Pseudarthrosis of the Cervical Spine: Risk Factors, Diagnosis and Management
Article information
Abstract
Cervical myelopathy and radiculopathy are common pathologies that often improve with spinal decompression and fusion. Postoperative complications include pseudarthrosis, which can be challenging to diagnose and manage. We reviewed the literature with regard to risk factors, diagnosis, controversies, and management of cervical pseudarthrosis.
Introduction
Spinal fusion was first described in the early 1900's for the treatment of Pott's disease in the thoracolumbar spine [123]. The anterior approach for cervical arthrodesis was introduced in the 1950's and subsequently became increasingly popular as it allowed access to anterior pathology [4567]. Despite technological advancements in spinal instrumentation and biologics, failed spinal fusion rates range as high as 50%, and the number of fusion procedures performed each year is increasing [5891011].
Pseudarthrosis refers to a failure of fusion after an index procedure intended to obtain spinal arthrodesis [4512]. The term suggests the presence of a false joint, although it is commonly used to describe a lack of fusion that occurs after an attempted arthrodesis. As not all patients with pseudarthrosis are symptomatic, the current literature likely underestimates the true incidence of this complication [891314]. Furthermore, multiple studies have shown that patients with pseudarthrosis are asymptomatic in approximately 30% of cases [81115]. Nonetheless, pseudarthrosis remains a leading cause of pain postoperatively and accounts for 45%–56% of revisions [16171819]. The literature has also shown a direct correlation between boney fusion and successful clinical outcomes [810121320].
Pathoanatomy and Risk Factors
Degeneration of the cervical spine may lead to cervical spondylotic myelopathy and/or radiculopathy. Degeneration of the intervertebral disc, uncovertebral joint, facet joint, ligamentum flavum, and posterior longitudinal ligament can cause spinal cord compression, myelopathy, and instability of the spine [710122122]. With extensive multi-level pathology and instability, obtaining a successful fusion may become more challenging. The most caudal level is involved in over 80% of pseudarthrosis occurring in multi-level arthrodesis [12]. This may be due to higher contact stress at the graft-body interface. Patient and surgical factors that impair vascularity, decrease stability, or increase stress through a fusion site can interfere with the intended arthrodesis.
The true etiology of pseudarthrosis is often not clear. Risk factors associated with pseudarthrosis following an arthrodesis include patient factors, multilevel fusions, type of bone graft, approach, and type of instrumentation [101112232425262728].
1. Patient factors
Patient issues of importance include smoking, obesity, diabetes, metabolic abnormalities, chronic steroid use, osteoporosis, malnutrition, chronic illnesses, age, and vascular abnormalities [12293031]. Older age has been associated with increased postoperative complications, although not with pseudarthrosis [32]. Interestingly, younger age has been significantly associated with a higher rate of symptomatic pseudarthrosis (43.8 years vs. 52.1 years; p<0.01) [12]. Although the reason is not entirely clear, this may be related to higher physical demands on the implant and fusion site or higher expectations in younger patients.
Smoking is associated with higher rates of pseudarthrosis [3031]. In a study of 160 patients who underwent anterior cervical corpectomy, current smoking status was an independent risk factor for pseudarthrosis as well as infection and longer lengths of stay [31]. Higher rates of fusion in nonsmokers were reported in smokers following anterior cervical discectomy and fusion (ACDF) with allograft (81% vs. 62%, p<0.05) [30].
Contrary to these studies, smoking was not associated with decreased fusion rates in patients undergoing posterior fusion with lateral mass and iliac crest grafting [33]. The authors suggested that in smokers, posterior spinal fusion should be considered to optimize fusion rates. Regardless, smoking has shown to increase the risk for nonunion in multiple studies as well as rates of other postoperative complications, such as infection, wound complications, and longer length of stay [31]. Thus, patients should be counseled appropriately during preoperative discussions.
Although duration and severity of symptoms and specific types of lesions seen in patients with ossification of the posterior longitudinal ligament (OPLL) have been negatively associated with patient outcomes, these factors have not been shown to be associated with pseudarthrosis [34]. These factors should still be considered in the process of judicious surgical planning (Table 1).
Risk factors for pseudarthrosis
2. Surgical considerations
Patients with progressive cervical radiculopathy or myelopathy often benefit from surgery and each surgical approach has specific benefits and complications to consider. There is considerable controversy between anterior, posterior, or combined anterior-posterior approaches. Planning the optimal surgical technique is dictated by, the number of involved levels, location of compression, underlying deformity sagittal and coronal alignment, severity of disease, presence of axial pain, patient baseline factors, and surgeon preference [223435].
