Postoperative Segmental Motion up to 1 Year Following Single-Level Anterior Cervical Discectomy and Fusion: Plate versus Non-plate
Article information

Abstract
Study Design
Retrospective observational study.
Purpose
This study aimed to investigate the impact of plating on postoperative serial segmental motion and its correlation with clinical outcomes in single-level anterior cervical discectomy and fusion (ACDF) for up to 1 year.
Overview of Literature
The advantages and disadvantages of using cervical plating in ACDF have been well discussed; however, few studies compared the early serial segmental motions at the postoperative level between plating and non-plating.
Methods
In retrospectively collected data, 149 patients who underwent single-level ACDF for degenerative disease were enrolled and divided into non-plating (n=66) and plating (n=83). Interspinous motion (ISM) at the arthrodesis segment, Numeric Rating Scale (NRS) for neck pain, and Neck Disability Index (NDI) were serially evaluated at 3, 6, and 12 months postoperatively. Predictable factors for fusion, including age, sex, plating, diabetes, smoking, and type of grafts, were investigated, and fusion was defined as ISM <1 mm.
Results
In both groups, ISM was the highest at 3 months and gradually decreased thereafter, and the plating group showed significantly lower serial ISM than the non-plating group at 12 months. The plating group had lower NRS and NDI scores than the non-plating group at 12 months, and the difference in the NRS scores was statistically significant, particularly at 3 and 6 months, although that of the NDI scores was not. In a multivariate analysis, plating was the most powerful predictor for fusion.
Conclusions
Plating significantly decreases the serial ISM compared with non-plating in single-level ACDF, and such decreased motion is correlated with decreased neck pain until 12 months postoperatively, particularly at 3 and 6 months. Given that plating was the most predictive factor for fusion, we recommend plating even in single-level ACDF for better early clinical outcomes.
Introduction
Stability support is a significant index of surgical outcomes in anterior cervical fusion surgeries. Anterior cervical plating, as well as well-fitted interbody grafts, has been a common augmentation procedure for ensuring stability at the operated segment [1]. Several studies have reported that plating has the advantages of decreased rates of pseudarthrosis, subsidence, and segmental kyphosis [1–4]; nevertheless, its drawbacks include higher incidences of dysphagia and adjacent segment disease (ASD) than those observed with cage and graft-alone procedures [5–7].
Some studies have reported that stand-alone anterior cervical discectomy and fusion (ACDF) was sufficiently effective for inducing fusion and have demonstrated similar fusion rates, even in multi-level cervical segments [5–16]. Moreover, reports of postoperative disadvantages associated with the presence of an anterior plate suggest that its routine use is not beneficial [17].
In terms of defining the fusion status, various fusion criteria and time points have been used, and the evaluation methods frequently differ as well [6,10]. Such inconsistencies make the comparison of published results regarding fusion status challenging and determining differences in various surgical options impossible. One of the anterior cervical fusion criteria, measuring differences in interspinous motion (ISM) on flexion and extension dynamic radiographs, is affordable in terms of cost and accuracy and is a reasonable screening tool to detect pseudarthrosis [18]. Furthermore, the ISM method has an advantage in that it can demonstrate serial changes in the degree of motion in the operated segment for some period before the time point of determining fusion. To the best of our knowledge, few studies have compared the postoperative segmental motion in the arthrodesis level from early postoperative periods to investigate the role of plating.
This study aimed to investigate the differences in postoperative serial segmental motion using ISM and clinical outcomes between plating and non-plating groups until 1 year postoperatively in patients who underwent single-level ACDF.
