Introduction
Due to an aging population and the needs of patients with spinal disorders, various minimally invasive surgery (MIS) techniques are gaining popularity. In particular, procedures that use percutaneous pedicle screws (PPSs) are practiced widely, such as MIS-transforaminal lumbar interbody fusion (TLIF) and MIS long fixation [1-4].
In 1982, Fraser [5] initially described the muscle-splitting retroperitoneal approach. In 2001, Pimenta [6] reported the lateral endoscopic trans-psoas retroperitoneal approach as a new MIS procedure. Subsequently, retractors and spinal monitoring were developed to enable direct visualization, which introduced the extreme lateral interbody fusion (XLIF) procedure [7]. Mayer [8] first introduced oblique lateral interbody fusion (LIF) in 1987; this technique was developed further to prevent lumbar plexus and femoral nerve palsies that result from the muscle-splitting retroperitoneal approach [8]. This diversified the LIF procedures that were available. LIF can provide interbody correction for spinal deformities and indirect decompression for spinal canal stenosis [9]. Moreover, for combined LIF with posterior fixation, a percutaneous reduction with combined LIF and PPS fixation (LIF/PPS) is becoming a standard procedure to reduce invasiveness and preserve the erector spinae muscle. For lumbar fusion resulting from degenerative spinal diseases, such as degenerative spondylolisthesis (DS), LIF/PPS is expected to achieve clinical outcomes that are comparable or improved compared to those of MIS-TLIF [10-12].
Indications for MIS-TLIF and LIF/PPS procedures, such as direct and indirect decompressions, remain unclear. Relative contraindications for LIF/PPS include a grade II slip or greater, high iliac crest, rising psoas, lateral recess stenosis, and severe central stenosis with cauda equina syndrome as its chief complaint [13-15].
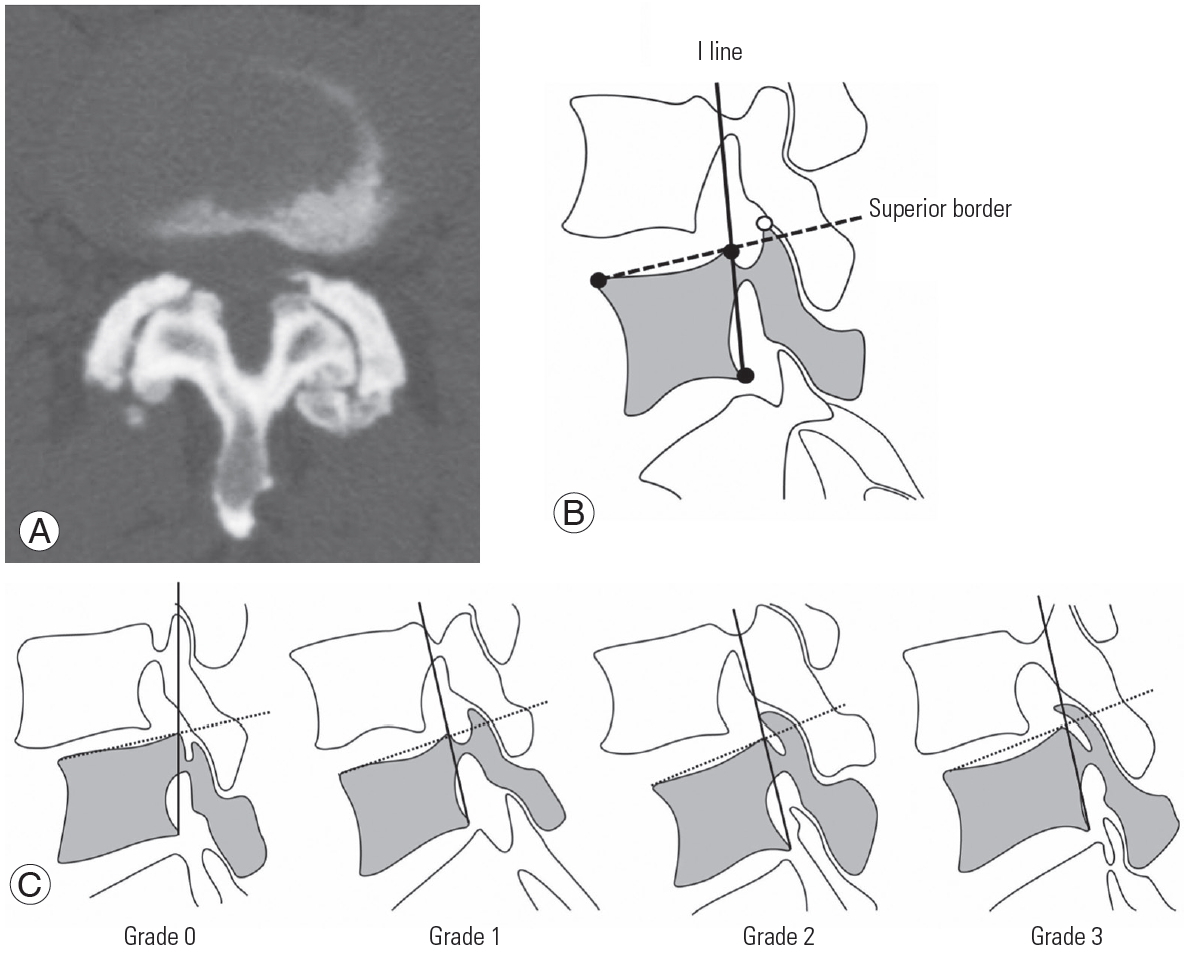