3. Anterior versus posterior and combined approaches
ACDF and anterior cervical corpectomy and fusion (ACCF) allow access to the majority of compressive pathology (intervertebral discs, ventral osteophytes, and OPLL), restoration of cervical lordosis, and decompression over kyphotic deformities. Efficacy, neurologic improvement, and favorable outcomes have been reported [561120212435363738]. Classically, overall complication rates with anterior procedures are higher than with posterior procedures [8112021242527283940]. Recent reviews have shown comparable complication rates between anterior and posterior procedures with higher complication rates in combined anterior-posterior procedures. Zhu et al. [24] compared anterior (n=245) and posterior (n=285) procedures, and reported a significantly higher reoperation rate in the anterior group (21/245, 8.57% vs. 1/285, 0.3%; p<0.001). Of the 21 patients who underwent reoperation, 13/21 (62%) were for pseudarthrosis, 7/21 (33.3%) for adjacent deterioration, and 1/21 (4.8%) for loosening of implant. In the posterior group only 1 (0.3%) required reoperation for radiculopathy due to a new herniation, consistent with other studies [1940]. However, postoperative neurologic function and outcomes were more favorable in the anterior group (p<0.05).
Anterior plating has been shown to improve fusion rates with ACDF and ACCF in several studies [29414243]. A retrospective review of 540 patients who underwent anterior cervical plating with cortical allograft showed fusion rates of 96% and 91% for one and two level ACDF with anterior plate fixation, respectively, compared with 90% and 72% without anterior fixation, respectively (p<0.05) [41]. A meta-analysis of 2,682 patients assessed fusion rates in anterior cervical interbody fusion and corpectomy procedures with and without plate fixation [42]. Plate fixation improved fusion rates for all one, two, and three level ACDF's (p<0.001, 0.001, and 0.05, respectively). They also concluded that for three level procedures, corpectomy with plate placement was associated with higher fusion rates than discectomy with plate placement (82.5% vs 96.2%, p<0.05). Thus, plate fixation has become widely accepted in both ACDF and ACCF procedures.
A posterior approach may avoid the complications associated with anterior arthrodesis and is essentially an indirect decompression. Thus, the approach is not recommended in patients with underlying cervical kyphosis. The posterior approach is associated with higher postoperative pain, due to greater muscle trauma and denervation, a less cosmetic scar and a lack of direct access to anterior structures [44].
Pseudarthrosis rates are lower following posterior procedures as compared with anterior procedures [2538]. Other complications, such as neurovascular injury, screw malposition, iatrogenic foraminal stenosis, and adjacent segment degeneration, are more common than pseudarthrosis in posterior procedures [1927284044]. Although pseudarthrosis rates are typically lower after posterior procedures, patients undergoing posterior arthrodesis are reportedly 7.5-times more likely to undergo reoperation due to adjacent segment disease (ASD) than patients undergoing posterior decompression only, and 3.0-times more likely to undergo reoperation due to ASD than patients undergoing anterior arthrodesis [45]. Callahan et al. [46] studied outcomes after posterolateral bone-grafting and wiring and reported fusion rates of 96% (50/52). Heller et al. [47] compared laminoplasty with laminectomy and fusion in patients with multi-level CSM and recommended laminoplasty as no complications occurred in this group. Complication rates were higher in the laminectomy and fusion group and included nonunion (38%), ASD, implant failure, and donor site pain.
A systematic review concluded that both laminectomy with fusion and laminoplasty produce similar outcomes and complication rates for patients with multi-level cervical pathology [48]. Pseudarthrosis was seen in 1% (1/82), 8% (2/26), and 38% (5/13) in the three studies that reported on this complication. Overall, both surgical options were similarly effective, although the quality of evidence was graded as low as only retrospective cohort studies were examined.
If anterior and posterior pathology are present, a combined approach may be indicated. An analysis of the combined anterior-posterior and anterior only approaches reported improved sagittal alignment and better maintenance of the correction angle in the combined group with a follow-up of two years (p=0.001, postoperatively; p=0.043, two-year follow-up). Lower rates of pseudarthrosis (20% vs. 0%, p=0.034), cage subsidence (40% vs. 6.7%, p=0.025), hardware-related complications (26.7% vs. 0%, p=0.013), and clinical outcomes (p=0.046) were found in the combined group. However, operative time was significantly longer (86 minutes versus 266 minutes, p<0.05) and blood loss was greater (188 mL vs. 329 mL, p<0.05) in the combined group. These factors should be considered when planning a combined procedure (Table 2) [192432404749505152].