Materials and Methods
1. Participants
This retrospective cohort study was approved by the institutional review board of Chung-Ang University Hospital (No., C2014197). The requirement for informed consent from individual patients was omitted because of the retrospective design of this study. Consecutive 221 patients who underwent single-level ACDF from C3–4 to C6–7 at a single institute were evaluated by three spine surgeons from January 2008 to January 2018. All patients were instructed to wear a rigid neck collar for 6 weeks postoperatively. Among them, patients who underwent surgery for fractures (n=4) and infections (n=5) were excluded. Moreover, patients with unavailable serial postoperative dynamic radiographs at 3 and 6 months or 12 months postoperatively (n=37), those with ineffective dynamic radiographs (n=9), those with translation cervical plates (n=8), and those with locked cages (n=9) were excluded (Fig. 1). An ineffective dynamic radiograph was defined as one with <4 mm of ISM at the superjacent level, which means just above the operative level [18]. Finally, a total of 149 patients were enrolled and divided into the following two groups: group I patients, who underwent single-level ACDF without plating, polyetheretherketone (PEEK) cage, or graft-alone, and group II patients, who underwent single-level ACDF with plating.
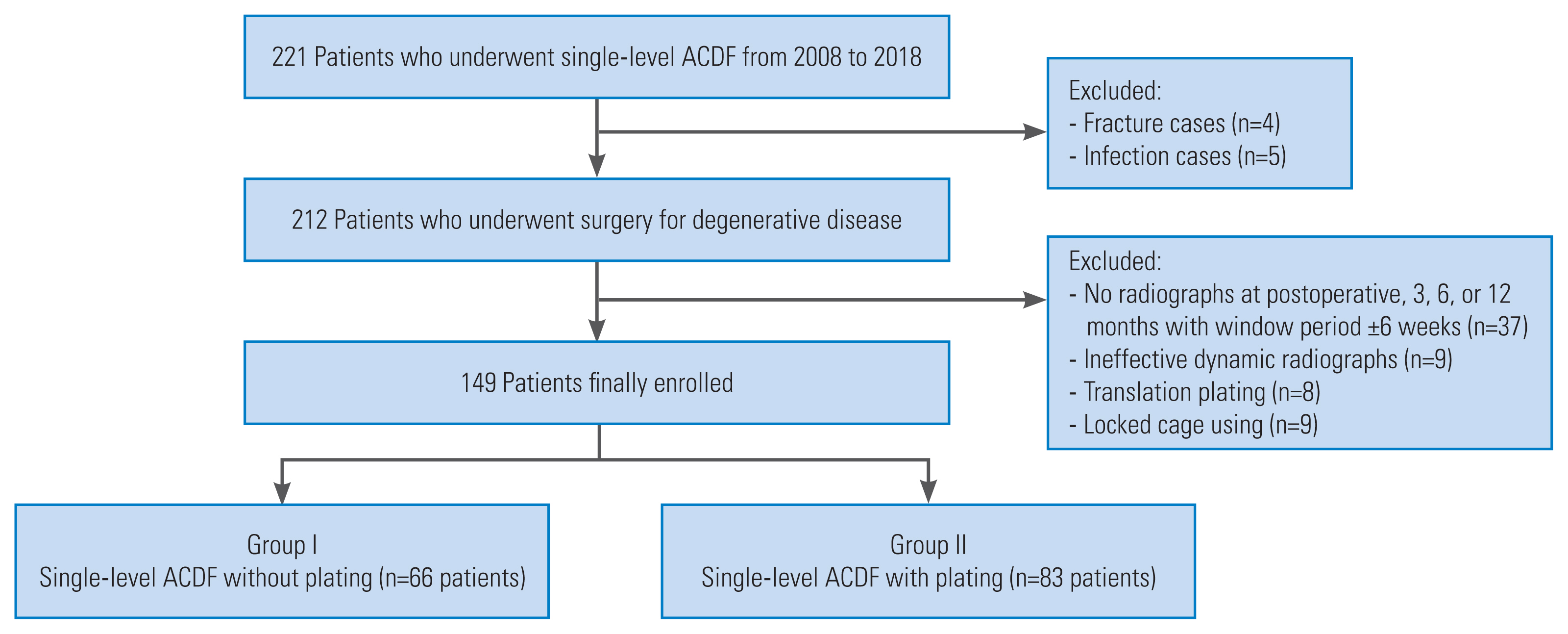
Flowchart of patient enrollment. ACDF, anterior cervical discectomy and fusion.
