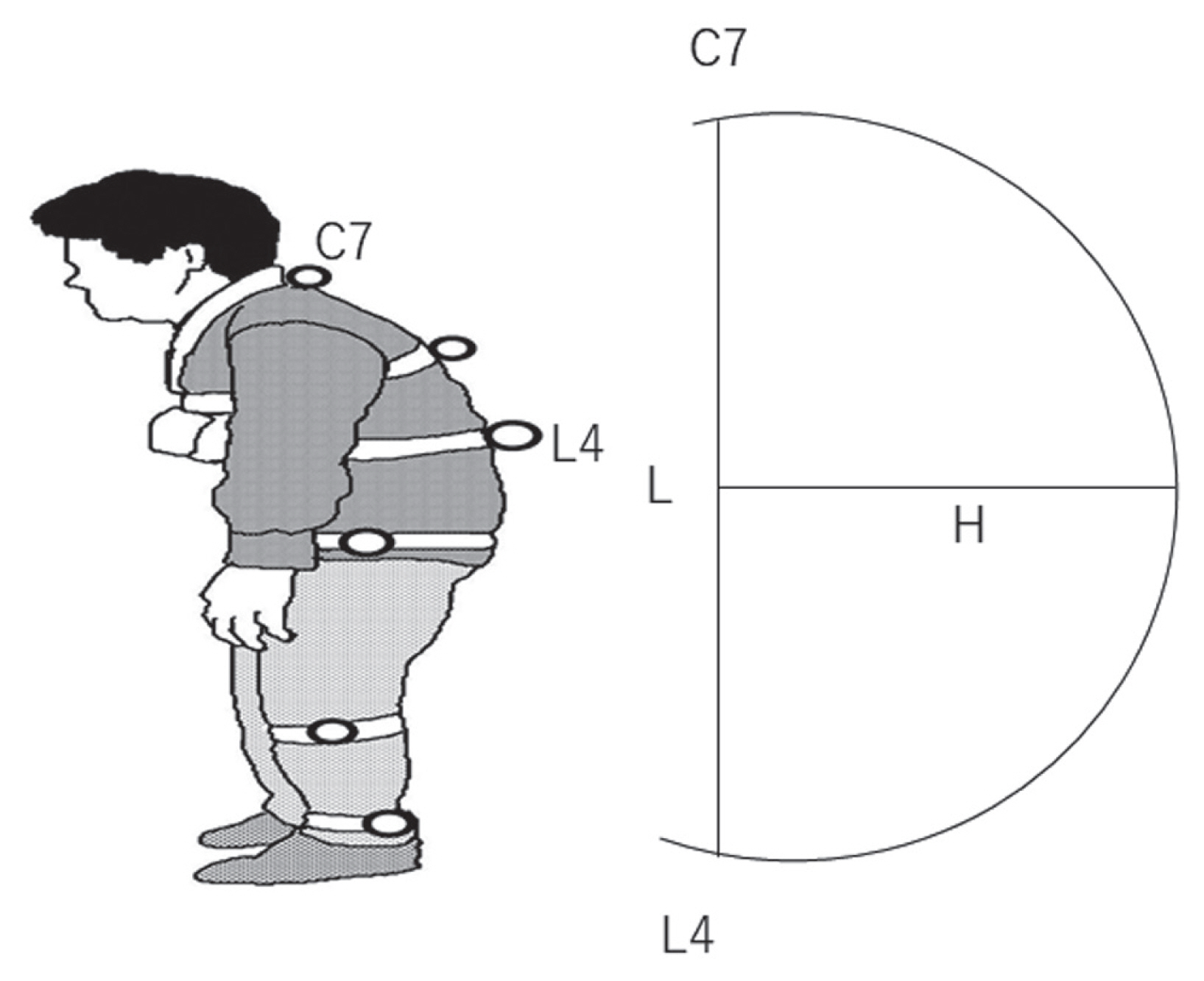
LOCOMO 5 is a simplified version of the 25-question Geriatric Locomotive Function Scale that screens for LS [16]. This evaluation method is based on a 20-point scale, with a score of ≥6 indicating a high sensitivity and specificity for determining LS [17]. Therefore, this study considered residents who scored ≥6 points on the LOCOMO5 to have LS and sarcopenia (Asian Working Group for Sarcopenia) [18]. The kyphosis index was produced by affixing landmarks to the participant’s body parts (spinous processes of the 7th cervical vertebra to the 4th lumbar vertebra), photographing the standing posture from the sagittal plane, and using the Image J (National Institutes of Health, Bethesda, MD, USA). The straight line connecting the spinous processes of the 7th cervical vertebra and the 4th lumbar vertebra was defined as L (cm), the distance from the straight-line L to the apex of curvature as H (cm), and the ratio was calculated as H/L×100 (Fig. 1). The participants were divided into the following three groups according to the kyphosis index [15]: normal (N) group (kyphosis index: <12; n=229, 63.4%), moderate (M) group (kyphosis index: 12 to <15; n=99, 27.4%), and kyphosis (K) group (kyphosis index: ≥15; n=33, 9.2%). Survey items were compared among the groups. A p-value of <0.05 was considered significantly different. Logistic regression analysis was performed to investigate the associated factors of kyphosis (kyphosis index: ≥15).
