Introduction
Foramen transversarium (FT) is the special foramen located on the left and right transverse processes of the cervical vertebrae (C1 to C7) containing the vertebral vessels and sympathetic plexus. Each side of the vertebral artery originates from the subclavian artery before continuing onto the FT of the 6th or 7th cervical vertebrae through the atlas to form the basilar artery on the brain stem. Clinically, the variable morphology and pathology of the FT are important to consider when performing surgery for screw fixation of the upper or lower cervical spine. In addition, variations of FT could be associated with compression of vertebral vessels, resulting in blood flow disturbances, especially vertebrobasilar insufficiency [1ŌĆō3]. It has been reported that the anatomy and morphometry of FT vary by nationality [4ŌĆō7]. Taitz et al. [7] in 1978 have classified the FT into five types based on the shape and direction of the main diameters. When comparing upper cervical vertebrae (C1 and C2), the type 1 (round FT shape) with a greater diameter of the left C2 has been reported in Chilean [6] and Indian [7] populations. In contrast, the shape of the FT has been classified into 13 types in the South African population and no difference was found in the anteroposterior (AP) and transverse diameters of the upper cervical spine FTs [5]. In Kenyans, the shape of the FT most commonly found was type 2 or elliptical, with the main diameter in the AP direction [8]. Moreover, the incidence of a double FT has also been documented in various nationalities [1,7ŌĆō10]. Particularly on C1, the presence of an osseous prominence in place of the C1 sulcus, known as a foramen arcuale (FA), has been investigated and is suggested to have clinical