2. Evaluation methods
Age, sex, diabetes, smoking, diagnoses, clinical scores, and types of grafts and implants for arthrodesis were reviewed from the medical records. Diagnoses included disc disease, stenosis, and ossification of the posterior longitudinal ligament. The interbody spacers used were divided into three categories, including PEEK cage, allo-cortical graft, and auto-cortical graft. Based on the type of bone graft used in the PEEK cage void, participants with PEEK cages were further divided into the following two subgroups: allograft (demineralized bone matrix) or autograft (harvested iliac bone). The Numeric Rating Scale (NRS) for neck pain and neck disability index (NDI) were recorded at 3-, 6-, and 12-month follow-up visits.
Differences in ISM between flexion and extension lateral cervical radiographs were measured on one monitor, displaying the two radiographs simultaneously. The most identifiable landmark around the spinous process tips on flexion and extension views at the arthrodesis segment was chosen at 150% magnification, and <1 mm of ISM at postoperative 12 months was defined as fusion [18]. Radiographic measurements were independently performed by two spine surgeons (14 and 2 years of experience) at two different time points over 4-week intervals. The data used were the average of all measured values.
3. Statistics
The Kolmogorov-Smirnov test and Q-Q plots were used to test for the normality of variables. NRS and NDI did not pass the Kolmogorov-Smirnov test; however, they did not show marked deviation from linearity on the Q-Q plot. Therefore, normality assumptions were applied to the linear mixed-effects model (LMEM). Natural log transformations of the ISM were performed because the ISM did not pass the Kolmogorov-Smirnov test and showed deviation from linearity on the Q-Q plot, and these values passed the Kolmogorov-Smirnov test. Differences in NRS, NDI, and natural log-transformed ISM were analyzed using LMEM, which were made using times (preoperatively and 3, 6, and 12 months postoperatively) and groups (I and II) as independent fixed factors and individual patients as random effects.
To compare ISM at each time point, t-test using Bonferroni correction (α=0.05/4=0.0125 or α=0.05/3=0.0167) was used. Multiple logistic regression was used to identify predictive factors for cervical fusion. The multi-collinearity diagnostic indicated no multi-collinearity issues (condition indices <30; variance inflation factor values <10) between the chosen independent variables. Age, sex, and factors that had univariate p-values of <0.1 were included for multivariate analysis. Data were expressed as median (P25–P75), odds ratio (OR, 95% confidence interval [95% CI]), or absolute number (%). Data in the figures were presented as mean±standard error. The inter-observer reliability of the measurements was evaluated using interclass correlation coefficients and 95% CI. All p-values <0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic data are shown in Table 1. No significant differences between the groups regarding age, sex, history of diabetes, current smoking, diagnoses, or operative levels were noted. Regarding ISM measurement, intra-rater reliability were 0.836 (95% CI, 0.739–0.912) and 0.833 (95% CI, 0.737–0.898) and inter-rater value was 0.795 (95% CI, 0.635–0.879). Reliability values were in the excellent range.

Demographic data
1. Serial changes in segmental motion at 12 months
In both groups, Ln (ISM) was the highest at 3 months postoperatively and gradually decreased until 12 months postoperatively. Group II had significantly lower Ln (ISM) values than group I (estimated difference in means [MD], −0.63 [−1.08 to −0.17]; p=0.007) at 12 months.
In comparison at each follow-up period, group II had significantly lower Ln (ISM) values than group I in all time points (3, 6, and 12 months postoperatively) (Fig. 2). The fusion rates of the non-plating and plating groups, defined as <1 mm of ISM at 12 months postoperatively, were 35% and 64%, respectively.
