Is Anterior-Only Fixation Adequate for Three-Column Injuries of the Cervical Spine?
Article information
Abstract
Study Design
Retrospective case series.
Purpose
To analyze the clinical and functional outcomes of patients who have undergone anterior cervical discectomy/corpectomy and fusion (ACDF/ACCF) for a three-column cervical spine injury (CSI).
Overview of Literature
The treatment of choice for a three-column CSI is an area of contention; however, combined anterior and posterior fixation is the preferred method explored in the literature. Studies have shown the superior biomechanical stability of posterior fixation over that of anterior fixation, but anterior-only approach in CSI has been proving its efficacy in recent times by providing reasonable stability with the maximum achievable decompression and fusion.
Methods
Twenty-one patients undergoing ACDF/ACCF with a bone graft/metallic cage treatment for cervical injuries involving all three columns from January 2016 to July 2018 were included in the study. All of the patients were followed up monthly for the first 3 months and then every 6 months, until their last follow-up visit.
Results
Nineteen patients had AO type C injuries and were managed with ACDF, and two patients with AO type B injuries were managed with ACCF. Fifteen had a complete spinal cord injury, while six had an incomplete spinal cord injury (American Spinal Injury Association B, C, and D). The mean segmental kyphosis at presentation of 12.2°±4.4° improved in the postoperative period to -7.2°±2.5°. At their final follow-up, all the patients showed clinical improvements when assessed by the Visual Analog Scale (6.8–1.8), Oswestry Disability Index score (59.7–34.9), and Spinal Cord Independence Measure score (24.8–36.4). One patient in the ACDF group needed a secondary posterior fixation because of instability.
Conclusions
An anterior approach to the cervical spine in cervical fracture dislocations is an effective treatment showing an optimal recovery rate in terms of patient-reported outcomes and structural stability, with the added advantages of less blood loss and the fact that the technique requires less instrumentation.
Introduction
Injury to the cervical spine involving all three columns is a serious problem in acute trauma scenarios that accounts for 2.4% of all blunt trauma [1] and 55% of all spinal cord injuries [2]. Commonly presenting injury patterns involving all three columns include flexion-distraction injuries (AO type B) and cervical fracture dislocations (AO type C). The most commonly reported sources of cervical spine injuries are vehicular accidents (41%), falls (27%), violence (15%), sports-related injuries (8%), and heavy objects falling onto the head [3].
Management of three-column injuries of the cervical spine (TCICS) demands achieving an adequate reduction with the reconstruction of the anterior and posterior tension bands, the decompression of neurological structures, and an emphasis on achieving early fusion for rehabilitation. Although combined anterior and posterior stabilization is considered the choice of surgery for these injuries, with improved instrumentation techniques and the right indications, anterior- or posterior-only stabilization to create instrumented fusion may prove to be an attractive alternative to combined surgery. Though biomechanical studies have shown that posterior stabilization allows for a more rigid fixation than anterior plates [4], the anterior approach allows direct decompression in cases with a protruded intervertebral disc or a fractured, retropulsed bone fragment, both of which may require the use of a large graft surface area, reducing the number of fused segments. The aim of this study is to assess the clinical and functional outcomes in patients undergoing anterior cervical discectomy/corpectomy and fusion (ACDF/ACCF) for TCICS.
Materials and Methods
1. Patients
This study is a retrospective case series from prospectively collected data of all the patients with a cervical flexiondistraction (AO type B), or fracture dislocations (AO type C), injury surgically treated via ACCF/ACDF in our institute from January 2016 to July 2018. The study was approved from the institutional review board of All India Institute of Medical Sciences (AIIMS/IEC/19/842). Informed consent was obtained from all individual participants included in the study. Patients with an injury at more than a single cervical level, or radiological evidence of compression over the posterior cord due to the fracture of posterior elements, were excluded from the study. Informed consent was obtained from all individual participants included in the study. The data in the registry for spinal trauma were reviewed for age, gender, mechanism of injury, level of injury, neurological status using the American Spinal Injury Association (ASIA) impairment scale, and functional status using the Visual Analog Scale (VAS), Oswestry Disability Index (ODI) score, and Spinal Cord Independence Measure (SCIM) score. Radiological data were evaluated for the type of injury, degree of subluxation/dislocation, and segmental kyphosis at the time of presentation. Facet reduction, adequate decompression, and an improvement in segmental kyphosis were evaluated in the immediate postoperative period, while bony fusion, instability, loss of correction, and implant-related complications were emphasized at the final follow-up.
