Introduction
Work-related low back pain (LBP) is a serious socioeconomic problem because of the large economic costs, including direct costs (medical costs, such as medication and physical therapy) and indirect costs (absences and decreased productivity). Studies have shown that the physical and psychological load at work can cause workrelated LBP. Flexion and rotation of the trunk and lifting are risk factors for LBP [1]. In addition, the prevalence of back pain increases as the number of working hours spent on repeated strenuous physical activities and repeated bending, twisting, or reaching increases [2]. Regarding psychological factors, job satisfaction, monotonous tasks, work relationships, demands, stress, and perceived ability to work are related to future back pain problems [3]. The prevalence of LBP among nurses worldwide is particularly high [4-8]. Among the various tasks that nurses perform, independently transferring patients between beds and chairs poses a high risk for LBP because of the large lumbar load [9]. Thus, attempts to decrease the lumbar load are crucial to avoid the risk of LBP. Previous studies have evaluated the effects of interventions, such as electromechanical lifts and sliding lift sheets, to reduce the lumbar load during patient transfers [10-12].
There are few reports evaluating the lumbar load for nurses using a wearable robot. Therefore, we investigated the hybrid assistive limb (HAL) for Care Support (Cyberdyne Inc., Tsukuba, Japan). The HAL is a novel robot suit that was developed to assist joint motion. It can provide interactive motion according to the wearer’s voluntary motor drive. Various types of HALs, such as those for lower limbs, for single joints, and for lumbar support, have been used for musculoskeletal and neurological disorders, including cerebral infarction, spinal cord injury, myelopathy, and osteoarthritis [13-15]. The HAL for Care Support substitutes hip joint motion for trunk motion and assists hip joint extension, which thereby reduces the lumbar load during lifting. It comprises an exoskeletal frame, power units, and lumbar and thigh molds. Tightening the lumbar mold enables trunk motion restraint. The torque assisting the wearer’s hip extension is affected by actuators within power units located bilaterally on the wearer’s greater trochanters. Nerve and muscle action potentials of the lumbar erector spinae are detected as bioelectrical signals (BES) through electrodes attached to the skin so the HAL for Care Support can sense the wearer’s intention to lift something. Moreover, the absolute angle of the trunk is measured by a triaxial accelerometer within the exoskeletal frame. The relative angles of the hip joint are measured by angular sensors within the power units and potentiometers. It is possible for motion supports to coordinate the level and timing of the torque because of these mechanisms of the HAL for Care Support, which comprises a hybrid control system composed of two subsystems: the cybernic voluntary control (CVC) and cybernic autonomous control (CAC) systems [16]. The CVC system performs concerted support that reflects the wearer’s voluntary motion thorough BES. The CAC system performs compensatory support against gravity on the wearer’s weight to decrease the moment induced by trunk flexion. In addition, the HAL for Care Support can be easily put on without the help of others in a few minutes. The wearer can even run and jump without difficulty. Thus far, the HAL for Care Support has been reported to reduce lumbar loads and improve task performance in repetitive lifting and snow-shoveling movements [17,18]. However, our search of the literature revealed no studies evaluating lumbar load during patient transfer movements using the HAL for Care Support. The aim of the present study was to determine whether the HAL for Care Support could reduce the lumbar load during a patient transfer.
Materials and Methods
1. Participants
Inclusion criteria for this study were volunteer participants aged 20–45 years who were healthy, injury-free, and suitable for the HAL for Care Support. Volunteers with heart and respiratory diseases undergoing medical treatment and with LBP were excluded. Nineteen volunteers (16 men, three women) participated in this study. The mean age of the volunteers was 31 years (range, 27–45 years); the mean height was 172±8.9 cm (range, 155–184 cm), and the mean weight was 66±11 kg (range, 47–85 kg). The mean finger-to-floor distance, which demonstrates the flexibility of the trunk, was 4.0±7.4 cm (range, -11 to 16 cm). The mean back-muscle strength (as measured by TKK5402; Takei Scientific Instruments Co., Niigata, Japan) was 110±59 kg (range, 51–170 kg). Informed consent was obtained from all participants in this study. The study was performed in accordance with the Declaration of Helsinki and within the appropriate ethical framework (IRB approval no., H27-50).