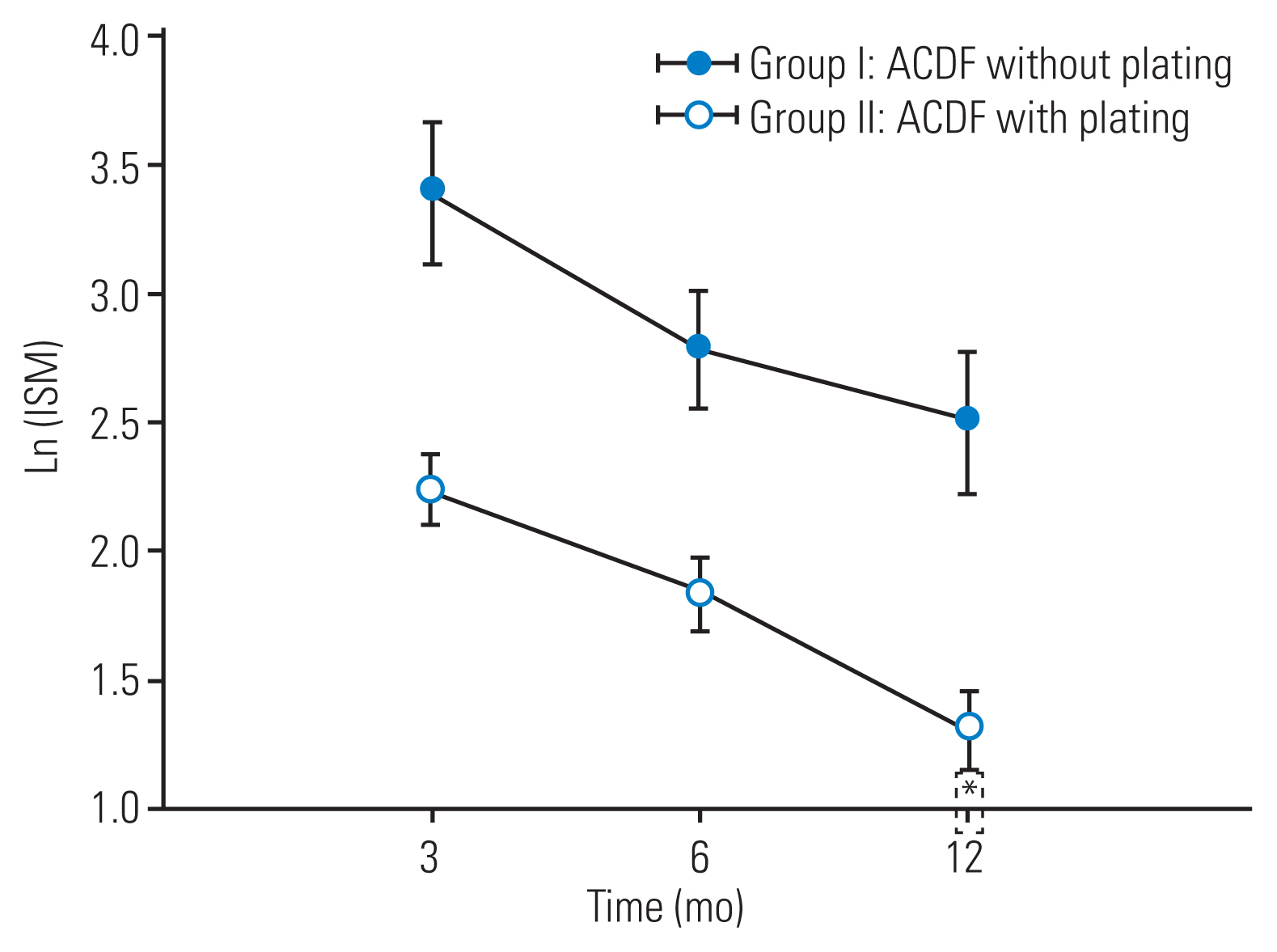
Serial change of Ln (interspinous motion [ISM]) between the groups during 12 months postoperatively. *p<0.05 compared with group I. ACDF, anterior cervical discectomy and fusion.