All the patients who were brought in with a suspected cervical spinal cord injury were immobilized with a Philadelphia collar. Radiological data included plain radiographs in anteroposterior (AP) and lateral views, noncontrast computed tomography (CT) images, and magnetic resonance (MR) images. The criteria for a diagnosis of TCICS included radiographs and CT scans suggestive of unilateral or bilateral, jumped, or perched facets or facetal fractures (or both) and flexion-distraction type injuries. MR images provided additional information about retropulsed disc fragments, the grade of spinal cord compression, cord edema or hematoma, and the magnitude of ligamentous injury. Patients with cervical fracture dislocations underwent a closed reduction under general anesthesia (GA) in an operating theater, followed by ACDF in the same session. In patients where surgery was expected to be delayed due to poor physical condition or a lack of surgical fitness, a closed reduction was attempted with cervical traction using Crutchfield tongs, with a gradually increasing weight, followed by ACDF/ACCF once the patient was deemed fit for surgery. Two patients with AO type B2 injuries with retropulsion of a posterior fragment underwent corpectomy and anterior instrumented fusion (ACCF) (Fig. 1).

Summary of management in the study group. ACCF, anterior cervical corpectomy and fusion; ACDF, anterior cervical discectomy and fusion.
2. Surgical technique
All the surgeries were performed by a single, senior spine surgeon. After GA and patient positioning, a closed reduction was attempted by manual cervical traction and flexion, followed by a gradual extension of the head under intraoperative fluoroscopy. Once the reduction was achieved, the extended position of the head and neck was secured using a soft roll in the interscapular region and by strapping the forehead. In cases where a closed reduction was not achieved, we considered an open reduction after a discectomy. A standard Smith and Robinson [5] approach was used for discectomies. We routinely removed posterior longitudinal ligament to examine the cord and to remove any retropulsed discs. Corpectomies were performed in cases with a vertebral body fracture and retropulsed bony fragments. Tricortical bone grafts harvested from the iliac crest, a polyether ether ketone (PEEK) interbody cage, or a mesh cage, filled with autologous bone grafts (in corpectomy cases), were used to obtain interbody fusion. A locking anterior cervical plate fixed with unicortical screws was used for stabilization. The final fixation was checked in the AP and lateral planes.
Postoperatively, X-rays and CT scans were done to confirm both reduction and fixation. Patients were kept under observation and postoperative immobilization with a sterno-occipital mandibular immobilization brace. After discharge from the hospital, they were followed up regularly at monthly intervals for 3 months and then every 6 months, until their last follow-up. Flexion and extension radiographs were done at the end of 3 months and then at 12 months, or at their last follow-up, to look for any implant-related complications, instability, or inadequate bone formation. Neurological and functional assessments were done at each follow-up, using ASIA and VAS grading, as well as ODI and SCIM scores.
