Introduction
Primary spinal cord tumors (PSCTs) include intradural intramedullary tumors developing from the cellular elements of the spinal cord, as well as intradural extramedullary tumors such as schwannomas and meningiomas, that do not originate from the cord [1]. Extramedullary tumors are formed from peripheral nerve roots or their membranes and are not part of the central nervous system (CNS), whereas intramedullary tumors originate from glial and support cells of the spinal cord. In this meta-analysis, the term “PSCT” will be used to designate all intramedullary and extramedullary (intradural and extradural) pathologies within the spinal canal arising from glial cells and supporting cells [2].
PSCTs account for about 4%–8% of tumors that occur in the CNS. They are more common in adults than in children (mean age=51 years) and are often benign [3]. When the tumor causes compression of neural structures, damage to the spinal cord and spinal roots occurs. The most common histological types of PSCT are meningiomas, schwannomas, and ependymomas [3]. Surgical resection remains the primary curative option for PSCT [1].
Laminectomy (LE) is the most widely used procedure for removing PSCTs [4,5]. However, LE may be associated with segmental instability, postoperative spinal deformity (kyphosis and scoliosis), and epidural scar formation; as a result, a high frequency of reoperations is observed [5–8].
Laminoplasty (LP), which can be considered as an alternative to LE in PSCT, is popularized by Japanese orthopedic surgeons for posterior decompression in degenerative cervical myelopathy. There are more than 20 variations of LP. The most commonly used LP techniques are modifications of the open-door LP (developed by Hirabayashi and colleagues in 1977) and the double-door LP (described by Kurokawa and colleagues in 1982) [5]. LP allows access for tumor removal, followed by restoration of the spinal ring (when mini-plates of grafts are used) and provides a dorsal roof for the spinal cord [4,5].
Despite the benefits of LP, it has not yet been widely accepted by the neurosurgical community and has not become the gold standard treatment for PSCT. The lack of information on the efficacy of LP in the treatment of PSCT, as well as contradictory data comparing LP with LE, was the motivating factors for this meta-analysis.
This meta-analysis was conducted to systematically compare the safety and efficacy of the two posterior approaches for PSCTs of adult patients (LP versus LE) to address limitations in the current literature.
Methods
1. Design, data sources, and searches
This review followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [9] guidelines and AMSTAR (A Measurement Tool to Assess Systematic Reviews) 2 [10] appraisal tool. A systematic search was conducted through MEDLINE via PubMed, Cochrane Library, EMBASE, and Google Scholar databases. A highly sensitive search strategy using the keywords “laminoplasty” and “spinal tumor” or “primary spinal cord tumor” or “oncology” or “extramedullary tumor” or “intramedullary tumor” or “intradural tumor” was performed. A broad search strategy using only the keyword “laminoplasty” was also performed. Irrelevant studies were excluded and duplicates were removed. Only original articles from 1980 to 2021 were selected. Additional references were found by manually searching literature lists of relevant studies, conference abstracts, registered clinical trials, and by contacting experts in the field. The search was limited to publications in English.
2. Study selection
All the articles were selected using the previously stated keywords. The data were selected independently by two authors (R.P., A.K.), who checked all relevant titles and abstracts of publications to exclude irrelevant ones. Researchers independently evaluated full reports, after which each selected article was independently evaluated by the entire author team using the PICOS (Population, Intervention, Comparison, Outcome, Study Design) [11] inclusion and exclusion criteria (Table 1) [12].
3. Data extraction and quality assessment
Data were extracted independently by two reviewers (R.P. and A.K.). The data included the following: study design, patients (age, sex, and tumor type), type of surgery (LP and LE), LP technique, clinical (clinical scales, complications, blood loss, and operation time), and radiological outcomes (postoperative kyphotic deformation). As all studies included were nonrandomized controlled retrospective studies, the Newcastle-Ottawa Scale was used to assess the quality of each study [13].
