Tuberculous and Brucellar Spondylodiscitis: Comparative Analysis of Clinical, Laboratory, and Radiological Features
Article information
Abstract
Study Design
This was a retrospective study.
Purpose
The aim was to compare the clinical, laboratory, radiological, and evolutionary features of tuberculous spondylodiscitis (TS) and brucellar spondylodiscitis (BS).
Overview of Literature
Clinical presentation of spondylodiscitis varies according to the underlying etiology, among which brucellosis and tuberculosis represent the primary cause, in endemic countries. Only a few studies have compared the characteristics between TS and BS.
Methods
A retrospective study was conducted using the data of all patients hospitalized for TS and BS in the infectious diseases department between 1991 and 2018.
Results
Among a total of 117 patients, 73 had TS (62.4%) and 44 had BS (37.6%). Females were significantly more affected with TS than males (56.2% vs. 22.7%, p<0.001). Fever (72.7% vs. 45.2%, p=0.004) and sweating (72.7% vs. 47.9%, p=0.009) were significantly more frequent among patients with BS. The median erythrocyte sedimentation rate was significantly higher in the TS group (median, 70 mm/hr; interquartile range [IQR], 45–103 mm/hr) than in the BS group (median, 50 mm/hr; IQR, 16–75 mm/hr) (p=0.003). Thoracic involvement was significantly more frequent in the TS group (53.4% vs. 34.1%, p=0.04), whereas lumbar involvement was significantly more frequent in the BS group (72.7% vs. 49.3%, p=0.01). Initial imaging findings revealed significantly higher frequencies of posterior vertebral arch involvement, vertebral compaction, and spinal cord compression in the TS group. Percutaneous abscess drainage (20.5% vs. 2.3%, p=0.005) and surgical treatment (17.8% vs. 2.3%, p=0.01) were more frequently indicated in the TS group, with a significant difference.
Conclusions
A combination of clinical, laboratory, and radiological features can be used to distinguish between TS and BS while these patients await diagnosis confirmation.
Introduction
Spondylodiscitis, also known as vertebral osteomyelitis, is a rare but serious infectious disease of the vertebrae and the intervertebral disc [1]. It accounts for 2%–7% of all cases of osteomyelitis [2]. The most common revealing symptoms are back pain and fever, followed by neurological deficits. However, there is also a report of apyrexia that contributed to diagnostic delay [3]. The clinical presentation varies according to the underlying etiology, which might be pyogenic (bacterial), parasitic, or granulomatous represented by tuberculous, brucellar, or fungal infection [4]. Globally, tuberculosis is the commonest cause of spondylodiscitis, accounting for 9%–46% of cases in developed countries [5,6]. In fact, brucellosis and tuberculosis are the major cause of spondylodiscitis in endemic areas [5].
In our intermediate-endemic country for tuberculosis [7], studies have reported that tuberculous spondylodiscitis (TS) represented around 60%–70% of cases of osteoarticular tuberculosis [8,9]. Brucellosis is also a widespread infection, contributing to a rate of 22% of brucellar spondylodiscitis (BS) [10]. Identification of the underlying etiology might be confusing and challenging, and only a few studies have compared the characteristics between TS and BS. In this perspective, this study was conducted to compare the clinical, laboratory, radiological, and evolutionary features between TS and BS.
Materials and Methods
1. Study design
This was a retrospective study conducted using the data of all patients hospitalized for TS and BS in the infectious diseases department between 1991 and 2018. We have not obtained ethical approval because of the non-interventional design of the study. The requirement for informed consent from individual patients was omitted because of the retrospective design of this study.
2. Data collection and case definition
TS was diagnosed on the basis of positive microscopic results using Ziehl–Neelsen staining for acid-fast bacilli or growth of Mycobacterium tuberculosis in the culture of specimens obtained from the bone marrow or abscess and/or caseation granulomatosis on histopathological examination. The isolation of M. tuberculosis from another site, associated with compatible clinical and radiological features of spondylodiscitis, confirmed the diagnosis. Otherwise, the diagnosis was based on strong clinical, radiological evidence and/or histopathological signs associated with positive tuberculin skin test and followed by an adequate response to antitubercular treatment. Tuberculin skin test was considered to be positive when the value was ≥10 mm after 72 hours of intracutaneous administration of five tuberculin units of purified protein derivative.
The diagnosis of BS was based on a positive Wright standard agglutination test (SAT) exhibiting a titer of ≥1/160 and/or the isolation of Brucella species from blood, bone marrow, or abscess cultures associated with compatible clinical and radiological findings. A minimum period of 10 days was required to incubate blood samples, which were cultured using an automated culture system.
