Absolute Bed Rest Duration of 3 Days for Osteoporotic Vertebral Fractures: A Retrospective Study
Article information

Abstract
Study Design
Retrospective case-control study.
Purpose
To reduce unnecessary absolute bed rest (ABR), this study sought to determine the optimal aimed length of ABR in older patients getting conservative treatment for osteoporotic vertebral fractures (OVFs).
Overview of Literature
OVFs are quite common in elderly patients. ABR is a vital part of conservative treatment for OVFs, although the length of ABR may increase patient. No recommendations regarding how long ABR should last.
Methods
This study was conducted in 134 patients with OVFs initially treated conservatively. The patients were split into two groups: 3-day and 7-day ABR. From the time of injury to 1, 4, and 12 weeks after injury, compression rate (CR) and local kyphotic angle (LKA) were assessed and compared between the two groups. Any complications such as pneumonia, deep vein thrombosis, delirium, and urinary tract infection known to be related to ABR were examined based on the electronic medical record.
Results
Forty-four patients underwent ABR for 3 days and 90 underwent ABR for 7 days. There was no significant difference in CR and LKA between the two groups at the time of injury versus 1, 4, and 12 weeks after injury. The patients were divided into two groups: those who received a 3-day ABR and those who received a 7-day ABR. CR and LKA were measured and compared between the two groups from the time of damage to 1, 4, and 12 weeks after injury. The ABR-related complication rate was 43.4% in the 7-day ABR group and 22.7% in 3-day ABR group (p=0.02). The duration of hospital stay was significantly shorter in the 3-day ABR group (12.8 days) than in the 7-day group (16 days) (p=0.01).
Conclusions
Considering radiological outcomes, prognosis, complications, patient convenience, and economic impact, a 3-day ABR period is appropriate for the conservative treatment of OVFs.
Introduction
Osteoporotic vertebral fractures (OVFs) are common in the elderly [1–3]. OVFs commonly occur after minor falls and can cause back pain and spinal deformity if not properly treated [2]. In Korea, the number of OVFs is increasing every year, with a total national cost of 66,183 million won for insurance-covered services in the year after OVFs in Korean women 50 years old between July 2002 and 2004 [4,5]
OVFs may be treated conservatively or surgically [3]. In most cases, patients with no neurological symptoms are treated conservatively with a period of absolute bed rest (ABR) followed by the use of a brace [1,2]. However, research is scarce on the best ABR length [6,7]. Because OVFs are more common in the elderly population, consequences from extended ABR should be considered [8]. These include pneumonia, bedsores, deep vein thrombosis (DVT), cerebral infarction, urinary tract infection (UTI), and sarcopenia. Furthermore, even a little period of ABR may limit daily activities and hygiene, and no studies have shown that prolonged ABR periods are useful in the conservative treatment of OVFs. A study by Cha et al. [9] compared and analyzed 1-week versus 2-week ABR groups in Korea and found no significant differences in radiologic changes or clinical results between the two groups, concluding that the 2-week ABR group experienced more complications and discomfort [9].
However, in the authors’ clinical experience, ABR intervals of less than 1 week are poorly tolerated in many older patients, and ABR times of less than 1 week tend to be more successful in patients with OVFs. A recent study found that just one week of bed rest caused significant muscular atrophy and whole-body insulin resistance [10]. Furthermore, osteogenesis stops during ABR, resulting in bone loss and osteopenia. Nigam et al. [11] reported that after a few days of bed rest, plasma calcium levels increased, and by the third day, urinary calcium losses increased considerably. Given the foregoing, the previously indicated ABR duration of 7 days may be troublesome. This study looked into the optimal duration of ABR in elderly individuals getting conservative treatment for OVFs in order to minimize unneeded ABR and its accompanying problems.