In terms of lateral recess stenosis, Satomi et al. [16] previously reported osteophyte formation on both the ventral and dorsal sides of the superior articular process as computed tomographic myelography (CTM) findings indicative of late stage spondylolisthesis (Fig. 1A). Because percutaneous reduction with anterior lumbar interbody fusion (ALIF) is difficult due to this facet deformity, which compresses the nerve root and prevents further slippage, they recommend a direct posterior decompression with or without fusion. Satomi’s classification is, thus, very useful for determining the surgical indication for ALIF. In contrast, there have been no previous reports on an effective radiographic indicator for determining the surgical indication for LIF/PPS, which provides a stronger corrective force.
Hence, this study’s purpose was to examine retrospectively the course of treatment and imaging findings in patients who had undergone LIF/PPS for DS. We also evaluated preoperative bony lateral recess stenosis and clarified the threshold of indirect decompression by LIF/PPS.
Materials and Methods
1. Patients and study groups
All aspects of this study were approved by the Institutional Review Board of International University of Health and Welfare (IRB approval no., 5-17-7), and informed consent was obtained from the study participants.
From February 2014 to May 2018, 185 consecutive patients underwent 1- or 2-level lumbar fusion surgery for DS. LIF/PPS was the only procedure performed for spinal fusion, and the study included 216 disc levels in 185 consecutive patients. The demographic characteristics of the sample were as follows: sex, 55 males and 130 females; mean age, 68.6 years (range, 44–91 years); and mean observation period, 32 months (range, 12–56 months).
The “recovery group” consisted of patients who exhibited improved postoperative symptoms, and the “no-recovery group” consisted of patients who developed new neurological symptoms. Evaluation criteria for the two groups included age, sex, number of fusion segments, pre- and postoperative Japanese Orthopaedic Association (JOA) scores, JOA recovery rates (RR), Oswestry Disability Index (ODI) scores, imaging findings, and need for reoperation. In the imaging findings, we evaluated the pre- and postoperative percent slip [17], rate of correction, and morphology of the superior articular process. We conducted this study according to Strengthening the Reporting of Observational Studies in Epidemiology guidelines [18].