Results
In retrospective data retrieved after 2 years, 28 cervical trauma patients were operated on, out of which 22 patients met the inclusion criteria and were included in the study. One patient expired in the postoperative period due to pulmonary complications and was excluded from the study. The included patients had an approximate male-to-female ratio of 5:2 (15 males, six females) with a mean age of 45.3 years (range, 18 to 70 years). Out of 21 patients, 19 had AO type C injuries and were managed with ACDF, and 2 patients with AO type B injuries were managed with ACCF (Table 1). The levels involved were C3–C4 (1), C4–C5 (4), C5–C6 (10), and C6–C7 (6), with C5–C6 being the most common level. The mechanism of injury was observed to be a fall from height in 14 patients (66.6%) and road traffic accidents in seven patients (33.3%). The average duration of the follow-up period was 16.8 months (range, 11 to 29 months). Fifteen patients had a complete cord injury (ASIA A), while six patients had an incomplete cord injury (two ASIA B, three ASIA C, and one ASIA D). Out of 19 patients with AO type C injuries, 13 patients were found to have a bilateral facet dislocation, while six patients had a unilateral facet dislocation. Seventeen patients underwent a closed reduction under GA on the table before surgery, while two patients had to be put on Crutchfield tongs as their pulmonary condition needed optimization before surgery. Out of the 17 patients, a complete reduction was achieved in 12 cases, while another five needed intraoperative manipulation. In one patient, a reduction could not be achieved despite intraoperative manipulation. Staged posterior instrumentation with lateral mass screws and posterolateral fusion was done for the patient, and a complete fusion was achieved by the final follow-up (Fig. 2). Overall, 19 patients underwent ACDF with bone grafts from the iliac crest (15 patients) (Fig. 3) or a PEEK interbody cage (four patients), and two patients underwent ACCF with a mesh cage (Fig. 4).

Demographic summary
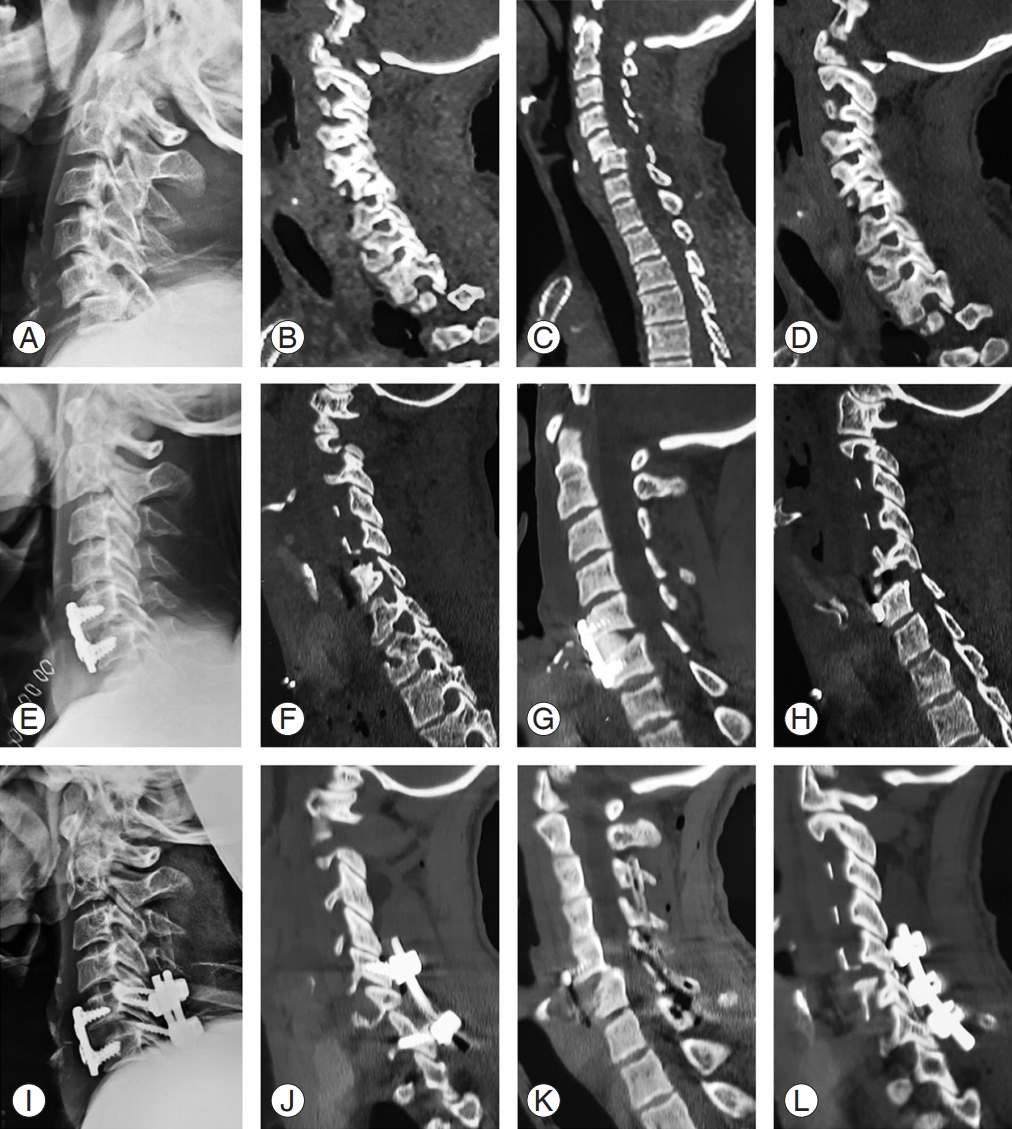
Radiology of a 45-year-old male with an AO type C injury. Preoperative (A) lateral X-ray and CT images in (B) right parasagittal, (C) midsagittal, and (D) left parasagittal sections. Post anterior cervical discectomy and fusion (stage 1) (E) lateral X-ray and CT images in (F) right parasagittal, (G) midsagittal, and (H) left parasagittal sections showing persistent facet subluxation. Post posterior instrumentation (stage 2) (I) lateral X-ray and CT images in (J) right parasagittal, (K) midsagittal, and (L) left parasagittal sections with a complete reduction of facet joints. CT, computed tomography.