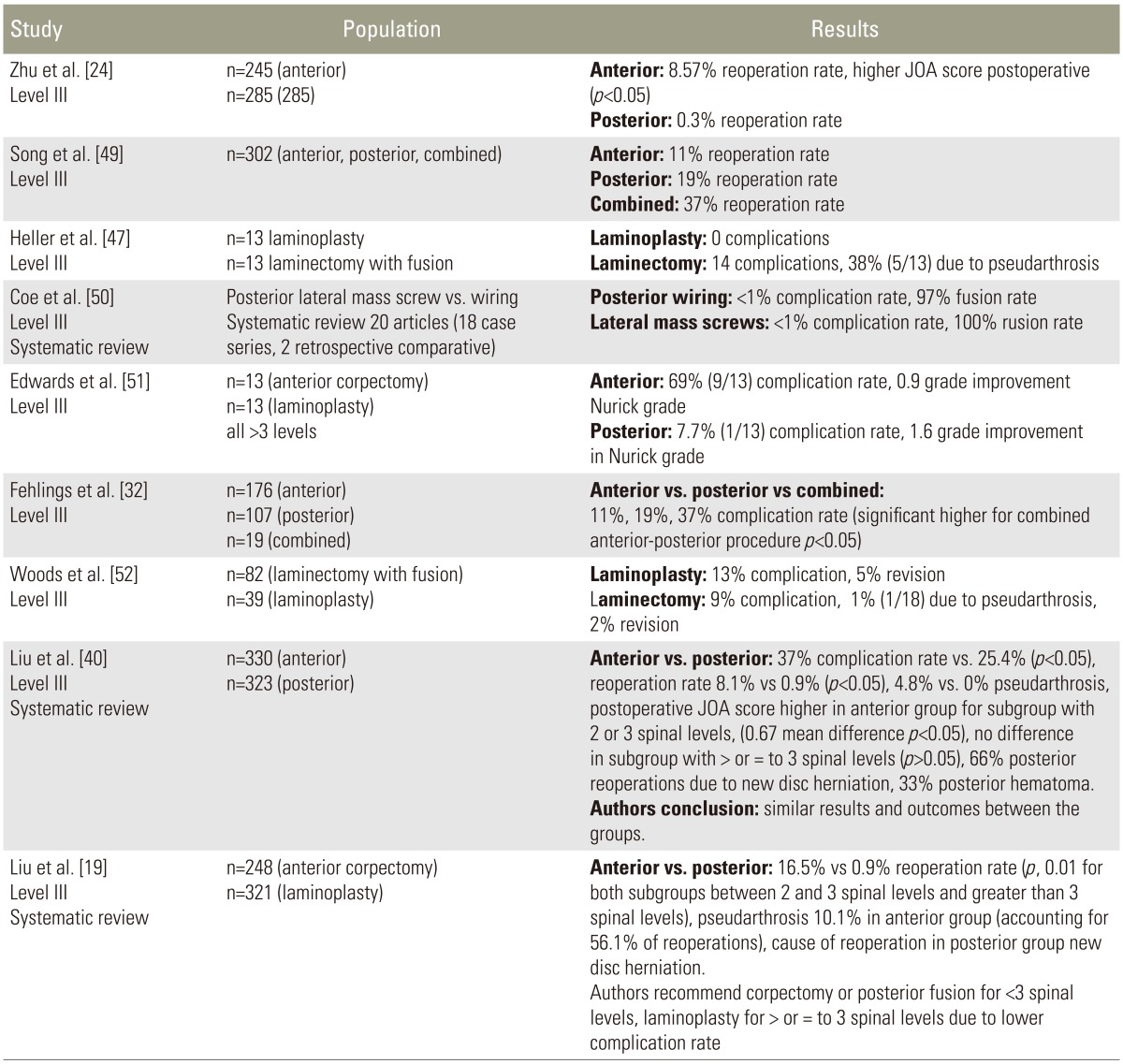
Anterior vs posterior vs combined cervical fusion
4. Multi-level cervical pathology
Increasing rates of pseudarthrosis with increasing levels of fusion have been reported [104353]. A report of one and two level ACDF's without instrumentation demonstrated a pseudarthrosis rate of 11% and 28%, respectively [43]. Another study reviewed 122 patients treated with ACDF with autogenous iliac crest bone graft and reported that the risk was significantly greater in multiple-level arthrodesis than after single-level arthrodesis (24/195, p<0.01) [10]. Similarly, high pseudarthrosis rates were reported in a review of patients undergoing three and four level ACDF's with iliac crest autograft and locking plates. Pseudarthrosis was found in 53% (8/16) of patients, although less than half (3/8) had enough pain to warrant a revision procedure [53]. The author concluded that although plating may improve fusion rates for ACDF's, three and four level fusions appear to have unacceptably high failure rates. A systematic review compared laminoplasty with corpectomy and fusion in patients with cervical myelopathy or OPLL (the groups were divided into 2- or 3-level involvement and ≥3-level involvement). The authors found significantly lower complications and reoperation rates, and less surgical trauma in the laminoplasty group (p<0.05) [1940]. A high percentage (56.1%) of reoperations were due to pseudarthrosis in the corpectomy group. The authors suggested that laminoplasty may be a safer option for >3 spinal levels, and either approach may be used for <3 levels. Complication rates were higher with anterior corpectomy, but postoperative neurological recovery and patient outcome scores were superior to posterior procedures, specifically in patients with >50%–60% spinal cord compression or <3 spinal level myelopathy or OPLL.
5. Bone grafting and biologics
Both the type of bone graft and use of biologic agents have been associated with the development of pseudarthrosis. Samartzis et al. [54] compared tricortical allograft with autogenous iliac crest tricortical graft in patients undergoing two- or three-level ACDF. Fusion rates and outcomes were assessed at a mean of 16 months. Almost all (78/80, 97.5%; p<0.05) achieved fusion and pseudarthrosis occurred in two patients who underwent allograft fusion, although this was not statistically significant. Regardless, clinical outcomes were similar between the two groups and were excellent and good in 88.8% of patients.