2. Patient transfer protocol
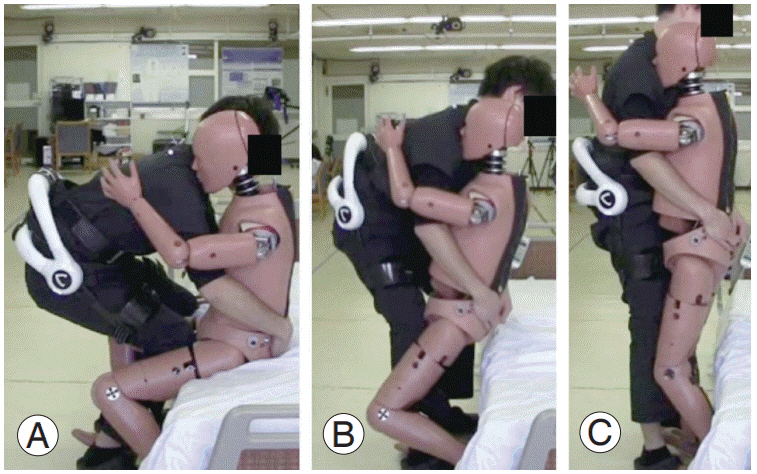
The subject for transfer was a doll weighing 60 kg, which simulated a patient with complete cervical spinal cord injury. Initially, the doll was in a seated position at bedside. Participants adopted a half-seated position to initiate the transfer. The doll’s arms were placed on the participant’s shoulders. Participants held the doll in their arms and lifted it until the doll was in a standing position (Fig. 1). The first transfer was performed without the HAL for Care Support. After a resting period of at least 5 minutes, the second transfer was conducted with the participant wearing the HAL for Care Support suit.
3. Outcome measures and statistical analysis
We evaluated the transfer performance and lumbar load and determined whether participants could lift the doll to a standing position. A visual analog scale (VAS) score for lumbar fatigue (maximum score, 100 mm) was determined after each trial to evaluate the lumbar load. Furthermore, wireless surface electromyogram analyses (Trigno Lab System; Delsys Inc., Natick, MA, USA) with six electromyogram sensors bilaterally attached to the latissimus dorsi, lumbar elector spinae, and gluteus maximus were conducted to evaluate muscle activity during the transfer. Participants were asked to report adverse events during the transfer for the safety evaluation of the HAL for Care Support in this transfer protocol. A Wilcoxon signed-rank test was used to compare variables when transferring patients with and without the HAL for Care Support. All statistical analyses were performed using the JMP software package ver. 14.0.0 (SAS Institute Inc., Cary, NC, USA). For all comparisons, p<0.05 was considered significant.
Results
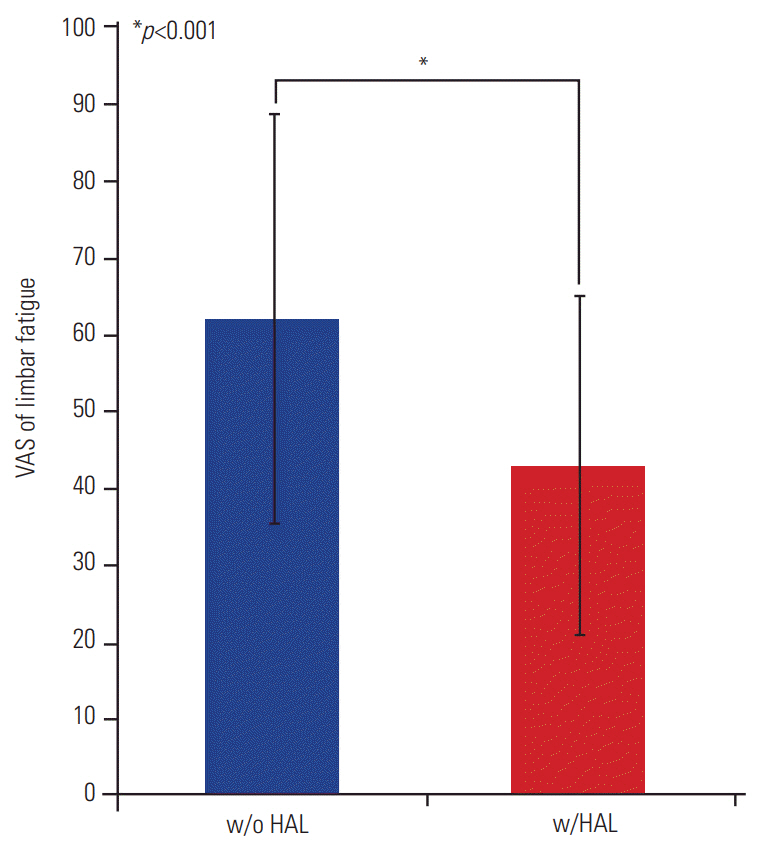
The transfer was completely accomplished by 14 of the male volunteers regardless of whether they were equipped with the HAL for Care Support. Four participants (two men, two women) succeeded with the transfer using the HAL for Care Support even though they could not succeed without it. Only one female volunteer could not accomplish the transfer task regardless of whether she used the HAL for Care Support. The mean VAS score of lumbar fatigue for all participants without the HAL for Care Support was 62±26 mm (range, 7–91 mm), while that with the HAL for Care Support was 43±22 mm (range, 0–79 mm) (Fig. 2). With lumbar support from the HAL for Care Support, subjective lumbar fatigue during the transfer decreased significantly. Muscle activity could not be evaluated in 10 participants because of noise in the electromyograms. We analyzed the muscle activity of the eight participants whose electromyograms could be evaluated. Only the activity of the left gluteus maximus increased significantly during the transfer with the HAL for Care Support compared with the transfer without the HAL for Care Support. The activity of the other muscles did not significantly change. There were no adverse events when using the HAL for Care Support for transferring the doll.
Discussion