4. Outcomes measures
The study analyzed the following data primarily: (1) operation time, (2) hospital stay, and (3) complications. The incidence of postoperative spinal deformity, which was defined as loss of cervical or lumbar lordosis, appearance or worsening (>10° Cobb angle) of cervical or thoracic kyphosis, or new appearance or worsening of scoliosis were also analyzed.
5. Statistical analysis
Review Manager ver. 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark) was used for data analysis. Risk ratio (RR), odds ratio (OR), and 95% confidence interval (CI) were calculated for dichotomous variables; standardized mean differences (SMD) and their 95% CI were used for continuous variables. The degree of heterogeneity was assessed using the I2 coefficient. A fixed-effects model was used for no heterogeneity, and a random-effects model was used if I2 was more than 40%. A funnel plot was constructed and the Egger test was performed to assess publication bias. A p-value <0.05 was utilized to indicate statistical significance.
Results
1. Systematic search results
Fig. 1 shows a summary of the study selection process. A total of 2,717 articles were identified through MEDLINE, Cochrane Library, EMBASE, and Google Scholar databases. A total of 2,631 studies were excluded as they were duplicates, irrelevant studies, case reports, and review. A total of 86 potential articles were retrieved for further full-text evaluation. Among them, 61 articles were excluded for not meeting the inclusion criteria. Finally, 25 studies were included in the qualitative synthesis and seven studies with 540 patients were included in this meta-analysis. Table 2 summarizes the main characteristics of the included studies [14–38].
2. Baseline characteristics and quality assessment
Seven studies were included in this meta-analysis. These studies were published between 1996 and 2021. The number of patients in the LP and LE group was 194 and 346, respectively. As all studies were retrospective nonrandomized studies, the Newcastle-Ottawa Scale was used to assess the quality. The quality of each study was low and medium (Table 2).
3. Clinical evaluation
1) Operative time
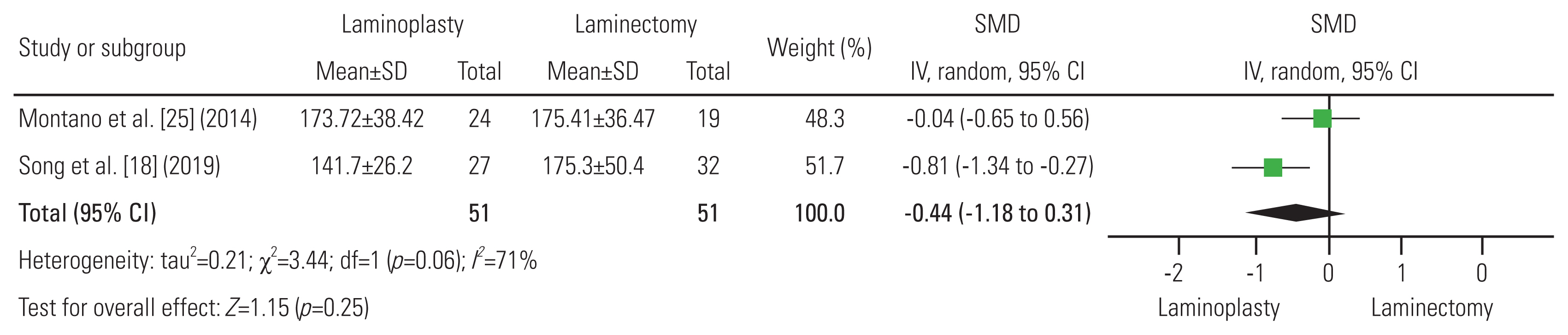
Operative time was analyzed in two studies (51 patients in the LP group and 51 patients in the LE group) [18,25]. Both groups showed similar operative times (SMD, −0.44; 95% CI, −1.18 to 0.31; р=0.25; I2=71%; random-effect model) (Fig. 2). The average operative time was 157.71 minutes in the LP group and 175.3 minutes in the LE group.
2) Hospital stay
Four studies reported information about hospital stay of LP (n=128) and LE (n=254) [18,23,25,29]. The LP group showed shorter hospital stays (SMD, −0.68; 95% CI, −1.03 to −0.34; р=0.0001; I2=48%; random-effect model) than the LE group (Fig. 3). The average hospital stay was 7.8 days and 11.3 days, in the LP and LE groups, respectively.
