Work-Related Low Back Pain Treatment: A Randomized Controlled Trial from Tehran, Iran, Comparing Multidisciplinary Educational Program versus Physiotherapy Education
Article information
Abstract
Study Design
Clinical trial.
Purpose
To compare the multidisciplinary educational program versus physiotherapy education among Iranian nurses.
Overview of Literature
Low back pain (LBP) can accompany significant occupational injuries in the nursing profession. There is no agreement on the most effective educational practice.
Methods
This study was conducted from August 17, 2014 to September 22, 2014 in Tehran, Iran. Eligible nurses with chronic mechanical LBP (n=136) were classified into an intervention group (n=66) or the control group (n=70). The intervention group received physiotherapy education for 120-minutes followed by a 120-minute health education session based on predictive constructs of social cognitive theory (SCT). The control group received the 120-minute physiotherapy education. Disability rate, pain severity and back pain prevention behavior were measured at initially and 3 months after intervention using visual analogue scale, Roland-Morris disability questionnaire and nursing low back pain preventive behaviors questionnaire.
Results
The two groups were the same in terms of all studied variables at the initiation of the study. At the 3-month follow up, predictive constructs of LBP preventive behaviors of participants in the intervention were improved (p<0.001). Significant decreases were evident at 3 months in pain severity (p=0.03) and disability (p=0.003).
Conclusions
The designed multidisciplinary educational intervention could decrease chronic mechanical LBP in nurses.
Introduction
Low back pain (LBP) is the second-leading health problem concerning disability and visits to the doctor in people under 45 years of age [1]. Musculoskeletal disorders including LBP comprise significant occupational injuries and disability within the nursing profession [1]. One research study showed that 11% of nurses quit their job because of LBP [2]. LBP is reportedly the most important reason for nurses' decisions to change their jobs [34]. Back injuries are a major cause of pain suffering, disability, high medical costs and absence from work among nurses [5].
A multidisciplinary program involving two or more targeted interventions has been reported to be successful at significantly decreasing chronic back pain, compared with a monodisciplinary approach [678]. Multi-dimensional exercise training is useful for reducing LBP by helping to alleviate fear avoidance beliefs. Excessive fear of heightened disability is an obstacle for recovery from acute, sub acute, and chronic LBP [1].
Health promotion measures in many countries create a supportive environment and can beneficially affect macroeconomic health policy [9]. However, in some countries the importance of health promotion for nurses is less recognized [10]. It appears that Iran is among the latter group.
Social cognition is an important cognitive concept recognized in recent decades as being important in the understanding of human healthy behaviors. This kind of cognition is reflexive, participatory and involves conciliatory behaviors [11]. Behavior is affected by learning, which is in turn influenced by societal models. Consequently, modifying environmental conditions, ensuring efficient self-care and improving inter-personnel relationships are among the most important methods to enhance health [12].
Social cognitive theory (SCT) provides a comprehensive and well-supported conceptual framework consisting of constructs including knowledge, outcome expectations, outcome expectancies, situational perception environment, self-efficiency, self efficacy in overcoming impediments, goal setting or self-control, and emotional coping, which can be used to understand factors that influence human behavior and the processes through which learning occurs, offering insight into a wide variety of health-related issues. Greater significance of SCT has come from its application to the design of interventions to meet important practical challenges in medicine and public health [11]. Each of the aforementioned constructs can contribute to predicting the implementation of preventive behaviors [12]. Thus, behavior can be changed through new learning experiences, guidance in the adjustment of perceptions, and support for the development of capacities [1].
In this study, SCT was used to assess preventive behaviors regarding mechanical chronic LBP. The aim was to use SCT to drive social learning [13]. The study compared the effect of a multidisciplinary educational approach based on SCT and physiotherapy with physiotherapy alone on the alleviation of chronic mechanical LBP among nurses.
Materials and Methods
This was a clinical trial. The statistical sample consisted of nurses with chronic mechanical LBP working in Mostafa Khomeini Hospital, Tehran, Iran. Eligible nurses were classified into two groups: an intervention group comprising 66 participants and a control group comprising 70 participants. Inclusion criteria were age 18 years and older and presence of mechanical LBP for more than 90 days. Exclusion criteria included spinal surgery within the past 2 years, congenital abnormalities in the spine, pregnancy, inflammation or presence of spine tumor. Questionnaires were presented to each of the participants and they were asked to complete it anonymously.
The intervention group received a physiotherapy educational program plus a health educational program based on SCT predictive constructs of emotional coping, environment, self-efficacy, and self-efficacy in overcoming impediments in the working environment. The control group received just the physiotherapy educational program. The physical therapy training session for both groups was provided by the same physiotherapist. In the 120-minute session the participants were educated regarding protecting healthy postures of vertebra while daily activities as well as appropriate back exercise training, through role-play and viewing related slides. Participants in intervention group engaged in the same 120-minute session delivered by the same physiotherapist, followed by another 120-minute session of health education in which a specialist addressed emotional coping, environment perception and self-efficacy in overcoming impediments in the working environment. The session involved preventive behaviors and exercises, group discussion, question and answer time and a motivational interview. The goal of the health education was to motivate participants to adopt healthy behaviors and practices in their work site.