significance, especially in terms of potential instability of screw insertion at the atlantoaxial joint [11]. Recently, there was a report on the direct measurement of subaxial cervical pedicles in Thai patients [12]. However, the morphometry of FT and FA in the northeast Thai population has not yet been investigated. Therefore, this study aimed to investigate the morphometry and incidence of FT. In addition, the variant formation of FA was also recorded. This morphometric study explored the size of the FT for consideration prior to upper cervical spine fixation in the Thai population, with the aim of avoiding injury to vertebral vessels and the sympathetic plexus.
Materials and Methods
1. Source of dried upper cervical spine samples
For this study, upper cervical (C) spine vertebrae, atlas (C1) and axis (C2) without degenerative disorders were collected from 107 northeastern Thai skeletons (age, 37ŌĆō94 years: average, 63 years; 53 males and 54 females) in the Unit of Human Bone Warehouse for Research, Department of Anatomy, Faculty of Medicine, Khon Kaen University, Thailand. This study was approved from the Ethics Committee for Human Research, Khon Kaen University, Thailand (approval no., HE621190).
The bones used in this retrospective study have been donated by people before their death with informed consents for studying and research of our medical and paramedical students.
2. Measurement of foramen transversarium diameters
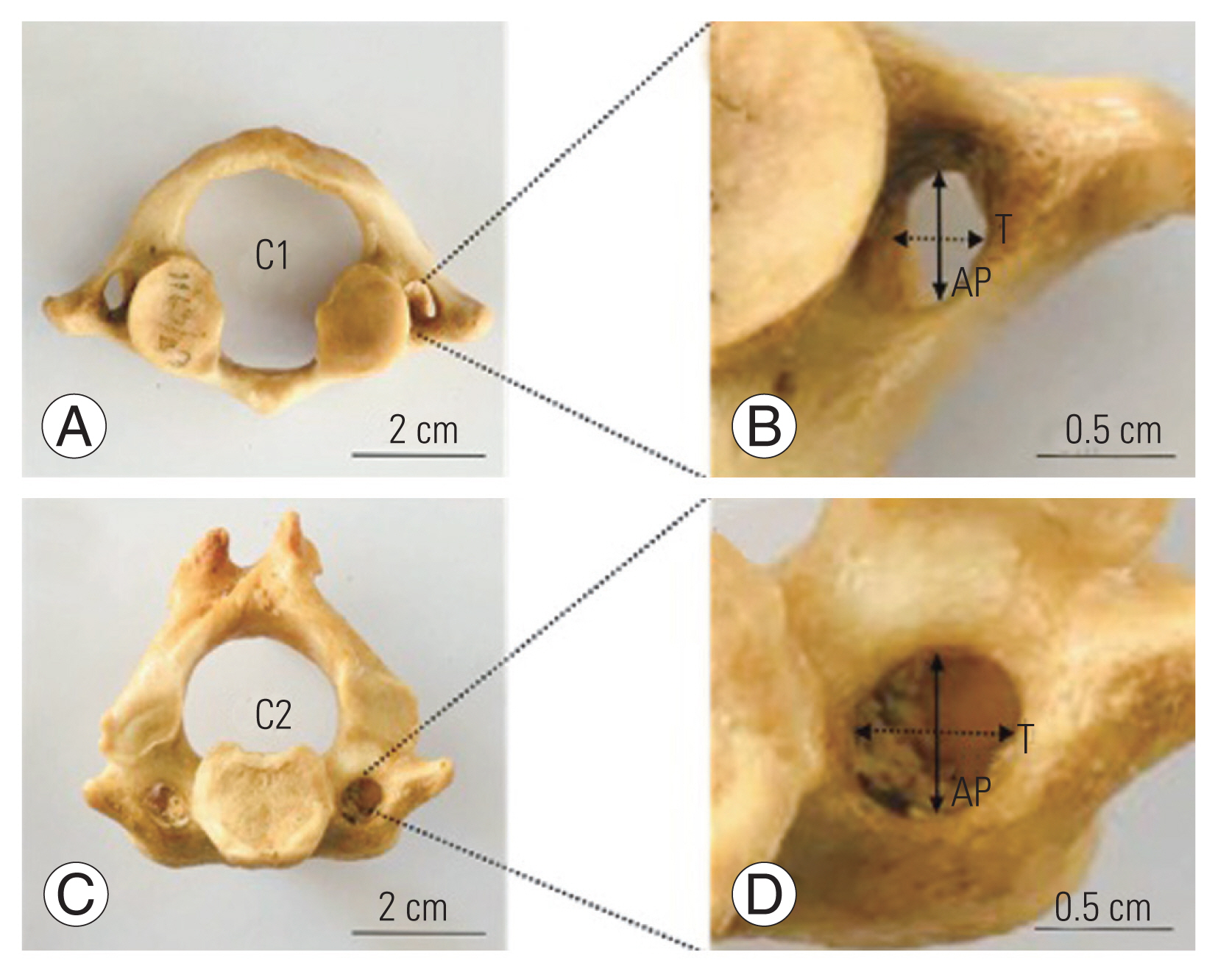
The FT diameters of each upper spine on both sides were measured in the AP and transverse planes using a Digital Vernier Caliper (0.01 mm precision; Mitutoyo, Kawasaki, Japan) in triplicate as shown in Fig. 1. This measurement was performed by internal and external observers on different days.