Disc-bone specimens or paravertebral/psoas abscess specimens were collected through needle aspiration or biopsy and sent for histopathological examination for direct microscopic examination and culture for detecting Mycobacteria.
Surgical treatment was indicated in case of neurological deficits with compression of the spinal cord or when there was clinical or radiological deterioration despite adequate antimicrobial treatment. Surgical treatment comprised radical debridement and fusion surgery. Abscess drainage was indicated, along with medical treatment, depending on the size and location of the abscess.
Treatment with antimicrobial medication was stopped based on the resolution of clinical symptoms associated with improvements in laboratory and radiological parameters. Sequelae included spine deformity, which was defined as the appearance of scoliosis, kyphosis, or lordosis after the completion of the treatment. The patients had no spine deformity before the onset of spondylodiscitis infection.
3. Statistical analysis
Statistical analysis was performed using IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as frequencies and percentages. Continuous variables were presented as mean and standard deviation in case of normal distribution; otherwise, they were expressed as median and interquartile range. The chi-square test was used to compare two frequencies. Student t-test was used to compare two mean values in independent samples after conducting normality assessment. The Mann-Whitney U-test was used for nonparametric data analysis. The difference between groups was considered to be significant at p<0.05.
Results
During the study period, there were 117 patients, among whom 73 patients (62.4%) had TS and 44 patients (37.6%) had BS. Females were significantly more affected with TS than males (56.2% versus 22.7%, p<0.001). The mean age of patients with TS (49±19 years) and that of patients with BS (50±16 years) were not significantly different. Patients with BS consumed raw milk more frequently than patients with TS (90.9% versus 49.3%, p<0.001). In the TS group, four patients (5.4%) had a previous medical history of tuberculosis (Table 1).

Demographical, clinical and laboratory features of patients with TS and BS
Among patients with TS, 66.7% showed a positive tuberculin skin test with a mean diameter of 25±9 mm. Urine and sputum cultures were positive for M. tuberculosis in 3% and 1.5% of the patients, respectively. Multifocal tuberculosis was detected in 23 patients (31.5%). Pulmonary tuberculosis was found to be associated with TS in nine patients (12.3%), lymph node tuberculosis in six patients (8.2%), and intestinal tuberculosis in four patients (5.4%). There were four patients (5.4%) with renal tuberculosis and four patients (5.4%) with tubercular meningitis. The treatment regimen for patients with TS included isoniazid, rifampicin, ethambutol, and pyrazinamide for a 2-month duration, followed by isoniazid–rifampicin for the remaining period. The mean duration of antitubercular therapy was 13±7 months.
Among patients with BS, SAT result was positive with a titer of >1/1,280 in 15 patients (34.1%), >1/640 in 17 patients (38.6%), >1/320 in seven patients (16%), and >1/160 in five patients (11.4%). Blood cultures were performed for 32 patients (72.7%), of whom seven patients (21.8%) had positive results for Brucella species. Three patients (6.8%) had sacroiliitis associated with BS. Treatment for patients with BS included oral doxycycline 200 mg daily and oral rifampicin 900 mg daily for a mean duration of 7±3 months.
Fever (72.7% versus 45.2%, p=0.004) and sweating (72.7% versus 47.9%, p=0.009) were significantly more frequent among patients with BS. Neurological deficits were more frequent among patients with TS than among patients with BS (13.7% versus 2.3%), but the difference was not significant (p=0.05). Patients with TS had significantly higher laboratory values, including white blood cell count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels, than patients with BS (Table 1).
Radiological examinations comprised computed tomography scan that was performed for 75 patients (64.1%) and/or magnetic resonance imaging that was performed for 86 patients (73.5%). Patients with TS showed significantly more frequent thoracic involvement (53.4% versus 34.1%, p=0.04), whereas those with BS showed significantly more frequent lumbar involvement (72.7% versus 49.3%, p=0.01). The mean number of involved vertebrae was significantly higher in the TS group than in the BS group (2.4±1.1 versus 2.1±0.6, p=0.04). The initial imaging findings revealed significantly higher frequencies of posterior vertebral arch involvement, vertebral compaction (Fig. 1), and spinal cord compression in the TS group than in the BS group (Table 2). Spinal epiduritis was detected in both groups, but there was no significant difference (Fig. 2).