Three questionnaires were used in this study. The Nursing low back pain predictor questionnaire (NLBPPQ) was used to measure predictive constructs of SCT. The development and psychometric process of this instrument as well as its' validity and reliability have been reported [14]. An established and validated visual analogue scale (VAS) was used to measure pain severity. The VAS is a psychometric response scale that can be used in questionnaires as a measurement instrument for subjective characteristics or attitudes that cannot be directly measured. When responding to a VAS item, respondents specify their level of agreement to a statement by indicating a position along a continuous line between two end-points of zero and 10 [1516].
The Roland-Morris Disability Questionnaire (RDQ) is most sensitive for patients with mild to moderate disability due to acute, sub-acute or chronic LBP. The questionnaire measures restriction or lack of ability to perform daily activities [17]. The validity and reliability of this instrument has been reported [1819].
All data were collected at the beginning of the study and at the 3-month follow-up. All comparisons between the two groups in terms of demographic characteristics were done by chi-square test. The two groups were compared in terms of SCT constructs, VAS and RMQ scale score through Student's t-test. Paired t-test was used to compare both groups before and after intervention. The Ethic Committee of Tarbiat Modares University approved the study.
Results
A total of 136 nurses with chronic mechanical LBP were studied. Sixty-six nurses received the multidisciplinary intervention program and 70 nurses received the physiotherapy educational program. Forty nine participants (74.2%) in the intervention group and fifty participants (71.4%) in the control group were female. Demographic characteristics are shown in Table 1. The mean scores of SCT predictive constructs regarding LBP preventive behaviors are shown in Table 2. All predictive factors in the intervention group were improved after 3 months (all p<0.001). Table 3 presents the mean scores of pain severity, disability, and preventive behaviors of the two groups. In the intervention group, pain severity was significantly reduced at the 3-month follow up (p=0.03) and disability was decreased (p=0.003).
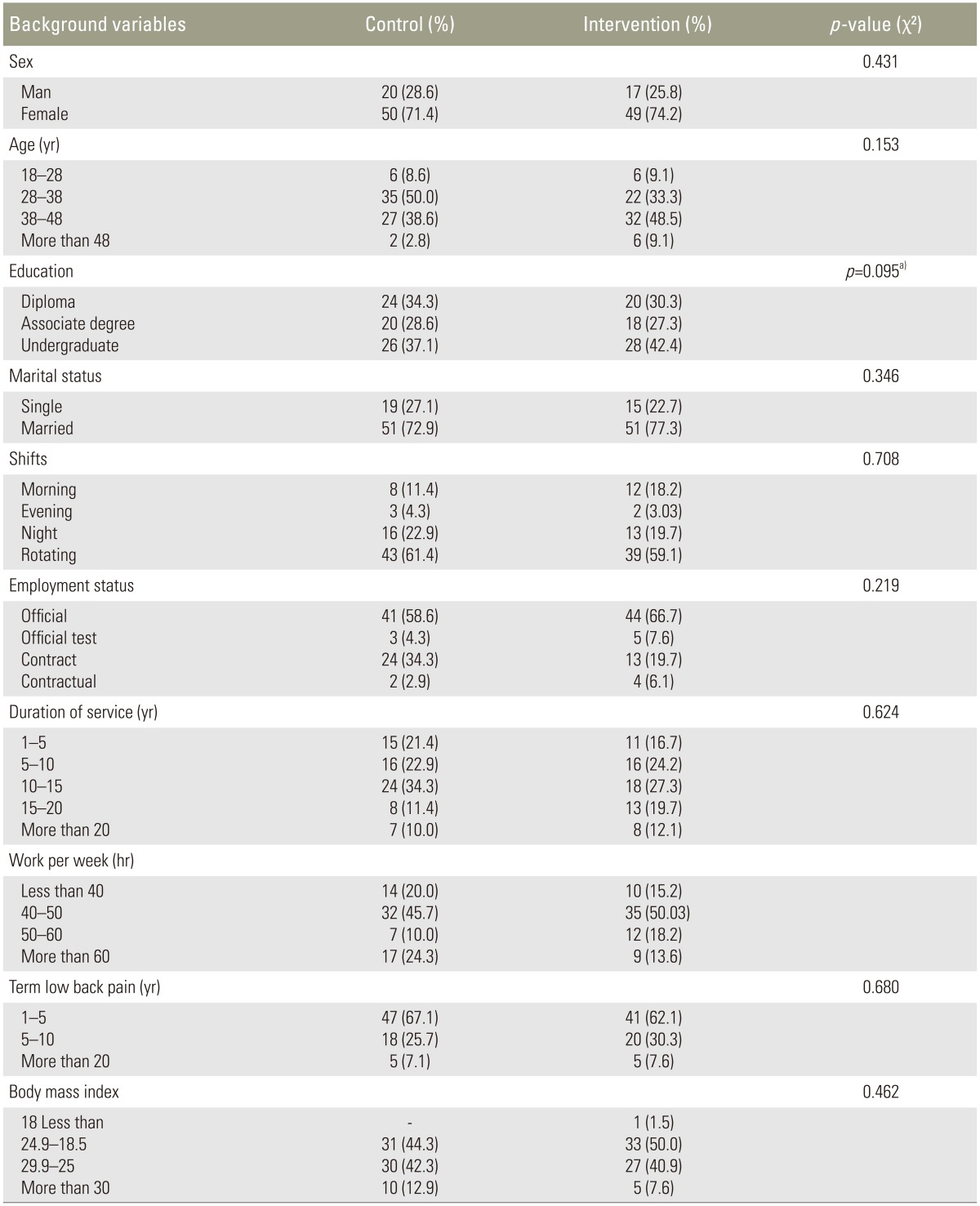
Demographic characteristics of both studied groups at initial of the study
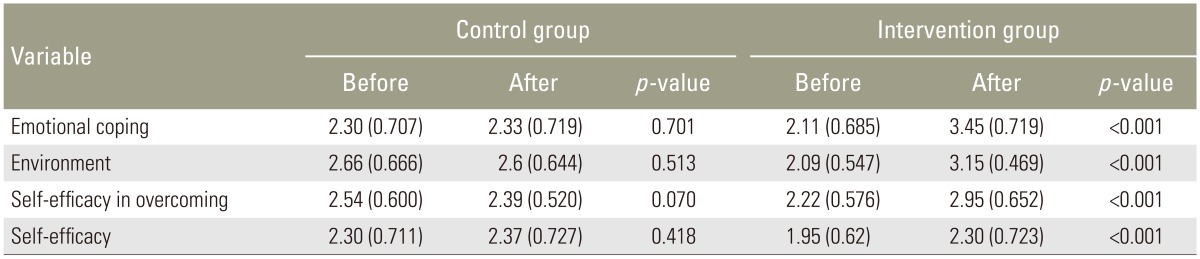
Comparing mean scores of predictive constructs in both groups at initial of the study and 3-month follow-up

Comparing preventive behaviors, pain severe and disability rate of intervention and control group at initial of the study and 3-month follow-up
Discussion
This study was conducted to compare the effects of a physiotherapy educational program alone (control) or in combination with a health educational program based on predictive constructs of SCT (intervention) on reduction of LBP severity and disability in nurses. The intervention program significantly reduced pain severity compared with the control group. This improvement might have reflected the success of the SCT-based intervention in promoting healthy behaviors. The general self-efficacy of the participants and their ability to overcoming impediments in their working environment were improved after 3 months of intervention.