Materials and Methods
1. Study design and participants
The institutional review board of Ilsan Paik Hospital gave its clearance to this retrospective investigation. This study comprised a total of 208 patients who were treated for OVFs at our center between December 2016 and November 2019. These patients were treated with ABR first, then with a custom-made brace (thoracolumbosacral orthosis [TLSO] or lumbosacral orthosis [LSO]). All procedures were carried out in compliance with the Helsinki Declaration and the ethical requirements of Ilsan Paik Hospital Research Committee (IRB no., 2021-05-044-002). The patients signed a written informed consent form.
OVFs were defined as fractures caused by low-energy trauma equivalent to a fall from a standing height in adults, and were not based on bone mineral density (BMD) [12].
The inclusion criteria were as follows: (1) patients aged ≥50 years; (2) acute back pain caused by OVFs; (3) OVFs limited to anterior or middle column; (4) patients who underwent brace treatment as primary treatment for OVFs; (5) patients who underwent computed tomography or magnetic resonance imaging to diagnose OVFs; and (6) patients followed up for at least 12 weeks after injury.
Exclusion criteria were as follows: (1) patients who did not have regular X-ray imaging follow-up; (2) malignant compression fracture; (3) OVFs with neurologic compromise requiring surgery; (4) OVFs with severe kyphotic deformity (kyphotic angle 30°) requiring surgery; (5) patients who had previous surgery or injury at the fractured level; (6) patients who were bedridden prior to OVFs; and (7) patients without BMD data.
We split patients with OVFs into 3-day and 7-day ABR groups since the custom-made TLSO or LSO brace normally takes 3 days to arrive. Patients were allocated to each group based on their attending physicians’ discretion without any specific criteria.
2. Treatments
During ABR, patients were instructed to lie supine in bed, without head elevation. Rolling from side to side in bed, and eating while lying on one side was permitted. To prevent vertebral body collapse, standing up to use the toilet was forbidden. As a result, during ABR, all basic activities such as feeding, maintaining physical hygiene, and toileting had to be done in bed. All patients were required to wear graduated compression stockings to prevent DVT. Chemical prophylaxis for DVT was not used because the patients did not want to have surgery. Patients wore braces and utilized analgesics as needed after completing ABR. Furthermore, patients were advised to restrict spine movement and heavy lifting during the first 12 weeks. Patients who did not respond to conservative treatment were in excruciating pain or had no improvement in clinical symptoms had cement augmentation surgery. Patients experiencing prolonged pain from nonunion, kyphosis progression, or spinal cord compression were also given fusion surgery.
3. Patient assessment
BMD was measured in all patients within 1 year after injury. In addition, radiographs (anteroposterior and lateral views) were taken at the time of injury and at 1, 4, and 12 weeks after injury to track changes in the fractured spine compression rate (CR) and local kyphotic angle (LKA). Because it was difficult for the patients to stand up due to pain in the early stages, all radiographs were taken in the supine position. Typically, hard callus forms and bone remodeling is complete 12 weeks following a fracture; as a result, pain severity diminishes dramatically by 12 weeks [13,14]. As a result, radiographic follow-up was limited to 12 weeks after injury. CR was calculated as a radiological parameter indicating the degree of fractured vertebral body collapse, as follows: 100−[b/(a+c/2)]×100, where “a” and “c” represents the heights of the normal vertebral bodies one level higher and lower, respectively than the compression-fractured vertebral body, and “b” represents the height of the compression-fractured vertebral body (Fig. 1) [9,15]. The LKA of the broken vertebral body was measured between the superior and inferior endplates (Fig. 2) [15]. Most patients had one vertebral fracture. In patients with more than one fractured vertebra, CR and LKA were analyzed based on the most severely compressed vertebral body. The values were compared between the 3- and 7-day ABR groups at the time of injury, and at 1, 4, and 12 weeks after injury to evaluate the differences in the degree of CR and LKA change.