Preoperative NCCT images of a 22-year-old male with an AO type C injury showing (A) right parasagittal, (B) midsagittal, and (C) left parasagittal sections with right facet dislocation and left facet subluxation at the C5–C6 level. Post anterior cervical discectomy and fusion NCCT images in (D) right parasagittal, (E) midsagittal, and (F) left parasagittal sections with a complete reduction of facet joints. NCCT, non-contrast computed tomography.

Preoperative NCCT images of an 18-year-old male with an AO type B2 injury at the C6–C7 level showing (A) right parasagittal, (B) midsagittal, and (C) left parasagittal sections. Post anterior cervical corpectomy and fusion NCCT images in (D) right parasagittal, (E) midsagittal, and (F) left parasagittal sections with evident bony fusion at a 14-month follow-up. NCCT, non-contrast computed tomography.
The mean operative time was 177.3±33.8 minutes, and the average blood loss was observed to be 253.1±109.7 mL. There were no intraoperative complications. Seven patients reported an improvement in neurology by 1 or 2 grades on the ASIA scale, while 14 showed no improvement (Table 2). Radiologically, the mean segmental kyphosis angle at presentation was 12.2°±4.4°, while, in the immediate postoperative period, it was -7.2°±2.5° (p<0.05). At the last follow-up, the mean loss of correction was 2.1°±0.9°. All patients showed bony fusion of the operated levels at the final follow-up. There was no evidence of instability as seen in flexion-extension radiographs at the time of last follow-up in any of the patients.

Neurological outcome
The preoperative mean VAS was 6.8±2.1, which showed a gradual improvement that was recorded over the serial follow-ups with the final mean VAS being 1.8±1.1 (p<0.05). The mean ODI score showed a similar trend with a mean preoperative score of 59.7±11.6 and 34.9±13.4 at the final follow-up (p<0.05). The preoperative SCIM score was 24.8±17.2, which improved to 36.4±23.7 (p<0.05).
Discussion
TCICS occurs as a result of hyperflexion with, or without, a rotational element to the cervical spine. The sub-axial spine is commonly involved, with nearly 70% of cases located in the C4–C7 region [6]. In our data, C5–C6 was the most common level. Falling from a height was found to be the most common mode of injury. Nineteen patients were found to have cervical fracture dislocations, while two patients had a flexion-distraction injury.