The same group also examined fusion rates comparing allograft and autograft following one level anterior cervical fusion with plate fixation [55]. They compared radiographic fusion at 12 months, risk factors, and patient reported outcomes between the two groups; 35 patients received allograft while 31 patients received autograft. Fusion was 100% in the allograft group and 90.3% in the autograft group with no statistically significant difference (p>0.05). Clinical outcomes were also not statistically different between the two groups. Typically, higher pseudarthrosis rates are seen when using allograft versus autograft with reported differences of 17%–27% versus 41%–62%, comparing allograft and autograft, respectively [255657].
Only one prospective study has been reported which compared recombinant human bone morphogenetic protein-2 (rhBMP-2) to autograft in patients undergoing ACDF [58]. Fusion rates of rhBMP-2 (0.9 mg per level) were slightly better than the use of iliac crest autograft with pseudarthrosis occurring in one of 30 receiving rhBMP-2 with allograft and 2 of 36 receiving iliac crest autograft. However, anterior neck swelling was reported in half of the rhBMP-2 patients. The United States Food and Drug Administration released a public health notification due to 38 reports of complications occurring with the use of rhBMP-2 associated with swelling, airway compression, neurologic injury, dysphagia, and dysphonia. Currently, rhBMP-2 is only approved for lumbar interbody fusion in skeletally mature patients with degenerative disc disease from L2–S1. rhBMP-7 is approved as an alternative to autograft for immunocompromised patients undergoing revision posterolateral lumbar fusion where autologous bone or bone marrow harvest are not expected to promote fusion [59]. Furthermore, issues with regard to higher cost, potential side effects, carcinogenesis, and inconclusive recommendations with regard to dosing and methods of insertion have dissuaded most spine surgeons from routinely utilizing rhBMP with cervical spinal arthrodesis.
Diagnosis
An accurate diagnosis of cervical pseudarthrosis can be difficult prior to a surgical exploration. High rates of asymptomatic patients and diagnostic tests lacking high sensitivity and specificity can cloud the diagnostic work-up. Regardless, if patients develop persistent symptoms or pain postoperatively, pseudarthrosis ought to be considered [489101214152360].
The work-up starts with a careful history and physical examination. Symptoms classically present as mechanical neck pain worsened by motion with radiation into the arm [812], although this can also occur with other underlying pathology. Disease progression, infection, implant failure, ASD, and postoperative pain syndromes should be ruled out.