2. Baseline characteristics and questionnaire
The baseline characteristics of age, sex, height, body weight, and BMI were recorded for each participant. The intensity of LBP was indicated by each participant by drawing a vertical mark on a 100-mm horizontal VAS.
The ODI was used to assess functional outcomes associated with LBP. All participants were asked about these questions, regardless of whether they had or had no back pain. Considering the older age of the participants, each participant was directly interviewed by the examiners to ensure that there were no accuracy issues. A history of falls and vertebral fractures was checked for 1 year to evaluate ADL performance.
3. Body function and structural measurements
The handgrip strength was measured using a TKK 5401 dynamometer (Takei Co., Niigata, Japan). The participants were asked to squeeze the dynamometer twice with each hand. Grip strength was performed with the left and right hands, and the higher value was recorded.
A bioelectrical impedance analysis (BIA) with an MC-780A (Composition Analyzer: Tanita Co., Tokyo, Japan) was conducted to investigate muscle mass. The BIA method requires the participants to step onto a platform and maintain a standing position for approximately 30 seconds. The skeletal mass index (SMI) was calculated by dividing the limb muscle mass (kg) by height squared (m2). Quantitative ultrasonography (QUS) was used to assess the calcaneal bone mass. A CM-200 sonometer (Furuno Co., Nishinomiya, Japan) was used to evaluate the speed of sound through the calcaneus. Participants were asked to place their right heel on the QUS device in a sitting position. %YAM was used to explain bone mineral density as a result of the QUS. A 10-m walking line was prepared. The walking and measurement sections were set. The participants completed a single trial at free speed following the instruction “At usual walking speed.” Walking speed was calculated using OPTO Gait analysis software ver. 1.6.4.0 (Microgate S.r.L, Bolzano, Italy).
4. Assessment of sarcopenia
The participants were classified as having sarcopenia based on muscle mass, muscle strength, and physical performance. The classification was based on the recommendations of the Asian Working Group for Sarcopenia, which classified participants as having sarcopenia if they were >60 years old and had a low handgrip strength (<26 kg in men and <18 kg in women) and/or a lower walking speed (<0.8 m/sec) with a low muscle mass (<7.0 kg/m2 in men and 5.7 kg/m2 in women).
5. Statistical analysis
All data are expressed as means±standard deviations. The survey items were compared among the groups. Differences in characteristics, demographics, VAS of LBP, and ODI of the participants and the prevalence of falls, LS, and sarcopenia among the three groups were examined using the Steel–Dwass test. A p-value of <0.01 was considered significantly different. To determine factors associated with kyphosis, a logistic analysis was performed with a kyphosis index of ≥15 as the dependent variable and factors demonstrating a significant difference (p<0.01) as the explanatory variables. Data were analyzed with StatMate for Windows ver. 4.01 (ATMS Corp., Tokyo, Japan).