Compression rate (CR) calculation method. CR was calculated as follows: 100–[b/(a+c/2)]×100, where “a” and “c” represent the heights of normal vertebral bodies one level higher and lower, respectively, than the compression-fractured vertebral body, and “b” represents the height of the compression-fractured vertebral body.
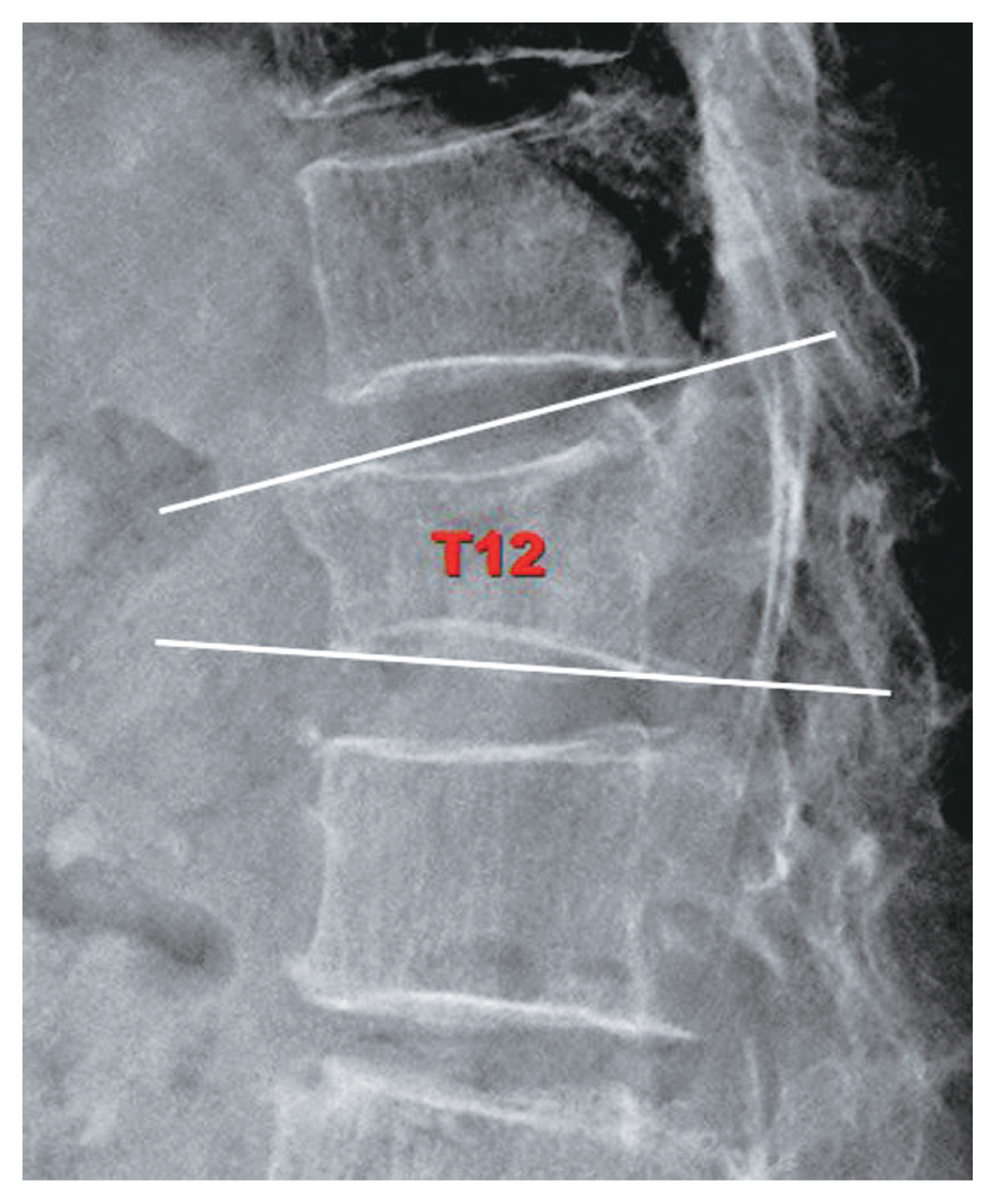
Local kyphotic angle (LKA) measurement method. LKA was the angulation between the superior and the inferior endplates of the fractured vertebral body.