2. Surgical procedure
Here, we briefly describe our MIS lateral retroperitoneal approach. All anterior approaches used a mini-open retroperitoneal trans-psoas or antero-psoas approach through a 4-cm skin incision performed by one surgeon (Ken Ishii). Free-running directional electromyography was used to define a corridor through the psoas muscle, anterior to the lumbar plexus and femoral nerve. An LIF retractor was applied at the intervertebral disc level under fluoroscopy. After the great vessels ventral to the lumbar spine were mobilized laterally, the affected interspace was treated with a discectomy, followed by sizing and placement of an intervertebral cage. Then, in 144 cases, the cage was implanted by an extreme lateral interbody cage (CoRoent XLIF Titanium Cage; NuVasive Inc., San Diego, CA, USA), and in 41 cases it was implanted with an OLIF25 PEEK Clydesdale Spinal System (Medtronic Sofamor Danek, Minneapolis, MN, USA) with auto-iliac cancellous bone and hydroxyapatite.
After interbody cage placement, all patients were positioned prone, and PPSs were placed above and below the affected level. Rod fixation then proceeded, first by insertion and the final tightening in the inferior pedicle screws, followed by cantilever reduction of the superior pedicle screws into the rod, which allowed further reduction of the spondylolisthesis.
3. Statistical analysis
Statistical differences were evaluated by the Mann-Whitney test and one-way analysis of variance, followed by Fisher’s protected least significant difference post-hoc test and Fisher’s exact probability test. Statistical analysis was performed using the IBM SPSS Statistics ver. 21.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as p<0.05.
4. Radiographic examinations
Plain radiographs and computed tomography (CT) images of the lumbar spine before surgery and during follow-up were evaluated in 216 disc levels of 185 cases. On preoperative axial CT images, the facet joint osteoarthritis was evaluated by the Pathria’s grading system of Pathria et al. [19]. On sagittal CT images, we focused on the shape and position of the superior articular process in the bilateral facet at the slipping level. First, in terms of the medial end of the apex of the superior articular process (or, in other words, the sagittal image slice that comes into contact with the lateral border of the spinal canal), the line that connects to the posterior surface of the inferior vertebral body was defined as the “impingement line” (I line) (Fig. 1B). The following four classifications were created according to the position of the apex of the superior articular process on the line that connects the I line to the superior border of the vertebral body (Fig. 1B, C): grade 0, the apex of superior articular process does not exceed the superior border of the vertebral body and does not contact the I line; grade 1, the apex exceeds the superior border but does not reach the I line; grade 2, the apex projects out on the ventral side and contacts the I line; and grade 3, the apex exceeds the I line (Fig. 1C). In terms of whether or not the apex of the superior articular process exceeds the I line, grades 0–1 and 2–3 were defined as I line+ and I line-, respectively. We classified all 432 superior articular facets in 216 disc levels of 185 patients, and we compared the characteristics of the recovery and no-recovery groups. In addition, we evaluated characteristics of the subgroups.
Results
We encountered no serious complications, such as vascular, ureteral, visceral, or neurologic injuries, in any of the 185 cases. Three cases underwent revision surgery. The overall JOA score increased from a mean of 13.1 points before surgery to a mean of 27.5 points at final follow-up, showing a JOA RR of 90.8%. The ODI score also improved from 46.3% before surgery to 9.9% at final follow-up. Immediately after the operation, 171 of 185 patients demonstrated improved symptoms, including leg pain (recovery group), while degeneration of symptoms was observed in 14 of 185 patients (7.6%) (no-recovery group). There were no statistically significant differences in age, sex, operative levels, percent slip, JOA scores, RR, or ODI scores between the two groups (Table 1). In all 14 cases of the no-recovery group, there were aggravated symptoms of lower extremity pain immediately after surgery (Table 2). Four patients at the L4 level and one patient at the L3 level achieved good percutaneous reduction, and percent slip recovered from 19.8% preoperatively to 5.7% postoperatively. Postoperative symptoms included aggravated lower extremity pain on the affected side in four patients and on the unaffected side in one patient. All patients were diagnosed with symptoms associated with deteriorated bony lateral recess stenosis and underwent conservative treatment; however, posterior decompression of the fusion site was performed additionally at a mean of 20.4 days (range, 7–60 days) postoperatively for five patients who showed no symptomatic improvement. Intraoperative findings revealed that all five patients exhibited a strong compression of the nerve root in the superior articular processes on the side of the affected lower extremity. Thus, we decompressed the nerve root by facetectomy. Symptoms of the remaining nine patients were resolved by conservative therapy at approximately 1 month. At final follow-up, the mean JOA score in the no-recovery group improved from 13.9 to 27.2 points.