3. Classification and observation of the foramen transversarium
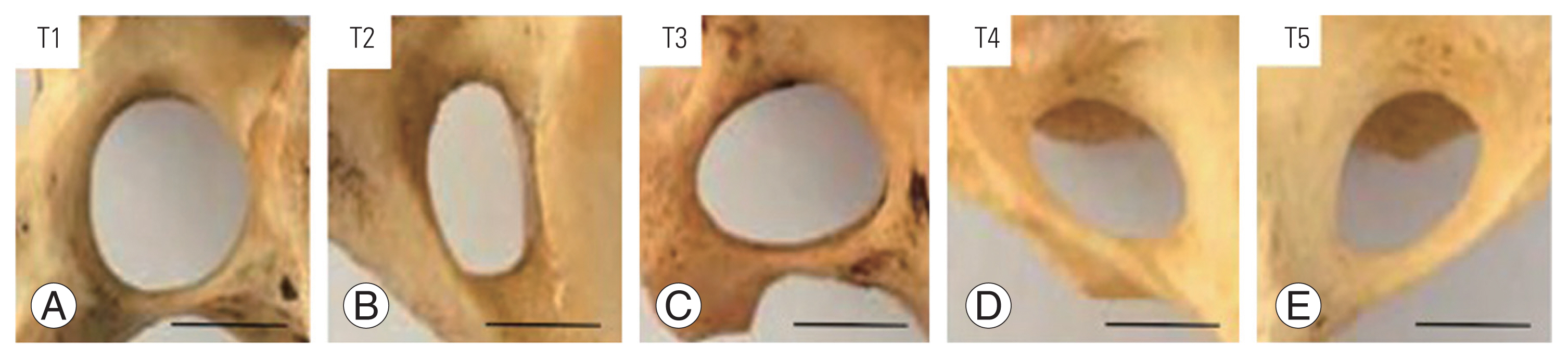
Morphological features of the FT were classified into five types including round (type 1), elliptical with AP (type 2), elliptical with transverse (type 3), elliptical with oblique from right to left (type 4), and elliptical with oblique from left to right (type 5) as described in previous reports [4ŌĆō7]. In addition, the variations of the accessory FT on the left or right sides of the upper spine in both sexes were also recorded and photographed. In detail, the FT variations in both sexes were classified into five types; variant FAs of C1, trilateral accessory foramen transversarium (TFT), bilateral accessory foramen transversarium (BFT), unilateral accessory foramen transversarium (UFT), and hypoplasic foramen transversarium (HFT). Subtypes of FAs included bilateral complete foramen arcuale (BCFA), unilateral complete foramen arcuale (UCFA), and incomplete osseous bridge (IOB).
4. Statistical analysis
The mean and standard deviation from all morphometric measurements are presented in this study. These continuous variables were tested for their normality using the Shapiro-Wilk test. An independent sample t-test was used to test the mean differences between the sexes. A paired sample t-test was performed to test the mean differences between the left and right sides or between the AP and transverse diameters. Statistical significance was set at p>0.05. All data were analyzed using IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA).
Results
1. Morphometry of foramen transversarium of the upper cervical spine
The overall morphometries (AP and transverse diameters) of the FT of the C1 and C2 in both sexes with the left and right sides of 107 dried bones are shown in Table 1.
2. Comparison of foramen transversarium diameters between sexes and sides
It was found that the transverse diameter of upper spine FTs in males was significantly greater than those of females (Table 2). The AP diameter of the C1 in both sexes was significantly greater than that of the transverse diameter, but there was no difference between males and females (Table 2). For C2, the transverse diameter of both sexes was significantly greater than that of AP. Additionally, AP and transverse diameters of the right FT in C1 were significantly greater than that of the left FT (Table 2). In contrast to C1, the transverse diameter of the right FT in C2 was significantly smaller compared with the left FT. However, there was no difference in AP diameters between the sides of C2 (Table 2). Moreover, the AP diameter of both sides in C1 was greater than that of transverse, while this measurement was significantly shorter than the transverse diameter of C2, as shown in Table 2. The two diameters of the C1 and C2 FTs were not significantly different between males and females, except for the transverse diameter of the right side in males, which was greater than that of females (Table 3). The FT diameters of the upper spine were not different between sexes. In contrast, the transverse diameter of the right FT in C1 was significantly greater than that of the left side in males, whereas the diameter in C2 of females was significantly shorter on the right side, as shown in Table 3.
3. Classification of upper cervical spine foramen transversarium types
In terms of FT types, type 1 (88.79%), type 2 (69.81%), type 3 (17.92%), type 4 (12.26%), and type 5 (13.20%) were found in males (Table 4). In females, there were type 1 (79.63%), type 2 (83.33%), type 3 (12.96%), type 4 (12.04%), and type 5 (12.04%), as shown in Table 4. There was no incidence of type 3 in C1 or type 2 in C2 found in the male FTs. In the female FTs, types 3ŌĆō5 in C1 were not observed (Table 4).