The most common causes of axial or radicular symptoms after ACDF are pseudarthrosis and ASD, although as previously mentioned a relatively high percentage of patients with pseudarthrosis are asymptomatic [41213]. Younger age at the index arthrodesis is associated with a higher incidence of symptomatic pseudarthrosis. However, symptoms may vary which complicates the diagnostic work up. Lowery et al. [8] reported that in patients with pseudarthrosis, 27% felt the same and 64% felt worse. Patients who develop this complication often develop a various relapse in symptoms. Several reports have documented symptomatic cases ranging from 70%–80% [101353]. Newman [13] reported on 23 patients who developed pseudarthrosis after an anterior fusion and 16/23 (69.6%) had persistent symptoms. Thus, spine surgeon must be mindful, as 20%–30% of patients may be asymptomatic.
The initial work-up generally includes radiographs (lateral and flexion-extension views), thin-cut computed tomography (CT), and some recommend the use of magnetic resonance imaging (MRI), nuclear studies, or ultrasound in special situations [12143961]. Although imaging is important in the diagnostic work-up, the true diagnosis is only made upon surgical exploration [39].
Radiographic signs of pseudarthrosis include a lack of bridging trabeculae between the host bone and graft, motion exceeding 1 mm or 2 mm between spinous processes on maximal flexion-extension views and changes in the Cobb angles [12142139]. Measuring the distance between the tips of the spinous processes of the fused levels in flexion and extension views has also been documented as an accurate diagnostic method [21]. Cannada et al. [21] reported a specificity of 89% and sensitivity of 91% using this method, while changes in Cobb angle of >2 degrees resulted in a specificity of 39% and a sensitivity of 82%. However, a change in Cobb angle of >4 degrees significantly improves the specificity with a positive predictive value of 100%. Some studies also suggest using higher magnification (150% or 200%) on radiographic evaluation to better visualize an underlying pseudarthrosis [62].
CT scans are typically utilized when radiographic studies are inconclusive. While metallic artifact may obscure the assessment of fusion, the interobserver reliability of fine-cut CT is better than with flexion-extension radiographs [3963]. A prospective study evaluated intraoperative findings compared with CT, radiographs, and MRI in patients with pseudarthrosis after ACDF; the greatest concordance was between fine-cut CT and intraoperative findings (p<0.05) [39].
MRI is commonly used preoperatively during the work-up of cervical pathology, although its utility in detecting pseudarthrosis is questionable. Although artifact can obscure the surrounding tissues, it may be useful to identify surrounding structures and soft tissues for revision planning. It has been shown to be inferior to CT in diagnosing pseudarthroses, although there is no ionizing radiation, making it an appealing option. Buchowski et al. [39] found only fair interobserver reliability and moderate agreement with intraoperative findings when assessing MRI in patients with pseudarthrosis after ACDF
There are limited studies on the use of ultrasonography in the diagnostic work-up of pseudarthrosis. In one study, ultrasonography was used to diagnose pseudarthrosis, and a sensitivity of 100% was found in patients following instrumented fusions, though the specificity was 60% [63]. Bone scans and photon emission CT scanning have shown to have limited clinical utility in the work-up of pseudarthrosis.
Diagnosing pseudarthrosis can be a challenge as many conditions may mimic this process. The current literature supports the use of flexion-extension radiographs and CT scanning as the preferred diagnostic modalities [1214213960]. Special cases may warrant further studies.
Management
Symptomatic pseudarthrosis often warrants a surgical exploration and revision as successful arthrodesis is associated with improved patient outcomes [111237]. In planning the revision procedure, factors that should be considered include patient comorbidities, current symptoms, underlying deformity (such as postlaminectomy kyphosis), ASD, and prior postoperative complications (such as durotomy, pseudomeningocele, wound complications, neurologic injury, and hematoma) [58101239]. The approach, number of vertebral levels, type of bone graft, and instrumentation are important considerations to clarify during surgical planning (Table 3).