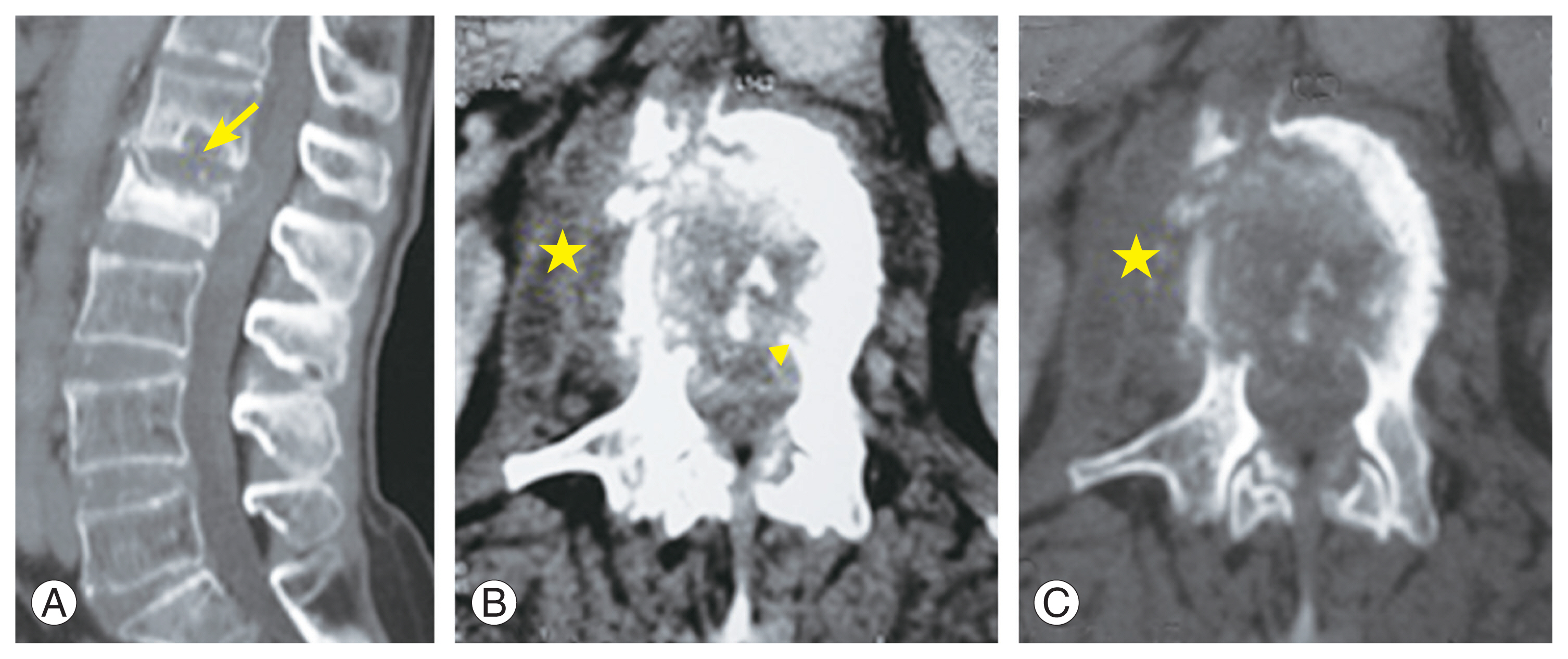
Tuberculous spondylodiscitis. (A) Sagittal computed tomography of the spine showing osteolytic lesion of L2 surrounded by osteocondensation and compaction of its vertebral body. L1–L2 disc enlargement associated with the presence of an intradiscal abscess and bony sequestrum (arrow). (B, C) Axial sections of computed tomography showing conus medullaris compression by an abscess (arrowhead) and the presence of an abscess in the right lateral vertebra (star).

Imaging findings of patients with TS and BS

Brucellar spondylodiscitis. Sagittal sections T1 (A), T2 (B), and T1 fat-saturated Gadolinium (C) of the lumbar spine showing anterior epiduritis extended from L4 to S1 and enhancement of anterior paravertebral soft tissue at the L4–L5 level (thin arrows). Heterogeneously hypointense signal of the vertebrae L4, L5, and S1 in T1-weighted images, especially at the anterior corners of L4, L5 and posterosuperior corner of S1, hypointense signal of the anterior corners of L4 and L5 in T2-weighted images and hyperintense signal of the rest of the vertebral bodies of L4, L5 and of the anterosuperior corner of S1 in T2-weighted images. The disc is hyperintense in T2 weighted images (thick arrow).