The results indicated multifaceted training involving physical therapy based on SCT improved mediator variables, such as predicting constructs that significantly reduced pain and disability in the intervention group. In the control group, who received just the physical training, these improvements were not evident. Thus, it seems physical training in the context of SCT constructs could have better and continued results regarding pain reduction and disability improvement.
Consistent with the present findings, Plotnikoff et al. [20] reported in a study of 1717 adults that a SCT-based educational intervention could predict 59% of the physical activity behavior variance among their participants. The present results are also consistent with another study healthier behavior in participants receiving a SCT-based intervention [21].
The mechanism of SCT in promoting behavior has been reported [12]. The present results reinforced prior reports as the success of multidisciplinary programs in reducing the disability of the participants compared to the typical monodisciplinary approach of care [822]. Therefore, multidisciplinary treatment (such as physiotherapy education+SCT-based educational in the present study) appears to be much more effective than a physiotherapy educational program alone for decreasing LBP severity and disability. The collective findings indicate that the success of the intervention program may be due to continued motivation of the participants to cope with preventive behavior change regarding LBP. Participants in intervention group were encouraged to cope with their working environment and developed confidence that they could overcome workplace impediments. Participants in physiotherapy educational program only received education regarding healthy behaviors and proper exercise.
Also consistent with these results, Petit et al. [23] reported the benefits of a mixed and lighter intensive multidisciplinary strategy on disability and pain reduction compared to two other approaches like intensive hospital-based program and outpatient program [23]. Furthermore, it has been argued that to effectively treat chronic pain patients, functional restoration program as well as psychosocial support programs are necessary [22]. The current results are consistent with results from other studies [24252627] in which the reduction of pain severity and disability rate were observed after intervention. Furthermore, a previous study reported better effects of multidisciplinary group rehabilitation versus individual physiotherapy for chronic nonspecific LBP reduction [28].
Lack of social support in the health system in Iran is a reality. The present study addresses psychological, biological, and social aspects of chronic pain. The role of health education specialist during this study was of crucial value, and is an aspect of the health system worth bolstering. The benefits of motivation and social support in improving outcomes in patients with chronic LBP have been reported [29].
As with most research, there are some limitations in this study that could have affected the findings. There were no data regarding the use of other resources. Secondly, the data were self-reported. However, the findings are consistent with previous data that have indicated the value of multidisciplinary treatment for LBP.
Conclusions
Physiotherapy training that integrates education based on SCT can lead to significantly better results concerning health behavior changes and reduction of pain and disability among nurses suffering from chronic LBP.
Acknowledgments
The financial support of the Research Deputy of Tarbiat Modares University is gratefully acknowledged. The author would like to thank them for this financial support.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.