In the analysis of preoperative axial CT images using Pathria’s grading system, there were no facet joints that were grade 0, 39 were grade 1, 144 were grade 2, and 33 were grade 3. No significant differences were found between the recovery and no-recovery groups (Table 1). In the overall evaluation of reconstructed preoperative sagittal CT images by our classification, 39 processes (9.0%) were grade 0, 358 (82.9%) were grade 1, 29 (6.7%) were grade 2, and 6 (1.4%) were grade 3. Of the 404 processes in 171 patients of the recovery group, 39 processes were grade 0, 358 were grade 1, seven were grade 2, and none were grade 3. Ninety-eight percent of the study population was either grade 0 or 1. Interestingly, there were no processes classified as grade 0 and 1 (I line+) in the no-recovery group. All processes were classified as grade 2 or greater (I line -) (grade 2, 22 processes; grade 3, 6 processes; p=0.0233) (Table 1). On the first postoperative CT images in the norecovery group, the superior articular processes of the lower vertebral body, approaching the intervertebral disc and bony lateral recess stenosis, were observed at the fusion level (Fig. 2). Next, we compared the percent slip before and after surgery in seven patients (recovery subgroup), who were grade 2 or greater in the recovery group, and 14 patients in the no-recovery group. As a result, the percent slip improved significantly from 19.2% to 3.8% in the recovery group and from 22.2% to 1.8% in the norecovery group. There was no significant difference in the correction rate between recovery and no-recovery groups (p=0.438). However, the correction rate for slippage of the seven patients in the recovery subgroup was significantly lower than that of the 14 patients in the no-recovery group (p=0.032). There was not a significant correlation between Pathria’s grading and our classification.