3) Complications
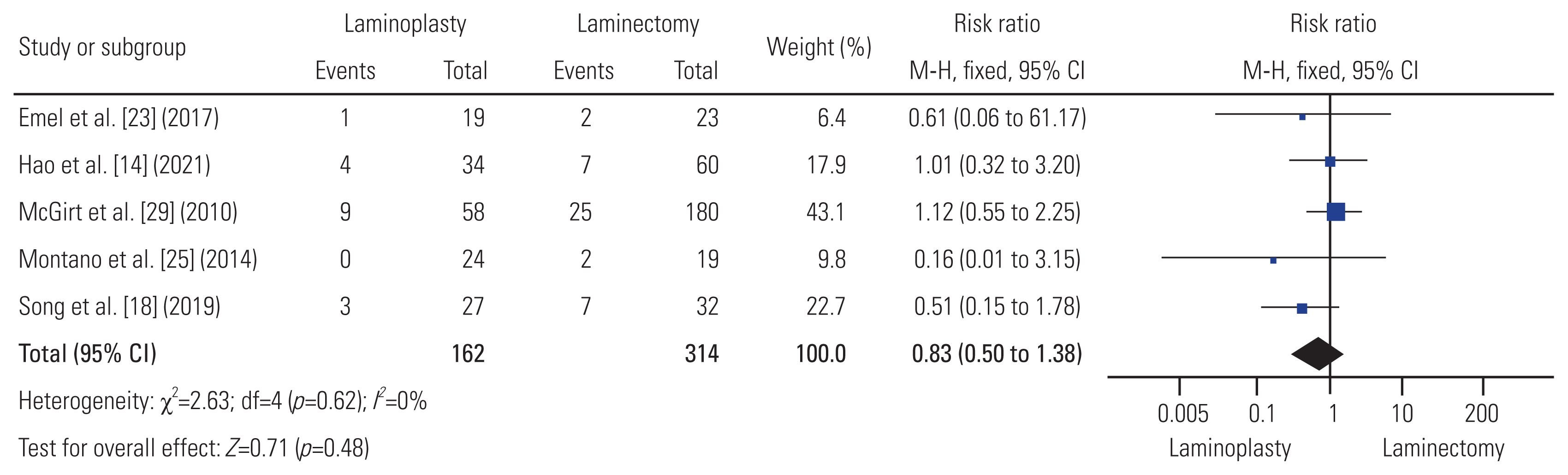
Five studies reported complications after LP (n=162) and LE (n=314) [14,18,23,25,29]. There were 17/162 (10.4%) complications in the LP group and 43/314 (13.6%) in the LE group. Total complications were similar between the two groups (RR, 0.83; 95% CI, 0.50−1.38; р=0.48; I2=0%; fixed-effect model) (Fig. 4).