Percutaneous discovertebral biopsy (65.8% versus 22.7%, p<0.001) and abscess puncture (31.5% versus 13.6%, p=0.03) were performed significantly more frequently in the TS group than in the BS group. Along with medical treatment, therapeutic interventions, including percutaneous abscess drainage (20.5% versus 2.3%, p=0.005) and surgical treatment (17.8% versus 2.3%, p=0.01), were significantly more frequently indicated for patients in the TS group than in the BS group. The mean length of hospital stay was significantly greater in the TS group than in the BS group (27.5±18.6 versus 18±11.7 days, p=0.001). No significant difference was detected in the response to treatment between the two groups based on the median time to spinal pain disappearance and the median time periods for normalization of the levels of CRP, ESR, and white blood cell count (Table 3). Three patients (4.1%) in the TS group died. Sequelae were noted in the two patient groups, among which only spine deformity was significantly more frequent in patients with TS (27.1% versus 6.8%, p=0.007) (Table 3).

Comparison of diagnostic, therapeutic intervention and outcomes of patients with TS and BS
Discussion
Our study demonstrated the discriminative features of TS and BS. In developing countries, as ours, both tuberculosis and brucellosis are the major causes of spondylodiscitis [11]. The diagnosis might be challenging and confusing due to the similarity in clinical, laboratory, and radiological features. However, some distinctive features might guide the clinicians toward one etiology or another while awaiting diagnosis confirmation.
The literature reports variations in the comparison of age and gender between patients with TS and those with BS. For instance, Liu et al. [12] found that patients with BS were older than those with TS, but there was no difference in gender. Moreover, BS was found to affect the elderly population, whereas TS affected a younger age group [13]. In fact, younger age and female gender have been reported as risk factors for extrapulmonary tuberculosis [14]. In the present study, although a significant age difference was not detected, females were found to be significantly more affected with TS, which was consistent with the result reported by Colmenero et al. [15].
In general, patients consult a physician for back or neck pain that worsens at night and is associated with fever, which was less common in patients with TS [16]. In fact, the absence of fever might be linked against the infectious etiology of back pain. In a previous research, fever was observed in only one-third of patients with TS [17]. In our study, we found that fever was significantly more frequent in patients with BS, which was similar to previous findings [18]. In previous studies, neurological deficits were found to be significantly more frequent in patients with TS [12,19], which is consistent with our results, although no significant difference was observed. This might be explained by the delay between the onset of symptoms and the diagnosis, which varies among studies. In fact, neurological deficits generally appear during the late course of the disease. Approximately one-third of patients consult a physician for neurological deficits, such as leg weakness, numbness, and incontinence, which were associated with a delayed diagnosis [16]. Previous studies have reported neurological involvement in 50%–60% of patients with TS [19,20]. The absence of fever in patients with TS might explain the diagnostic delay and therefore contribute to the progression to a more complicated form of the disease associated with the appearance of neurological deficits.
It has been reported that inflammatory markers, including elevated ESR and CRP levels, were associated with spondylodiscitis in the majority of cases, and decreasing their levels was found to be useful for monitoring the response to treatment [6]. However, abnormal laboratory investigation results have been mild in BS cases [10] but significantly higher in TS cases [18], which are in agreement with our results.
Diagnosing BS might be easier than diagnosing TS, which is because serological tests and blood cultures are of immense help and thus reduce the need for interventional procedures. Studies have reported that the proportion of patients with BS who underwent invasive diagnostic procedures varied from 0% to 8.5% [18,20]. In the present study, this rate was found to be higher, which might be due to the high incidence of tuberculosis in our country and the need to exclude a possible tuberculous and BS coinfection, according to the clinician’s index of suspicion.
Imaging findings are the cornerstone of the diagnostic process. The level of spinal disease is known to vary according to the underlying etiology. It has been observed that thoracic involvement was generally associated with TS, whereas lumbar involvement was commonly associated with BS [18,21,22], a finding consistent with our result. Previous studies have demonstrated the destructive nature of TS compared with BS. In fact, multifocal involvement, significant bone destruction, and epidural abscess were suggestive of TS, whereas focal bone destruction and well-limited paravertebral involvements were suggestive of BS [12,18,22]. In addition, the involvement of posterior parts of vertebrae was frequently reported in TS cases [19], which is consistent with our results. In contrast to previous studies that reported that soft tissue abscesses were significantly more frequent in TS cases [19,20], we found no significant difference between the two groups in this regard. The destructive nature of TS and the diagnostic delay also explain the significantly high rate of patients in this group who underwent surgical therapy, which was consistent with other studies [18,20]. A better prognosis in patients with TS was associated with a prompt diagnosis before the appearance of any spinal deformity or neurological deficits [23]. A recent meta-analysis of 870 cases of BS reported treatment success in all the cases, with the absence of any residual complaints or relapse [24].
Conclusions
Our study demonstrated that a combination of clinical, laboratory, and radiological features can be helpful in distinguishing between TS and BS. The destructive nature of tuberculosis was obvious and explained most of the differences observed between the two patient groups. However, the diagnosis can be confirmed only based on microbiological and/or histopathological results.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.