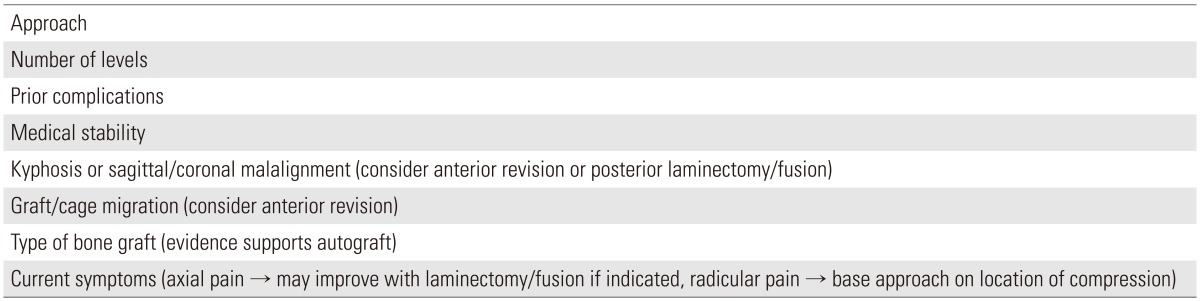
Planning surgical revision
Non-operative principals should be exhausted prior to revision surgery as pseudarthrosis alone is not an indication for revision. Nutritional counseling, smoking cessation, and the stabilization of medical comorbidities ought to be addressed prior to proceeding with a revision.
Although the use of allograft versus autograft in a primary cervical arthrodesis is contentious, most studies support the use of autograft in revision operations to optimize fusion potential and BMP is commonly utilized [4891012246164]. There is likely a limited healing potential inherent with the use of allograft as the underlying pathology is often related to diminished vascularity.
1. Anterior versus posterior revision
The surgical approach in terms of anterior versus posterior must be decided upon in planning the revision surgery. Proponents of the posterior approach highlight the avoidance of scar tissue and wound complications if the index procedure was anterior. Additionally, a posterior revision provides fresh soft tissue planes, a native fusion bed, and small studies have shown higher fusion rates [9126164]. Contraindications to a posterior approach include cervical kyphosis and graft or implant migration that can only be addressed from anteriorly [891264].
Although the approach is contentious, several studies have shown high fusion rates and improved patient outcomes with posterior decompression and arthrodesis [1216266164]. Treating pseudarthrosis posteriorly using iliac crest or local autograft and posterior wiring or lateral mass plating has been recommended [64]. In this study, 100% fusion was achieved using this approach, with no difference between iliac crest and local bone graft. However, relatively high rates of persistent complaints of pain in these patients despite high fusion rates were reported. A retrospective review of 120 patients provided further support for posterior fusion for pseudarthrosis after ACDF [61]. Of the 27 patients who underwent a repeat anterior spinal fusion, 12 required an additional revision, while of the 93 patients treated with a posterior procedure, only 2 required an additional revision operation (p<0.05). A slightly longer recovery and increased blood loss was observed in the posterior group though the higher fusion rates and lower incidence of a second revision procedure support the use of posterior fusion. Brodsky et al. [26] reported radiographic fusion rates of 76% in pseudarthrosis cases treated with anterior approach versus 94% in those treated from a posterior approach (p<0.05). Another review of cases of symptomatic pseudarthrosis reported that of 16 undergoing repeat anterior procedures, successful fusion occurred in 14 [12]. The two patients who did not fuse went on to undergo posterior fusions and achieved arthrodesis.
Contrary to these reports, some studies support using an anterior approach for the revision procedure [6566]. The advantages include lower rates of wound complications, access to anterior pathology and graft or implant migration, exploration of the pseudarthrosis site, and biomechanical advantages [6566]. The anterior approach also allows for better restoration of normal cervical lordosis and sagittal alignment and has been associated with less postoperative stiffness and pain [6567]. In a study of 35 patients treated for pseudarthrosis following ACDF, all cases were treated with anterior decompression and autogenous bone grafting; excellent results were reported in 29 patients, good results in one, fair results in four, and poor results in one [65].
Although pseudarthrosis can be treated with posterior or anterior approaches, the decision must be individualized based on the underlying pathology. Pseudarthrosis can also occur concomitant with other postoperative complications, such as ASD, hardware failure, or implant migration. Although the majority of the literature supports using a posterior procedure for the revision, most of these studies are low-quality retrospective studies from a single institution [12166164]. In the absence of kyphosis or anterior graft migration, posterior procedures may provide the most reliable option for achieving fusion, although prospective randomized studies are needed to better substantiate this question (Table 4).