1. Case presentation: case 1 (a 78-year-old female, I line-, grade 3)
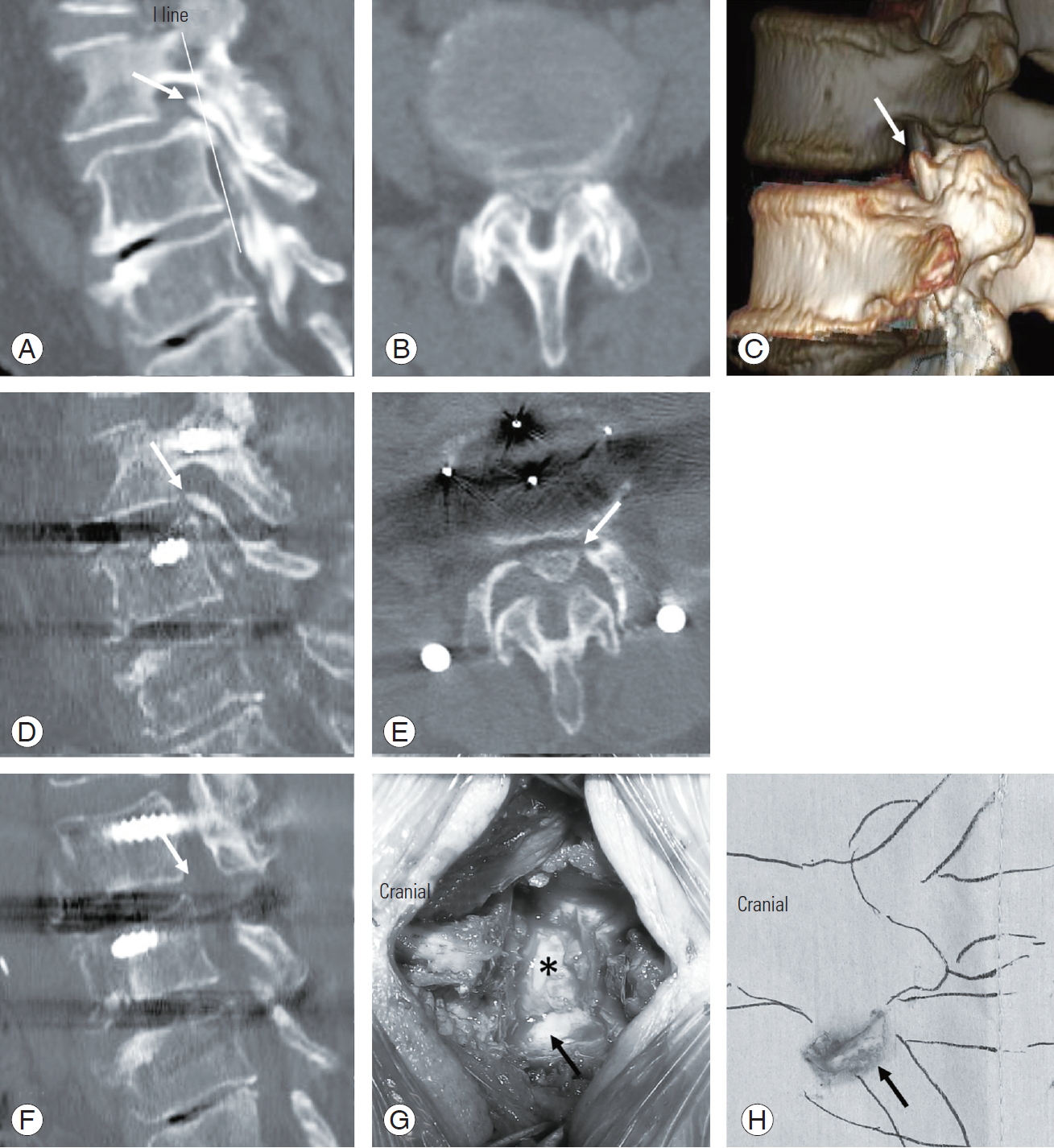
Preoperative radiographic images revealed degenerative lumbar scoliosis with Meyerding grade II DS at L3–4 (Fig. 2A–C). The preoperative CT reconstruction showed the patient was at stage 2 on Satomi’s CTM classification (Fig. 2B). The apex of the bilateral superior articular processes of the L4 vertebral body (arrows in Fig. 2A, C) completely exceeded the I line (solid line in Fig. 2A), which was grade 3 on our classification system. We performed a percutaneous reduction of DS at L3–4 and fusion at L3–5. Anterior slippage at L3 was corrected 100% with surgery.
Immediately after the operation, the patient’s left lower extremity symptoms were aggravated, and we observed a decrease in manual muscle testing (MMT) of the quadriceps. On nerve root block and CT images, the patient was diagnosed with bony lateral recess stenosis due to a massive superior spur in the left superior articular process (arrows in Fig. 2D, E), and decompression surgery at the L3–4 levels was performed 7 days after the first operation (Fig. 2F). Because the intraoperative findings revealed that the left superior articular process (arrow in Fig. 2G) severely compressed into a part of the dura (asterisk in Fig. 2G) and left L4 nerve root, the superior articular process (arrows in Fig. 2G, H) was resected and the L4 nerve root was decompressed. Immediately after the operation, the left leg pain was resolved, and the MMT improved. In the 1-year postoperative CT images, the left facet of L3–4 was resected (arrow in Fig. 2F). At final examination (25 months postoperatively), the preoperative JOA score had improved, from 14 to 28 points (JOA RR=93%).