2. Serial changes in clinical outcomes at 12 months
In both groups, the NRS and NDI scores gradually decreased until 12 months postoperatively. The NRS scores in group II were significantly lower than those in group I (MD, −0.34 [−0.64 to −0.04]; p=0.028); however, no evidence of a difference in the NDI scores between groups I and II (MD, −1.02 [−2.78 to −0.75]; p=0.258) at 12 months was noted (Figs. 3, 4).

Serial change of the Numeric Rating Scale (NRS) between the groups at 12 months postoperatively. *p<0.05 compared with group I. ACDF, anterior cervical discectomy and fusion.

Serial change of the Neck Disability Index (NDI) between the groups at 12 months postoperatively. ACDF, anterior cervical discectomy and fusion.
In comparison at each follow-up period, group II had significantly lower NRS scores than group I at 3 and 6 months postoperatively; however, no significant difference in the NRS scores at 12 months postoperatively was noted. No evidence of difference in the NDI scores between groups I and II at each time point was noted (Figs. 3, 4).
3. Predictive factors for the fusion
Uni- and multivariate analyses of predictive factors for fusion at 12 months postoperatively are presented in Table 2. In univariate analysis, age, sex, diabetes, and smoking were insignificant; however, anterior plating and graft type showed powerful predictive values. Anterior plating showed a significant OR of 4.16 for fusion (p<0.001). Both allo-cortical (OR, 2.53; p=0.022) and auto-cortical grafts (OR, 2.23; p=0.046) showed statistical superiority compared with PEEK cage. In multivariate analysis, only anterior plating was a significant predictive factor for fusion (OR, 3.543; p=0.001). In 97 participants using PEEK cage, anterior plating was also a powerful predictive factor for fusion (univariate: OR, 3.305; p=0.002; multivariate: OR, 2.795; p=0.070). Based on bone material type used in the void of PEEK cages, autograft was a more influential factor for fusion than allograft (univariate: OR, 2.540; p=0.010; multivariate: OR, 1.164; p=0.662) (Table 3).

Uni- and multivariate analysis for fusion at postoperative 12 months

Uni- and multivariate analysis for fusion at postoperative 12 months in 97 subjects with cage
Discussion
Our results revealed that the plating group in single-level ACDF demonstrated not only significantly lower serial ISM but also lower NRS scores for neck pain than the non-plating group at 12 months postoperatively; however, no significant differences for NDI scores were noted. Regarding each follow-up time point, the differences in clinical outcomes were observed only at 3 and 6 months for NRS. These results suggest that such larger postoperative sustained motion at the operated segment adversely affects postoperative neck pain, particularly until postoperative 6 months.
If surgical outcomes between the two groups were compared at only 12 months postoperatively, as in most other studies, our results demonstrated no differences as well. Although the different result is due to different evaluation time points, we believe that comparing these sequential effects for 12 months postoperatively using LMEM may be more meaningful to demonstrate the actual differences between the groups (Fig. 5).

Representative postoperative serial radiographs for both groups. (A–C) A 66-year-old female patient who underwent C5–6 single-level anterior cervical discectomy and fusion (ACDF) with plating. The interspinous motion (ISM) gradually decreased from postoperative 3-month to 12 months. The ISM gradually decreased from 3 to 12 months after surgery and showed less than 1 mm in the last follow-up. (D–F) A 42-year-old male patient who underwent C5–6 single-level ACDF without plating. The postoperative 12-month ISM was 2.03 mm and considered a failure to achieve fusion.