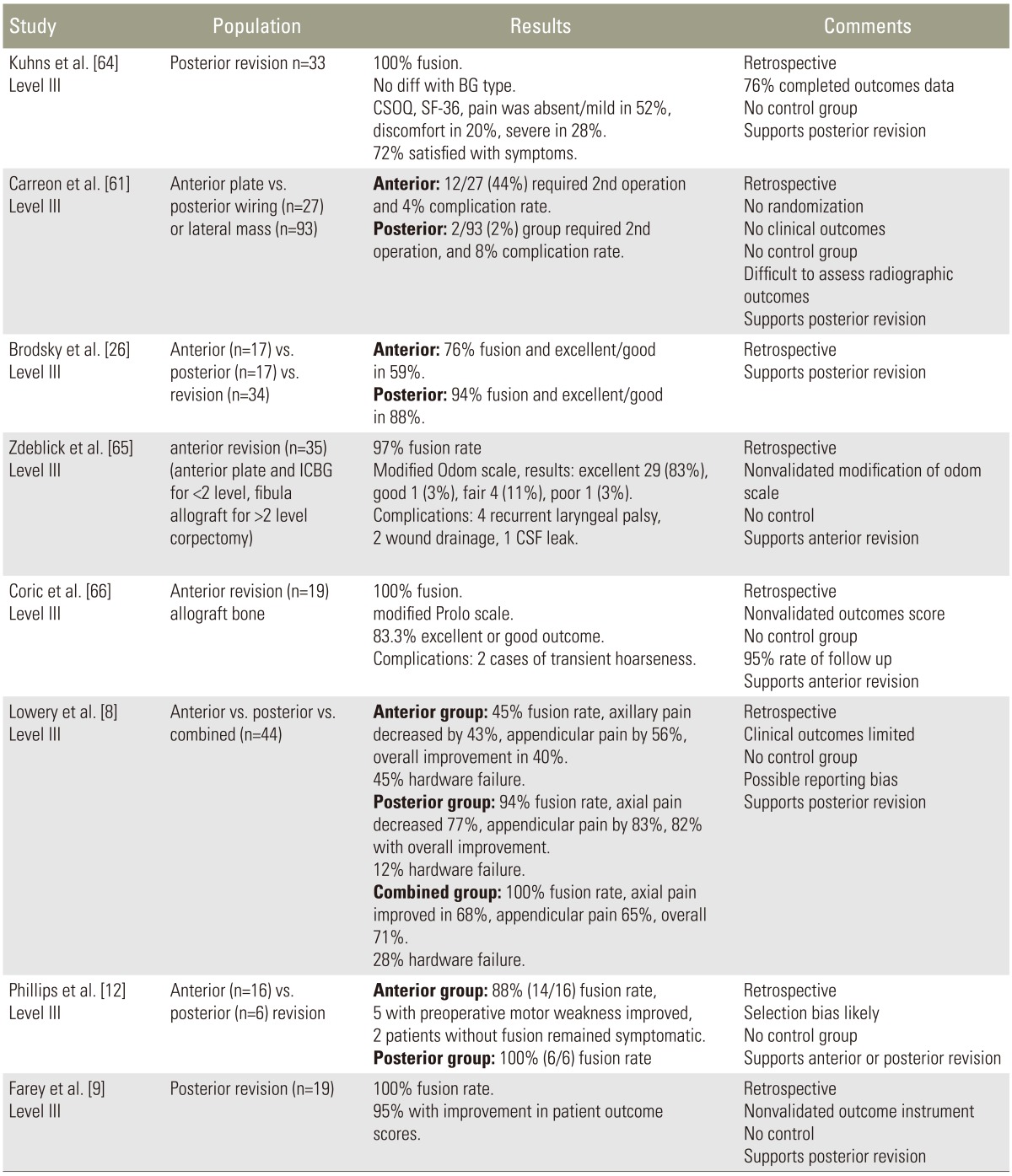
Comparison of revision procedures for pseudarthrosis
Conclusions
Degenerative pathologies of the cervical spine are frequently treated with surgery with favorable patient outcomes are supported in the literature. Pseudarthrosis is a common postoperative complication that may occur after anterior or posterior procedures, and can be challenging to diagnose and manage [8101253]. A thorough understanding of risk factors and diagnostic work-up as presented in this review may assist the spine surgeon in guiding proper management. High fusion rates with posterior revision procedures are supported in the literature, although several variables will determine the optimal management. There is a paucity of high quality studies. So, most recommendations are limited in strength and further large multicenter studies will enhance our ability to manage this complication.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.