4. Radiographic evaluation: postoperative spinal deformity
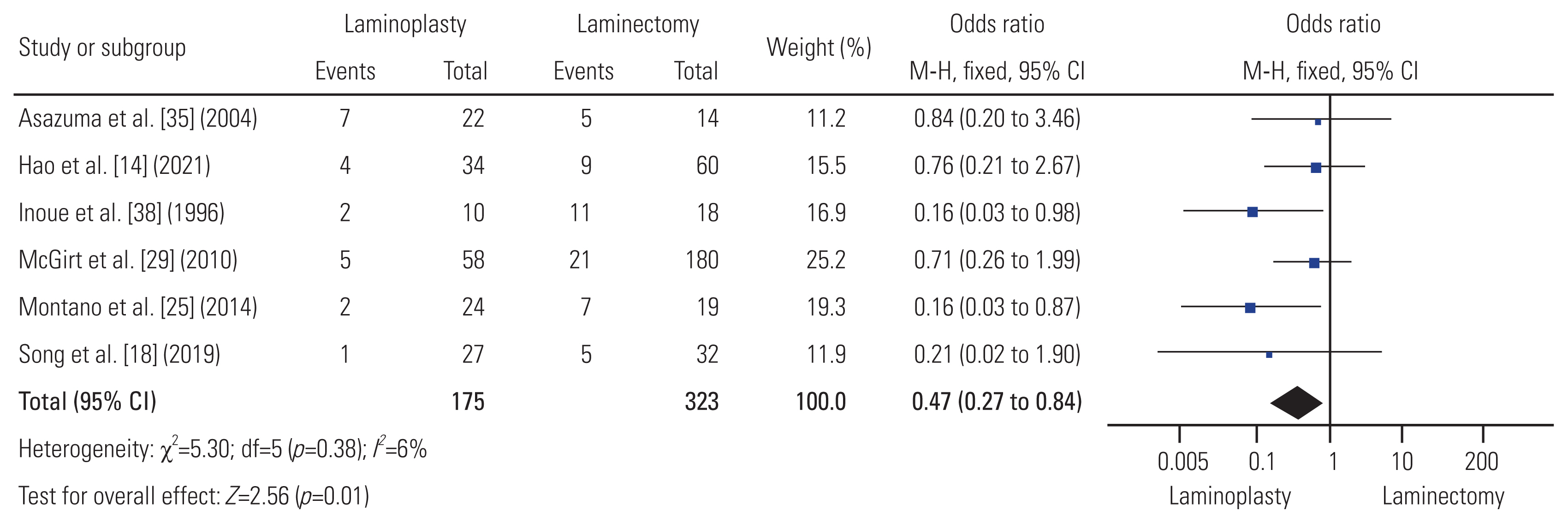
Postoperative spinal deformity rate was analyzed in six studies [14,18,25,29,35,38]. The overall rate of postoperative spinal deformity was statistically significantly lower (OR, 0.47; 95% CI, 0.27−0.84; р=0.01; I2=6%; fixed-effect model) in patients who underwent LP (21/175 [12%]) than in those who underwent LE (58/323 [18%]) (Fig. 5).
5. Publication bias
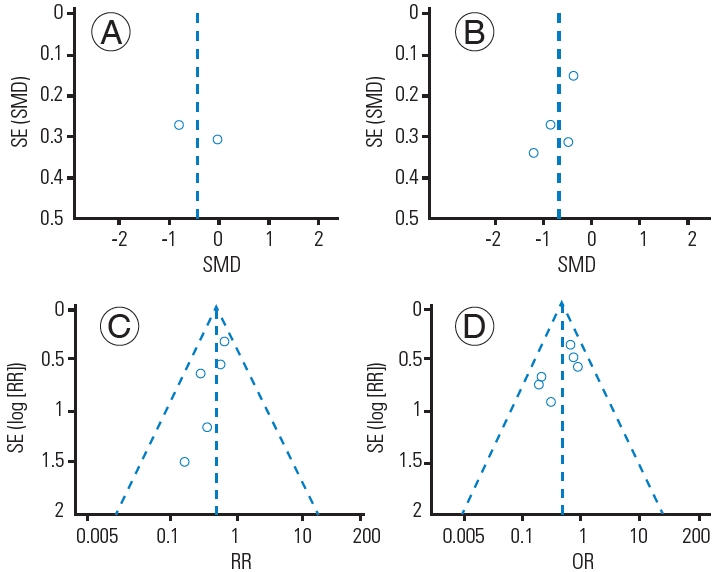
Assessment of publication bias for each parameter of the included studies was performed by funnel plots on visual inspection. The studies were nearly symmetrically distributed on both sides of the vertical line, indicating a relatively small publication bias (Fig. 6). However, there were fewer than 10 studies in the meta-analysis and the test power was too low to distinguish chance from real asymmetry.
Discussion
The LP technique was developed for the purpose of decompressing the spinal canal for degenerative and inflammatory conditions, while retaining the dorsal structures [5]. The spinal cord remains exposed following LE, whereas the spinal ring can be recreated fully and the spinal cord can be covered with LP. LP has not been widely used in PSCT surgery, where the canal itself is usually not narrowed relative to the spinal cord once the tumor has been removed.