Any complications such as pneumonia, bedsores, DVT, cerebral infarction, delirium, and UTI associated with ABR were examined based on the electronic medical record [8]. The authors also compared the two groups in terms of the surgical intervention rate where surgery was required due to intolerable pain, progressive kyphosis, or spinal cord compression. In addition, age, BMD, and length of hospital stay (days) were analyzed.
4. Statistical analysis
In a pilot study of 20 subjects each in the 3- and 7-day ABR groups, the average initial CR was 19 (3-day ABR group) and 25 (7-day ABR group). The required number of participants was 40 per group when the standard deviation was set at 9.5, alpha 0.05, and power 80. As a result, the number of participants in each group in this study (3-day ABR group: 44 patients; 7-day ABR group: 90 patients) was deemed appropriate. The independent sample t-test, chi-square test, or Fisher’s exact test was used to determine whether there was a significant difference between the two groups. Statistical analyses were performed using IBM SPSS Statistics for Windows ver. 20.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p<0.05.
Results
Of the 208 patients selected, the following were excluded: 58 patients who did not undergo regular follow-up X-ray imaging, and 16 patients without BMD data. Finally, the study comprised a total of 134 patients (Fig. 3). After 3 days of ABR, 44 patients wore a brace, whereas 90 patients wore a brace after 7 days of ABR.
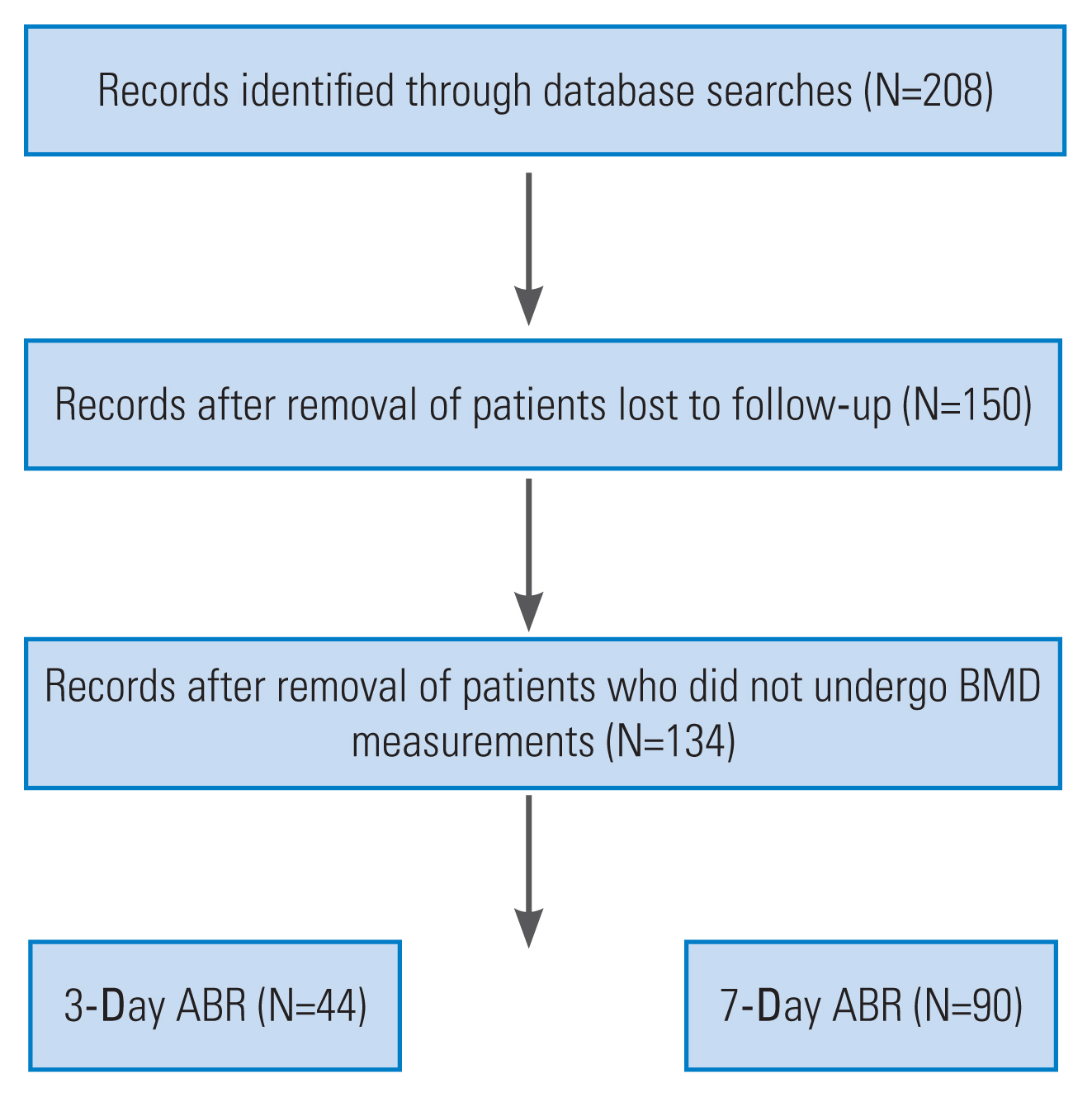
Flow diagram of participant selection. BMD, bone mineral density; ABR, absolute bed rest.
T12–L2 was the most prevalent OVF location in both groups (Fig. 4). The mean age of patients in the 3-day ABR group and the 7-day ABR group was 74.0 and 71.6 years, respectively (p=0.21). A T-score of lumbar spine BMD was lower in the 7-day ABR group (−2.02) than in the 3-day ABR group (−1.84), but this difference was not statistically significant (p=0.22). A total of 13 patients (29.5%) in the 3-day ABR group and 22 patients (24.4%) in the 7-day ABR group underwent surgical intervention, with no statistically significant difference in the surgical intervention rate between the two groups (p=0.53) (Table 1). However, the length of hospital stay was significantly shorter in the 3-day ABR group (12.8 days) than that in the 7-day ABR group (16.1 days) (p=0.01) (Table 1).