ACDF is a successful surgical procedure with good clinical results and a high fusion rate [19]. Stand-alone ACDF causes less damage to adjacent structures and is associated with shorter operating times and blood loss than plating [1,10]. Several studies have reported comparative fusion rates between plating and non-plating [6–14]; however, the debate is currently ongoing. In this study, the impact of plating on suppressing segmental motion from the early postoperative period was not only correlated with better neck pain score but also resulted in a higher fusion rate (plating: 64% versus non-plating: 35%). Remarkably, in this study, the fusion rates in both groups were relatively 20%–30% lower than those reported in previous studies [1,10]. Our suggested fusion criterion, ISM <1 mm, may be considered stringent versus an ISM of 2 mm. However, careful determination of landmarks on radiographs at 150% magnification could overcome the measurement concerns and may be a tool to distinguish the overlooked difference [18].
Contrary to our findings, previous studies have reported similar fusion rates between plating and non-plating. Some studies did not provide details regarding how to define fusion; moreover, the time points of determining fusion varied from 3 months to several years postoperatively. It is debatable whether determination of radiographic fusion within 6 months is reasonable [17,20] using only bridging bone patterns on plain radiographs [8,11,13,14,16].
When evaluating graft materials as predictive factors for fusion, the PEEK cage was inferior to allo-cortical allografts (OR, 1.784) and auto-cortical grafts (OR, 1.542). Both strut grafts have better biocompatibility than PEEK cage [21]. Although auto-cortical grafts have better osteogenic potential, allo-cortical grafts provide initial strength for supporting the anterior column [22]. On analyzing the effects of different materials in the PEEK cage void, we found that the autograft showed higher OR than the allograft (Table 3).
Dysphagia and ASD are the major concerns of anterior plating over stand-alone ACDF [10]. Although higher incidences of dysphagia related to the presence of plating have been reported, several reports have also demonstrated no significant differences in the incidence of dysphagia; the mechanism of dysphagia itself is also unclear [4,23]. Furthermore, ASD is influenced by the surgical technique, graft materials, amount of fusion level, alignment, and individual lifestyle [9]. The main reason for higher ASD related to the presence of plating could be the proximity or surgical insult to an adjacent segment, both of which are related to the surgical technique and appear to be preventable. Furthermore, stand-alone ACDF is associated with more subsidence and loss of cervical lordosis than anterior plating ACDF [1,24]. These adverse effects could affect the progression of ASD.
This study had some limitations, particularly in terms of its retrospective design. First, a large proportion of participants was excluded due to mainly unavailable serial follow-up radiographs (37/186); however, a similar lost proportion of plating (15/81, 18%) and non-plating (22/105, 20%) in single-level ACDF patients may reduce some selection bias. Second, postoperative 12 months was relatively short to evaluate the long-term effects of plating, including ASD and the revision rate, and it could be early to determine the fusion status. Further fusion progression after 1 year can occur, and the possibility that our fusion rate increase cannot be excluded. Third, ISM fusion criteria demonstrated functional stability and not anatomic radiographic bony fusion. It may be difficult to directly compare the fusion rate with that of other studies due to the absence of data on the evaluation of anatomic bridging bone in this study. However, our study aimed to evaluate the differences in the changes of serial segmental motions and clinical outcomes from early postoperative periods between plating and non-plating in single-level ACDF, and there is a consensus that 1-year follow-up period is sufficient to determine fusion [25]. Fourth, the result of postoperative dysphagia comparing plate and cage-alone groups could not be presented due to a lack of dysphagia evaluation data.
Conclusions
Considerable sustained motion at arthrodesis segments was observed at early postoperative periods, which gradually decreased in both the plating and non-plating single-level ACDF groups. However, compared with non-plating in single-level ACDF, plating significantly decreased the serial segmental motion, and such decreased motion was closely correlated with decreased neck pain at 12 months postoperatively, particularly at 3 and 6 months. Given that plating was the most predictive factor for fusion, we recommend anterior plating even in single-level ACDF for better early clinical outcomes.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conceptualization: KSS; data curation: CWJ, JL, SWP; formal analysis: HK, YBK, KSS; visualization: YBK, DG C, DWH; writing–original draft: KSS; writing–review & editing: KSS.