It has been recognized that many nurses have musculoskeletal disorders because of their heavy workload. There are many studies on the particularly high prevalence of LBP among nurses worldwide [4-8]. Several systematic reviews have summarized the prevalence of LBP. Hignett [19] reported that the annual prevalence of LBP ranged from 40% to 50%, and the lifetime prevalence ranged from 35% to 80%. Azizpour et al. [20] showed that the prevalence of LBP during working life and during a year was estimated at 63% and 61.2%, respectively. Lorusso et al. [21] reported that the 12-month prevalence of LBP ranged from 33% to 86%. Of the nursing tasks causing LBP, manually transferring patients between a bed and a chair is significantly associated with an increased risk of back pain [9,22]. Moreover, the spinal biomechanical load during a patient transfer exceeds tolerance limits, and patient transfer is associated with a risk of low back disorder [23]. To avoid the risk of LBP in nurses, training or education, no-lift policies and several devices to assist patient transfers, including battery-powered lifts, sliding boards, and ceilingbased patient lifts, have been attempted [10-12]. However, these interventions have not been established to prevent LBP because there is no strong evidence for their efficacy according to systematic reviews [24-26].
In the present study, we evaluated the safety of the HAL for Care Support and investigated whether it could reduce lumbar load and improve performance during the transfer of a doll that simulated a patient with complete cervical spinal cord injury. No adverse events occurred while participants were using the HAL for Care Support for this task. Without the HAL for Care Support, five of the 18 participants failed in the simulated patient transfer.
However, with the HAL for Care Support, four of these five participants succeeded, which indicates the HAL for Care Support could improve transfer performance. The HAL for Care Support significantly reduced subjective lumbar fatigue. A power analysis indicated adequate statistical power to determine differences in the VAS score of lumbar fatigue (0.99). Detecting muscle activity was a problem during the analysis because the electromyograms of approximately half of the participants could not be evaluated due to noise. In the eight participants whose electromyograms could be evaluated, only the activity of the left gluteus maximus increased significantly during the transfer with the HAL for Care Support compared with the transfer without the HAL for Care Support. The HAL for Care Support replaces trunk motion with hip joint motion and assists extension. The HAL for Care Support might increase the muscle activity of the gluteus maximus by assisting the hip joint motion so that participants can perform the simulated patient transfer movements more easily.
There are some limitations to the present study. Only the vertical movement of a patient was simulated and evaluated in this study. In addition to a vertical load, actual patient transfers require a trunk rotational load. Electromyogram analysis linked to motion analysis, such as that in the joint angles of the trunk and hip, remains to be investigated for more precise biomechanical evaluation. Additionally, initial implementation costs and maintenance costs are required to use the HAL for Care Support. Thus, its cost-effectiveness compared with other interventions should be considered. Further studies with highquality study designs are needed to confirm that the HAL for Care Support can reduce lumbar load.