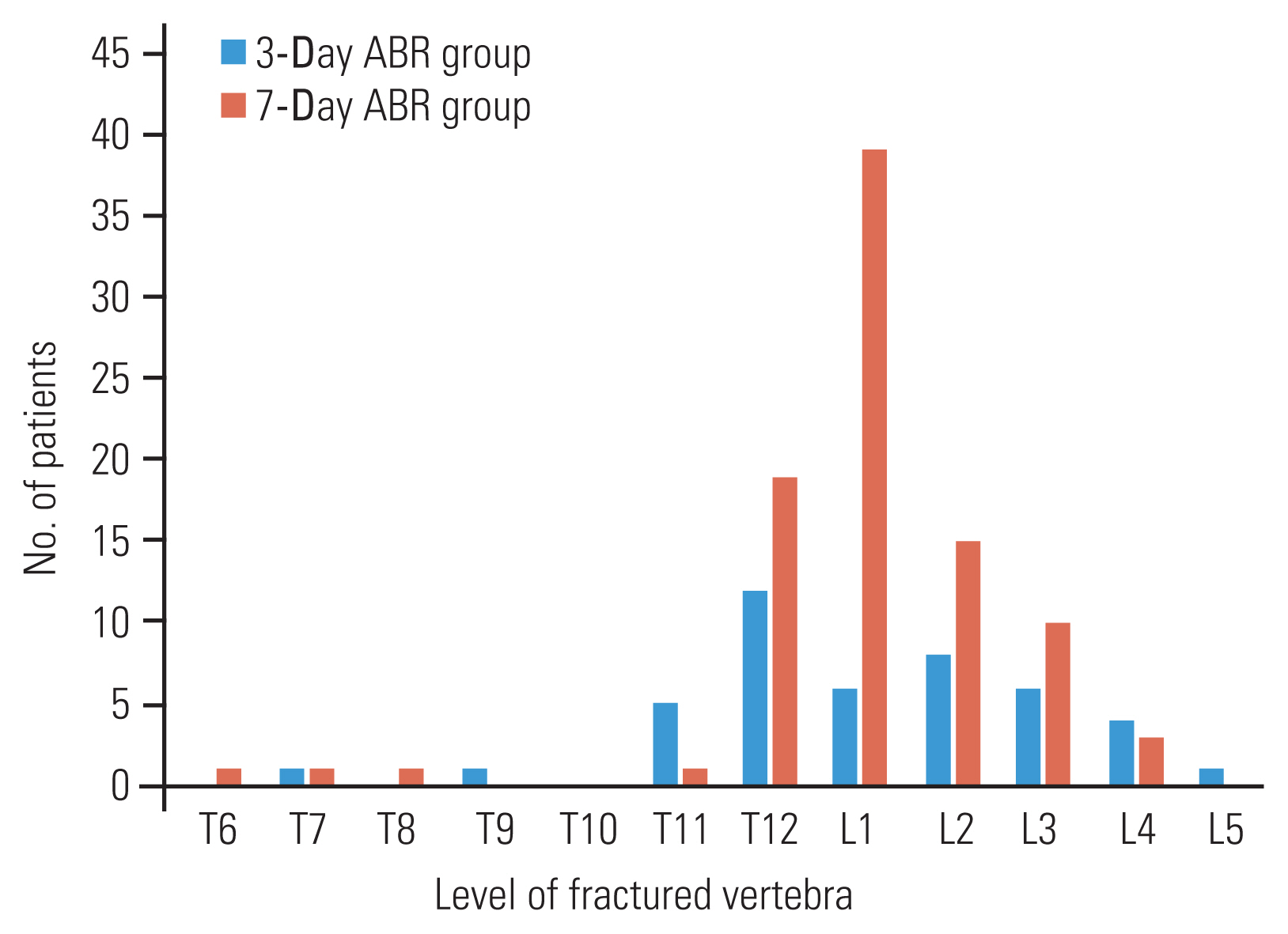
Distribution of compression fracture levels in 3-day versus 7-day absolute bed rest (ABR) groups.

Characteristic of patients in 3-day and 7-day absolute bed rest groups
The initial CR of each group was 21.4% (3-day ABR group) and 23.1% (2-week ABR group) (7-day ABR group). At 1, 4, and 12 weeks following injury, the change in CR in the 3-day ABR group was −0.6, 3.8, and 10.0, respectively, whereas the change in CR values in the 7-day ABR group was −2.2, 6.0, and 10.0, respectively (Table 2). Each group’s initial LKA was 11.59° (3-day ABR group) and 12.71° (2-day ABR group) (7-day ABR group). The change in LKA in the 3-day ABR group at 1, 4, and 12 weeks after injury was −1.17, 2.12, and 3.87, respectively, with the change in LKA values in the 7-day ABR group being −1.01, 2.01, and 3.98, respectively (Table 3). In both groups, CR and LKA decreased at 1 week after injury and continued to worsen until 12 weeks after injury. However, there was no significant difference in CR and LKA between the two groups at the time of injury or at 1, 4, and 12 weeks after injury (Tables 2, 3).