Most scientific papers suggest that the resection of ligaments, facet joints, and laminae is accompanied by an increase in the range of motion (ROM) and a decrease in the stability of the operated segments [39]. Healy et al. [40], when analyzing the biomechanics of open-door LP, demonstrated that LE, as compared to LP, led to a relatively greater increase in global cervical ROM. An increase in segmental ROM may be a factor in the occurrence of postoperative pain syndrome and the risk of postoperative spinal deformity. Subramaniam et al. [41] noted, using cadavers, the advantage of LP over LE in maintaining spinal stability: ROM after LE was 13% greater than after LP. Despite ample evidence from biomechanical studies [42], including those using computer modeling and finite element analysis [43], the results of the clinical use of LP in PSCT surgery remain uncertain. This may be because of the wide variety of LP techniques in PSCT surgery, which is supported by the data from published studies included in our systematic review. The literature lacks definitive information on several aspects of using LP for PSCT surgery, including the adequacy of intraoperative visualization of and access to the tumor, the ability to resect the entire mass, the size of the mass that can be resected, the postoperative clinical and radiological results.
In the present meta-analysis, patients in the LP group had significantly shorter hospital stays compared to LE. The exact reasons are not clear, but it may be conjectured that reconstruction of the posterior elements somehow results in a decrease in postoperative pain, or an improvement in neurological symptoms, allowing early mobilization. The reason needs to be investigated in prospective studies with sufficient power, using validated clinical scales and measuring the time of mobilization for the two groups.
A statistically significantly lower incidence of postoperative spinal deformity in the LP group was found as compared to the LE group. This may be caused by the restoration of the posterior elements, to which extensor muscles can attach and pull. Spinous processes elevate the extensor mechanism away from the center of rotation of the spine, thereby increasing the biomechanical moment arm of the pulling force. In contrast, with LE, the extensor mechanism has nothing to attach to and, without spinous processes to hold it up, it is functionally elongated, increasing the risk of postoperative spinal deformity. The findings of the present study were consistent with the results of the series by McGirt et al. [29] with a follow-up period of up to 2 years, where the advantage of LP was confirmed: Following LP versus LE, 5 (9%) versus 21 (12%) patients developed progressive deformity (p=0.728) at a mean of 14 months after surgery. A thorough assessment of all factors that influence the deformity is needed: the degree of facet joint resection, the number of levels of decompression, the severity of the initial degenerative changes, the presence of preoperative spinal instability, systemic diseases of the connective tissue, etc. Additional studies are required to know the biomechanical features and reconstructive nature of LP for the prevention of postoperative spinal deformity.
There were no statistically significant differences between the groups with respect to the duration of surgery and the risk of postoperative complications. This suggests that LP may be advantageous, since it restores the vertebral structures following tumor removal, but it is not associated with an increased risk of complications or significantly increased operative times. In five of the retrospective studies, all postoperative complications were identified without specifying which ones were related to LP or LE. Likewise with perioperative complications, most studies failed to specify which complications were associated with LP versus LE groups.
To date, there is a single meta-analysis by Sun et al. [44], which is devoted to the subject of this study. The authors evaluated 16 studies with a total of 1,096 patients with PSCT treated with LP or LE. Statistically significant differences were noted between both groups in terms of effective recovery rate (p=0.003), blood loss (p<0.00001), hospital stay (p=0.006), postoperative spinal deformity (p=0.01), and cerebrospinal fluid leak (p<0.00001). However, there were no significant differences in the total resection rate of tumors (p=0.21) and operative time (p=0.14). In a subgroup analysis, the results indicated that age, type of tumor, follow-up period, surgical levels, and methods were associated with an increased incidence of postoperative spinal deformity [44]. Despite the seemingly clear advantages of LP over LE, a meta-analysis by Sun et al. [44] has a number of significant methodological problems. First, the final synthesis included both children and adults. The efficacy of LP in the pediatric population is well known and confirmed in studies with long follow-up [29,45,46], which could significantly bias the results in favor of LP when clubbing adults and children together. The present study, therefore, considered to evaluate LP in adult patients. Secondly, a meta-analysis by Sun et al. [44] included a large number of clinical studies written in Chinese, which complicates methodological evaluation and analysis of primary texts that are not in the public domain. Thirdly, the authors did not include a number of studies that the present study used as search strategy that met their inclusion criteria [14,18,23,35,38]. This indicated that their systematic search and selection of papers were incomplete. This study was unable to conduct a meta-analysis on many parameters because of lack of sufficient data, in contrast to the work of Sun et al. [44], where the advantages of LP are more definitively identified.