4. Variations of foramen transversarium and foramen arcuale formation
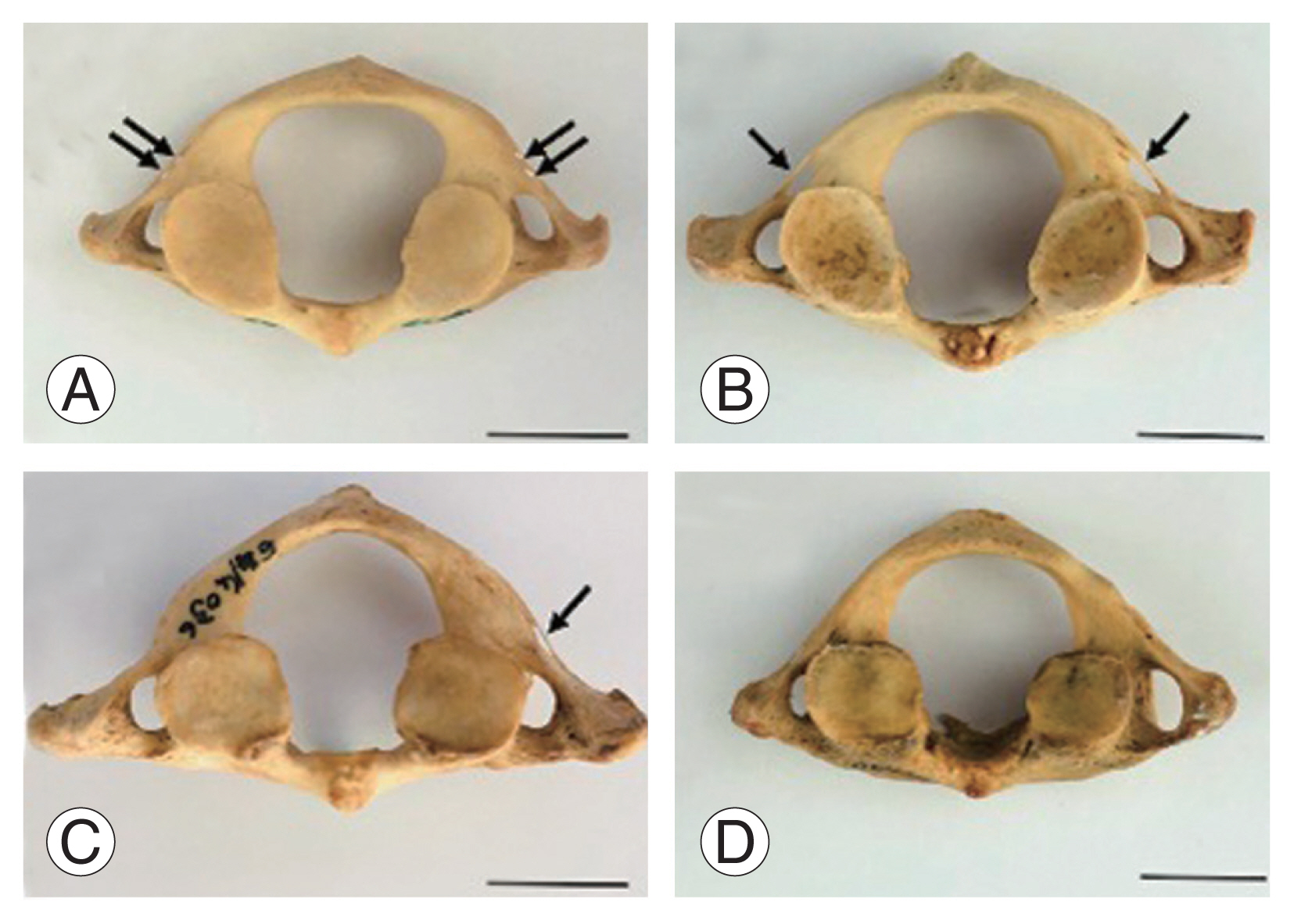
Classification and variations of FT are shown in Figs. 2 and 3. The incidence of BCFA was 0.93%, while that of UCFA and IOB was 2.80% and 9.35%, respectively. In addition, the TFT (1.87%), BFT (25.23%), UFT (8.41%), and HFT found in males (0.93%) were observed in C1. For C2, the incidence of UFT or HFT was 0.93%.