Comparison of the compression rate of fractured vertebra in 3-day ABR and 7-day ABR groups

Comparison of the local kyphotic angle of fractured vertebra in the 3-day and 7-day ABR groups
Complications from ABR were reported in 10 patients (22.7%) in the 3-day ABR group and 39 patients (43.3%) in the 7-day ABR group, with UTI being the most prevalent, followed by delirium. The number of patients with UTI was substantially higher (26 individuals) in the 7-day ABR group than in the 3-day ABR group among the other sequelae (five patients). Other consequences, such as pneumonia, pressure ulcers, psychosis, sleep disturbances, and constipation, did not differ significantly between the two groups. There were no DVT cases among the patients (Table 4).

Comparison of the ABR-related complications between 3-day ABR and 7-day ABR groups
Discussion
In the context of increasing demand for advanced medical services, this study attempted to investigate alternative conservative treatment methods for OVF that are more efficient and convenient for patients. We found no significant difference between the 3-day and 7-day ABR groups pertaining to the degree of change in CR and LKA. Regardless of the duration of ABR, the degree of fractured vertebra collapse over time was similar between the 3-day and 7-day ABR groups. In addition, there was no significant difference between the 3-day and 7-day ABR groups in terms of surgical intervention rate and the complication rate related to ABR was significantly lower in the 3-day ABR group than in the 7-day ABR group.
In the absence of severe CR, conservative treatment of OVF using a brace following ABR is acceptable. Patients undergoing ABR are unable to stand up to use the restroom and must eat while lying down, which is difficult and inconvenient. Patients frequently complain about these specific inconveniences during OVF treatment, rather than the complications associated with prolonged ABR. The current study was carried out in the Republic of Korea, where healthcare is provided through the national health insurance system. As a result, the financial burden placed on patients during hospitalization is relatively light. Nevertheless, most patients found ABR difficult and preferred to ambulate quickly and return to their previous lifestyle.
As discussed earlier, the study of Cha et al. [9] demonstrated the acceptability and benefits of 1 week of ABR over 2 weeks of ABR. In a study of Vorlat et al. [16], which utilized an ABR duration of up to 3 days, the researchers investigated the correlation between the prognosis of conservative treatment for OVFs and different factors such as age, sex, body mass index, social status, education level, occupation, smoking history, health insurance, past medical history, back pain, association with injuries, fracture type, disc damage level, and sagittal index of injuries. The prognosis was found to be influenced by smoking and health insurance. However, neither the rationale for a 3-day ABR period nor the effect of 3-day ABR on clinical prognosis or radiological parameters was described in this study. Thus, based on previous research, the current minimum acceptable ABR period is 7 days [9].
Based on our study findings, we suggest that it is reasonable to further shorten the ABR duration from 7 days to 3 days since there were no significant differences in the clinical and radiological results between the two groups. In addition, the 3-day ABR group had fewer ABR-related complications than 7-day ABR group. Shortening the ABR duration and hospitalization period may benefit patients financially, and positively affect rehabilitation [17,18]. Previous research has shown that antigravity muscle groups such as the back extensor, soleus, and quadriceps muscles atrophy frequently during bed rest [19,20] and that up to 40% of muscle strength can be lost within the first week of bed rest [21]. Muscle shortening and weakness are quickly exacerbated by inactivity. Early rehabilitation may aid in preventing further muscle atrophy and strengthening the erector muscles, which support the spine [17,18]. Patients in our study wore a brace immediately after completing ABR, received in-hospital rehabilitation through early walking, and were discharged once they returned to their previous way of life. Consequently, in terms of length of hospital stay, the 3-day ABR group recovered more quickly after rehabilitation and was discharged sooner, allowing a return to normal life earlier than the 7-day ABR group.