Results
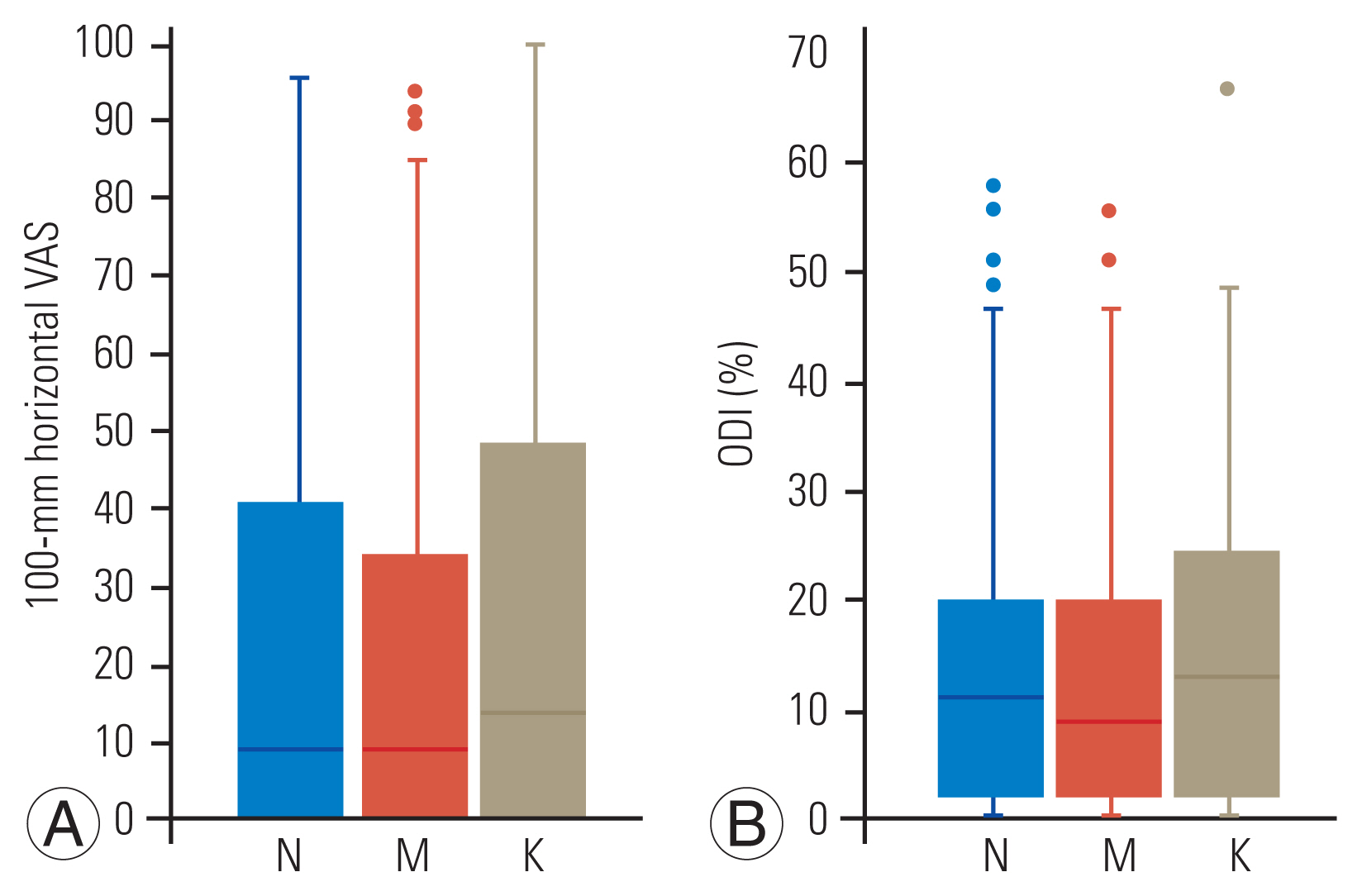
The K group had the highest age and the lowest bone density (%YAM) and gait speed than the M and N groups. No significant differences were found for sex, height, weight, BMI, grip strength, and SMI (Table 1). VAS and ODI were not significantly different among the three groups. No difference was found in the rate of sarcopenia among the three groups (Fig. 2).
LS was significantly higher at 42.4% in the K group compared with 18.3% and 24.2% in the N and M groups, respectively (Table 2). Falling at least once during the year was reported in 24.2% of the participants in the K group compared with 21.0% and 16.7% in the N and M groups, respectively. No difference was found in the rate of falls among the three groups (Table 2).
The association between spinal kyphosis and falls revealed that falls were significantly more common in the K group. A logistic analysis of the factors associated with a round back was conducted using a round-back index of ≥15 as the dependent variable. Bone density loss was associated with a round back.
Logistic analysis with age, LS incidence, gait speed, and bone mineral density as explanatory variables and a round back (kyphosis index: ≥15) as a dependent variable revealed that bone mineral density was an independently associated factor (odds ratio, 0.21; 95% confidence interval, 0.04–0.96), and lower bone mineral density was associated with kyphosis (Table 3).
Discussion
This study examined factors related to a round-back posture in older residents of a mountainous area and further examined whether a round back is associated with sarcopenia and LS. The results revealed that a high degree of a round-back posture with a kyphosis index of >15 was associated with decreased bone mineral density. Residents with round back had a higher incidence of LS and were more prone to falls.
Generally, a round back was defined by vertebral fractures, disc degeneration [19], and muscle weakness [20,21]. Kasukawara et al. [22] evaluated the relationship between muscle strength and kyphosis in 572 community residents aged ≥50 years, and back extensor strength was revealed to be associated with high thoracic kyphosis in both men and women. A study evaluated the back strength of women aged ≥30 years and reported a decrease in back strength over time with every 10-year generation [23].
Our back muscles may lose strength as we age, thereby leading to a round back. Additionally, the Osteoporotic Fractures in Men Study of men aged 65 years revealed low bone density and disc degeneration as risk factors for kyphosis progression [24]. The present study revealed an association between low bone density and kyphosis.