Achieving an early reduction of the dislocated facets is the first step in the management of patients with cervical fracture dislocations. Different authors have different recommendations with respect to the technique of the said reduction. A reduction of the dislocated facets can be achieved in the emergency room by the application of cervical traction [7], in the operating room under GA before surgery [8-10], or intraoperatively by distraction after a discectomy [11-13]. We achieved a reduction in 70.5% of patients (12 out of 17) by using a technique involving manipulation on the table under GA without any attempt at a closed reduction by traction; this was to avoid time loss and patient discomfort [12,13]. We achieved a reduction by intraoperative distraction after a discectomy in four patients, and in one patient with persistent dislocation, a staged posterior approach was deemed necessary. All five patients with failed attempts at closed reductions had injuries more than 72 hours old, which could explain the inability to achieve a reduction by manual traction.
Being the most mobile segment in the axial spine, the need for adequate stabilization cannot be overemphasized. Optimal stabilization for TCICS remains controversial due to the lack of randomized prospective trials. From the anterior-only, posterior-only, and combined anterior and posterior stabilization techniques, the combined approach is reported to be superior in terms of biomechanical stability [4,14,15]. Despite the theoretical biomechanical advantage, a number of studies have reported comparable results with anterior-only fixation [14,16]. Anterior-only surgery has less blood loss and a shorter operative time and avoids prone turning of the patient intraoperatively, something that poses a potential risk of losing reduction [7]. Facet reduction by the anterior approach can be achieved via intraoperative manipulation with a distraction technique [17] or, if required, by a facetectomy [18]. Moreover, the anterior-only approach offers direct decompression [19-22], by removing the offending agent and reducing the number of fused segments or the large surface area (i.e., the interbody area) to be fused, and has a lower infection rate [23].
The posterior approach is considered superior to the anterior approach in achieving reduction [24], but in cases with the presence of a retropulsed disc fragment, reduction by a posterior-only approach may lead to further neurological deterioration [25]. The posterior approach is reserved for cases with posterior cord compression due to fractured posterior elements or irreducible fracture dislocation with failed open, or closed, anterior reduction techniques. In our data, a staged posterior fixation was needed in one case with the dislocation persisting after an attempted closed reduction and an attempted anterior reduction with stabilization.
None of the patients in our data showed a worsening of their neurology. An improvement in neurology was seen in 33.3% of patients (7 out of 21). Among the patients with an incomplete spinal cord injury, four out of six patients showed an improvement in their ASIA grade, and five out of six patients achieved an ambulatory status after surgery. A significant improvement in VAS, ODI, and SCIM scores was seen at the final follow-up in all the patients. The neurological and functional outcomes were comparable to other studies describing the management of TCICS with posterior or combined approaches [7,12-14,16]. Radiologically, the segmental kyphosis angle showed significant improvement at the final follow-up (-5.1°±1.4°) when compared to the preoperative kyphosis angle (12.2°±4.4°, p<0.05). There was a mean loss of 2.1° of correction between the immediate postoperative period and the last follow-up. This can be explained due to interface bone resorption in cases that used an iliac crest bone graft or minimal cage subsidence in cases using a PEEK or mesh cage. Achieving and maintaining a reduction of the facet joints is the most important factor when determining the correction of kyphosis deformity in cases of cervical fracture dislocations. These results are comparable to other studies evaluating the radiological outcomes of surgically managed patients with cervical fracture dislocations [14,16]. A facet reduction was achieved in all our patients, and follow-up imaging showed bony fusion in all our cases. None of our patients had any instability or implant-related complications at the final follow-up.
This article has a few limitations: the study design being retrospective could lead to bias, the small sample size, and the short follow-up period.
Conclusions
Most patients with TCICS can be managed by anterioronly stabilization with good neurological, radiological, and functional outcomes with a minimal complication rate. Further randomized prospective studies are required for a better comparison with the combined approach.
Notes
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conception and design: SSS; data acquisition: SSS, BS, PK; analysis of data: SSS, KA, SI, BS, PK; drafting of the manuscript: SSS; critical revision, KA, SI; supervision: KA, SI, BS, PK; and administrative support: BS, PK