Discussion
Previous studies have reported on FT morphology, including variations in size and shape. Clinically, variations of FT could cause vertebral compression, leading to neurological symptoms. Additionally, these variations are important for surgeons and radiologists to consider prior to surgery on the posterior upper cervical spine [13]. The morphometric alterations of FT diameters have been documented in many populations including Chilean [6], Kenyan [8], Greek [4], Indian [7,14], American [15], Turkish [16], Japanese [17], Chinese [17], and Korean [18]. We herein observed the shape and size of the FT in Thais for the first time. Using Digital Vernier Caliper (Mitutoyo), our results showed shorter FT diameters in both sides of the upper cervical spine compared with Chilean and Kenyan populations [6,8]. The transverse diameter of the male C1 observed in one recent study was significantly greater than that of females, unlike what was found for Kenyans [8], which showed AP diameters in males that were significantly greater than in females. Similar to Asian populations [17], transverse diameters in Thais were significantly greater in males than in females. However, the transverse diameter in Kenyans was not different between sexes, whereas its diameter was greater in Thai males. In South Africans, no difference in FT diameters of the upper spine vertebrae have been found [5]. In general, the transverse diameter of the left side is greater than that of the right side in some nationalities including the Thai population [5ŌĆō7], as summarized in Table 5. In the literature, the shape of the FT can be classified into 5, 12, and 13 types [5ŌĆō8,17]. The FTs in this study were classified into five types as shown in Fig. 4. We found that the type 2 FT in C1 is mostly investigated (male, 69.81%; female, 79.63%) which is similar to that of the Kenyan [8], South African [5], Japanese, Chinese, and Indian populations [17]. In contrast, mostly only type 4 in Israeli and types 4 and 5 in Chilean and South African populations were found, with equal incidence [5ŌĆō7]. However, Kimura et al. [17] in 1985 reported that mostly type 5 was observed in the Japanese, Chinese, and Indian population. For C2, the most common type of FT found in Thailand was type 1, which is similar to that reported in many countries [5ŌĆō7,17]. In addition, the accessory FT (also called retrotransverse foramen) of C1 most commonly found in this study was BFT (25.23%), which was higher than that found in the Romanian (1.41%) [19], South AfricanŌĆōSpanish (1.5%) [20], Greek (1.61%) [21], Spanish (2.27%) [22], Indian (4%) [23], and Indian populations (4.08%) [24]. The incidence of UFT was approximately 9.38%, which was lower than that found in the Indian population (18%) [23]. In contrast, this incidence was higher in South AfricaŌĆōSpanish (5.8%) [20]. Furthermore, the presence of TFT and HFT in C1 from our study was 1.86%, which has not been reported previously. The finding of HFT in both C1 and C2 (1.86%) agreed with that found in C6 (1.1%) of the Italian population [25]. Moreover, the incidence of FA, sulcus or retroarticular canal for the vertebral artery, was found to be highest in the IOB subtype (9.35%). However, the highest incidences of UCFA were reported in the northern Greek (24.43%) [26] and Turkish populations (15.38% and 10%, respectively) [16,27]. The incidence of the FA subtype (BCFA) observed in the Thai population was 0.93%, which was low and comparable with that of the northern Greek (1.13%) [26] and Turkish (1.6%) populations [27]. In contrast, Cirpan et al. [16] in 2017 reported that BCFA had not been investigated in the Turkish population.
Conclusions
The morphometry of the upper spine FT in the Thai population is unique and differs from that of other populations. We conclude that all morphometric parameters are greater in the male FT and transverse diameter of the right C1, except for C2, which is greater than the left C2 in both sexes. Additionally, the most common type of FT in C1 is type 2, whereas in C2 the most common type of FT is type 1. Moreover, BFT is the most common FT variation investigated in the Thai population. The knowledge of FT and FA variations can identify potential landmarks for surgeons, neurosurgeons, and radiologists to help determine the most accurate approaches prior to posterior upper cervical surgery for specific populations.