We did not directly evaluate the association between back muscle strength and kyphosis; however, we examined grip strength and kyphosis and did not find an association. We speculate that kyphosis was not caused by poor back muscle strength, although indirectly, in the community residents evaluated, because several studies have revealed that grip strength correlates with back muscle strength in older adults [25]. In the questionnaire, we asked for a history of vertebral fractures; however, we considered the association to be small because none of the participants had a history of symptomatic vertebral fractures. Intervertebral disc degeneration could not be evaluated in this study because imaging evaluations, such as X-ray and magnetic resonance imaging, were not performed.
This study revealed low bone mineral density as a factor independently associated with kyphosis. The Framingham Study, in which spinal computed tomography was performed on approximately 2,000 adolescents and young adults, revealed that low bone density is strongly associated with thoracic kyphosis and suggested that this factor may be predominantly genetic in origin [26]. One of the diagnostic criteria for osteoporosis is %YAM measured by the dual-energy X-ray absorptiometry (DXA) in <70% of the patients [27]. In the present study, the mean %YAM of the K group with severe kyphosis was 70.8±13.5, although measured by the QUS method, which is a considerably lower bone mineral density. Therefore, kyphosis deformity may be observed in older patients because of a combination of subclinical vertebral fractures and disc degeneration caused by low bone density.
The association between kyphosis and sarcopenia, falls, and LS was also examined. The results revealed that sarcopenia was not associated with kyphosis; however, residents with kyphosis had a higher frequency of falls and a higher prevalence of LS. Although many studies have used X-ray imaging to evaluate kyphosis, several others have used postural assessment methods other than X-ray imaging to evaluate kyphosis and ADLs.
Tominaga et al. [28] evaluated the relationship between kyphosis and falls and fear of falling using the wall-occiput test (distance from the back of the head to the wall) as the criterion for kyphosis in residents aged ≥40 years. The results revealed a correlation between kyphosis and a 1-year history of falls in men [28]. Takahashi et al. [29] defined kyphosis using surface markers and evaluated the relationship between kyphosis and ADLs in residents aged ≥65 years. Sugai et al. [7] classified 532 residents with kyphosis using the simplest illustration-based method compared with previous report and revealed that residents with kyphotic deformities had lower ADLs. The results were generally similar to other reports, including ours [30,31]. Evaluation of kyphosis using a simple method that does not require X-ray imaging is considered acceptable for assessing the relationship with ADLs.
The results of this study revealed an association between low bone density and kyphosis. This is different from muscle weakness, which is the most common cause. This may have been influenced by the average age of the participants of >70 years, and many participants were female.
Some studies suggesting a relationship between muscle weakness and arched back have included participants in their 40s, or the participants were in their 60s on average age, which is a relatively young age range [20]. Woods et al. [24] reported that thoracic kyphosis is greater in older men with a BMI of <30 kg/m2, small paraspinal muscle mass, and localized muscle mass and kyphosis relationship.
The relationship between the thoracic spine and kyphosis is likely to be influenced by the sex and age of the participant. However, many studies have suggested that exercise therapy has some benefits, given that kyphosis is often associated with muscle weakness and is associated with several fall events and decreased ADL performance [32].
These reports cover a wide age range, including a relatively young group aged 40–60 years [33]. Therapeutic intervention for low bone density should be considered in an older population, such as those in this study. Further studies, including longitudinal studies and studies of adolescents and young adults, are necessary to identify factors associated with kyphosis. This study revealed an association between kyphosis and low bone mineral density mainly in older adults.
This study has several limitations. First, the results are limited by the bone density measurement method used. In this study, bone mineral density is shown in %YAM based on the results of the QUS. However, no clear criteria have been set for the diagnosis of osteoporosis using %YAM in QUS, which is originally a diagnostic criterion using the DXA method. QUS is a simple method; however, its positive predictive value for osteoporosis diagnosis is inferior to that of DXA [34]. In their analysis of 480 patients, Niimi et al. [35] reported that QUS demonstrated a moderate correlation with the bone mineral density of the proximal femur measured by DXA. In fact, the %YAM measured by QUS has been used as an indicator of bone density in various studies [36,37]. Further, we believe that QUS presents as a simple bone densitometry tool and must not have substantially affected the study results. Second, whole-spine alignment was not evaluated. The kyphosis index was used to evaluate the severity of kyphosis in this study. This method could infer kyphosis based on the vertebral bodies and intervertebral discs; however, it could not clarify whether pelvic alignment, such as pelvic incidence, affected kyphosis. Thus, future studies are needed.
Conclusions
In this study, we examined the factors associated with kyphosis in older residents of a mountainous area. In older adults living in mountainous areas, LS and sarcopenia were unrelated to kyphosis, whereas low bone density was independently associated with kyphosis. Moreover, kyphosis deformities were associated with falls.