Osteopenia is another important consideration in the recommended ABR duration. As previously stated, osteogenesis ceases during ABR, and osteoclasts resorb bone, resulting in a loss of bone density [11]. In a previous study, Creditor et al. [22] discovered that patients who were bedridden experienced 50 times faster vertebral bone loss. According to Pisot et al. [23], it takes four months to recover from the negative systemic effects of just ten days of bed rest. Hospitalization can result in an irreversible decline in functional capability and quality of life in elderly patients [24]. Therefore, when considering the detrimental effects of bed rest, the ABR period should arguably be further reduced if the patient can bear the pain and wear a brace immediately.
UTI was the most common complication associated with ABR in this study and it occurred more frequently in 7-day ABR group than in 3-day ABR group.
Shortening the ABR period can help to prevent UTI more effectively. Furthermore, there was no DVT patient in our study, which was previously linked to ABR [8]. It is thought that wearing graduated compression stockings helped prevent DVT.
Wearing a brace in addition to ABR may have played an important role in the treatment of OVF in the current study. Lumbar braces have been shown to reduce overall lower back movement as well as segmental movement in the injured region [25,26]. A previous study found that lumbar braces reduce ABR duration and allow for faster rehabilitation [27]. However, a study by Kim et al. [28] demonstrated that braces may not always be necessary in the treatment of OVF. Patients who ambulated immediately after injury without an orthosis were compared with patients using braces for 8 weeks, and the researchers found that 12 weeks after injury, the Oswestry Disability Index scores for compression fracture treatment without a brace were not inferior to those where soft or rigid braces were used. In addition, CR progression was similar among the two brace groups (soft and rigid brace) and the no-brace group [28]. However, given that the vertebral CR in our study lasted up to 12 weeks, wearing the brace for only 8 weeks is unlikely to be enough to stabilize the fractured vertebra. In addition, the study by Kim et al. [28] was limited by small sample size (<20 patients per group). Jin and Lee [29] concluded from their meta-analysis that high-quality randomized controlled trials are required to determine whether braces should be used in the treatment of OVFs. Additionally, we found that the change in CR and LKA was negative at 1 week after injury, and it was suggested that the collapsed vertebral body partially recovered because wearing a brace in the initial stage of injury was helpful in reducing the vertebral fracture and maintaining vertebral body height. Based on previous studies and our research, we believe that wearing a brace for conservative treatment of OVFs has clear advantages.
The following are the study’s limitations. For starters, the number of patients in the 7-day ABR group was twice that of the 3-day ABR group. Until early 2017, all patients with OVF in our hospital received a 7-day ABR. The experimental use of 3-day ABR was mostly used after 2018, which explains the difference in patient numbers between the two groups. A prospective study design with a random 1:1 allocation of patients to the 3-day and 7-day ABR groups is required in the future. Second, there may be selection bias between patients using TLSO and LSO. However, most OVFs occurred at the thoracolumbar junction, and TLSO was used in most cases. In addition, there was no significant difference between the 3-day and 7-day ABR groups in the type of brace used (p=0.23). Third, the radiographs taken in the supine position may underestimate the changes in CR and LKA. Patients were unable to stand up in the early stages of OVFs due to severe pain, so radiographs were taken supine. In future studies, radiographs taken in a standing position after the acute phase of OVF will be required to accurately evaluate the changes in CR and LKA. Finally, it is difficult to use a 3-day ABR period in all OVF patients. There is a need for research into the factors that influence patient prognosis following ABR. In the presence of certain risk factors, recommending surgical treatment from the start may have a positive economic and psychological impact on patients.
Conclusions
Considering radiological outcomes, clinical prognosis, complications, patient convenience, and economic impact, a 3-day ABR period is appropriate for the conservative treatment of OVFs.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Study concept and design, analysis and interpretation of data and drafting of the manuscript: Sung Tan Cho and Jin Hwan Kim; acquisition and analysis of data: Seung Joo Kim, Bum Joon Nam, Kun Woo Kim and Gyu Hyeon Lee.
Acknowledgements
We would like to thank you for Ji Yeon Lee in the Medical record office for helping to collect patient data.