Discussion
Minimally invasive procedures, such as MIS-TLIF and LIF/PPS, have gained popularity in recent years. The major difference between MIS-TLIF and LIF/PPS is that the former can achieve direct decompression, while the latter achieves indirect decompression on nerves. LIF/PPS has been reported to have complications specific to LIF [20,21], but it has a great advantage in that it can achieve nerve decompression indirectly without touching the nerves, in addition to its high corrective force and ample bone grafting volume.
To obtain sufficient indirect decompression with LIF for DS, a larger slip correction can induce a larger expansion of the spinal canal. Satomi et al. [16] listed lateral stenosis as a contraindication for ALIF in DS cases, and they reported a classification system based on axial images of preoperative CTM. In the facet joints, stage 3 cases are especially challenging to correct for slippage with ALIF and are, likewise, contraindicated, because osteophytes form in the superior articular process, envelop the inferior articular process, and the morphology of the facets look as though they are locked. The current LIF/PPS procedures can often achieve percutaneous reduction, even in stage 3 cases, due to the expansion of the intervertebral height by cage and strong corrective force by PPS. On the other hand, greater correction for slippage can induce osteophytes of the superior articular process that protrude ventrally to move closer to the slipped vertebral body that is corrected dorsally, wherein the superior articular process can enter the dorsal side of the nerve root to aggravate the lateral stenosis (Fig. 2A–E). However, there are no good indices using preoperative imaging to assess bony lateral stenosis.
In this study, we report a classification system for preoperative evaluation of lateral stenosis using I line, a new radiographic indicator. To the best of our knowledge, this is the first report to introduce techniques that can evaluate lateral stenosis properly, and we believe that this study presents a very useful indicator and classification system. Because nerve root compression by the superior articular process occurs on the side of the spinal canal, an important aspect of a classification system is that the sagittal CT slice should be parallel to the lateral side of the spinal canal. In our study, all 14 patients who exhibited aggravated symptoms after undergoing LIF/PPS (no-recovery group) were grade 2 or greater (I line-) in our classification system. Good correction of slippage was obtained in all cases. In five cases that required posterior decompression, the osteophyte of the superior articular process entered the dorsal side of the nerve root. In patients classified as grade 2 or greater, the smaller the gap between the superior articular process and the sliding vertebral body that includes the intervertebral disc, the more the slippage correction will compress the nerve root. In fact, postoperative lower extremity pain in the no-recovery group was more severe in terms of pain and paralysis than it was prior to surgery. In addition, most patients of the recovery group were grade 1 or less (I line+), but seven patients were grade 2 or greater (I line-) (recovery subgroup). In the recovery subgroup, we believe that the significant insufficiency in correction compared to the no-recovery group (p=0.032) may have been the reason why the postoperative symptoms did not show aggravation. In addition, it is necessary to keep in mind that the grade of the superior articular process is not necessarily bilaterally congruent, due to scoliosis, and that neuralgia of the contralateral leg may appear after correction. Therefore, in DS cases classified as grade 2 or greater (I line-), the risk of aggravated bony lateral recess stenosis due to corrective surgery is high; therefore, indirect decompression by LIF/PPS is, in principle, contraindicated. In these cases, we recommend a direct decompression from the posterior aspect.
Our study had several limitations. First, we conducted a retrospective cohort study, which was subject to potential confounders and selection bias. Second, our results and proposals were based on one surgeon’s experience. Third, although our new indicator and classification system is very useful, we did not take into account disc bulging, herniation, or osteophytes at the posterior margin of the vertebral body. Thus, it is necessary to evaluate imaging findings, such as magnetic resonance imaging and CT, individually, even for grade 1 cases and determine the indication for LIF/PPS surgery so that the bony lateral recess stenosis does not deteriorate due to deformity correction.
Conclusions
In the present study, we reported a novel classification system for the preoperative evaluation of lateral stenosis using I line, a new radiographic indicator. In DS cases classified as grade 2 or greater in our grading system, the risk of aggravated bony lateral recess stenosis due to corrective surgery is high; therefore, indirect decompression by LIF/PPS is, in principle, contraindicated.