If the significant number of methodological shortcomings in the design of the included publications were considered, this study results indicate the need for further research aimed at the clinical and radiological efficacy of LP in PSCT surgery in adults. The published series could not analyze the most advantageous method based on the exact location of the tumor.
There are several fundamental limitations to this study. First, it concerns the design of the studies included in the meta-analysis. There are no prospective randomized trials on this topic. All the included studies were of a retrospective observational nature with no blinding procedure. There are many biases including selection bias, attrition bias, reporting bias, and other systematic and random errors. Second, a small number of subjects in each of the studies, or lack of data, confounded our statistical analyses, although this was partially mitigated by the meta-analysis itself. The CI for postoperative spinal deformity crossed the central axis in many studies. There was no distinction between the occurrence of postoperative kyphotic and scoliotic deformities. Therefore, a general term “postoperative spinal deformity,” was used in this study that included both scoliosis and kyphosis cases. Assessment of deformity in degrees was presented only in one paper, which precluded us from presenting a meta-analysis of the degree of deformity for both groups. Although hospital length of stay was statistically significant, there was a fairly high degree of heterogeneity (I2=64%). Significant variation, and, in some cases, the lack of necessary data, precluded us from performing a meta-analysis on parameters such as blood loss, total resection rate, etc., as the effectiveness of LP using validated clinical scales such as McCormick, Japanese Orthopaedic Association, 36-item Short Form Health Survey, Visual Analog Scale, and so forth. A number of studies had high heterogeneity within groups. For example, Song et al. [18] included patients who underwent LE with instrumented arthrodesis, instead of putting them into a separate subgroup. Tatter et al. [15] reported no details regarding postoperative kyphotic deformity, only two cases required revision stabilization. All of the above discrepancies likely affected our analyses of the duration of surgery, hospital stay, the frequency of postoperative complications, and the risk of postoperative spinal deformity. Third, the inclusion of studies performed on different regions of the spine in the meta-analysis is an important limitation when determining the incidence of postoperative spinal deformity. The incidence of deformity is highly dependent on the spinal region; in our opinion, combining all data without taking this factor into account introduces significant biases and complicates the unambiguous interpretation of the meta-analysis. Finally, another potential limitation of this study is that it only analyzed studies published in English.
Conclusions
The study revealed significant advantages of LP compared to LE in PSCT surgery. The LP procedure had a shorter hospital stay and a lower incidence of postoperative spinal deformity, with comparable operative times and surgical complications. The advantages of LP include prevention of adhesion of the dura to the paravertebral tissues, reconstruction of the dorsal roof of the spinal canal, and restoration of the spinal ring. It also results in early mobilization, a faster return to previous physical activity, and, likely, a lower risk of postoperative spinal deformity. If our analysis would be verified with future studies, we believe that LP should be adopted as the approach of choice for PSCT surgery, since it retains normal anatomy and is less invasive than LE [47].
Clinical trial data obtained from meta-analyses are highly susceptible to biases because of small sample sizes and the retrospective nature of the studies. Therefore, it is necessary to conduct large, prospective, randomized clinical trials with long-term follow-up, using a uniform LP technique to preserve the original spinal canal diameter, to improve the methodological quality of studies, as well as to objectively compare LP to LE.