Introduction
The spine and the body function within a cone of equilibrium with focus in maintaining sagittal and coronal alignment with minimum energy expenditure. This happens with a harmonious relationship involving cervical lordosis (CL), thoracic kyphosis (TK), lumbar lordosis (LL), and pelvic anatomy. The purpose is mostly to maintain a mechanical balance in the sagittal and coronal planes centered from the center of the cranial mass, femoral heads, and lower extremities [1]. Many authors have reported that sagittal balance rather than coronal balance is significantly correlated with health-related quality of life, especially in patients who received surgical treatment [2-4]. Therefore, more attention is often paid to sagittal balance than coronal balance during spinal deformity assessment, surgical plan-making, and surgical procedure. Generally, sagittal imbalance results in increased muscular effort and energy expenditure, causing pain, fatigue, and disability [5]. Sagittal imbalance of the spine as a crucial factor in the pathogenesis of myelopathy is supported by several reports [6,7]. Multiple studies have described normative values for parameters of spinopelvic alignment in different populations of varying ages and pathologic conditions. In these studies, the interrelation of pelvic parameters, LL, TK, sagittal imbalance, and its effect on the quality of life and patient outcome has been well-established [5,8,9]. Many studies have reported that pelvic incidence (PI), a constant morphological parameter in each individual, has a significant influence on sagittal alignment of the lumbar spine or the thoracic spine, such as LL and TK [10]. The correlation between the cervical and thoracic spinal parameters is weaker than that between the lumbar and pelvic spinal parameters [11,12]. We started our study with the hypothesis that the overall sagittal balance of the thoracolumbar and lumbosacral spine is expected to influence the cervical spine, with the justification that the cervical spine is not an independent unit because it is connected to the thoracic spine. The aim of this study is to explore the correlation between the lumbosacral parameters and cervical sagittal balance, hoping that the results could provide guidance for changing these primary contributors in correction surgery.
Materials and Methods
1. Materials
The study was conducted prospectively over a period of 1 year in Guilan University of Medical Sciences (Poorsina Hospital) after obtaining approval from the institutional review board and ethics committee (approval no., IR.GUMS.REC.1396.278). Informed consent was obtained from all individual participants included in the study. A total of 420 adult volunteers were placed in four groups (each contains 105 subjects). Inclusion criteria for each group were as follows: group 1 (lumbar subjects) includes patients with lumbar pain or lower limb radiculopathy; group 2 (cervical subjects) includes patients with cervical pain or upper limb radiculopathy; group 3 (post-cervical surgery subjects) includes patients undergoing cervical discectomy and fusion or laminectomy/laminoplasty without initial cervical deformity; and group 4 (normal subjects) includes asymptomatic volunteers without any complaints of low back, hip, or knee pain and no diagnosis or treatment related to the whole spine. The exclusion criteria were age lesser than 18 years, history of spinal trauma, history of bony diseases, and radiologic abnormalities, including degenerative changes, osteophyte formation, or global sagittal imbalance more than 5 cm from the sagittal vertical axis (SVA). A whole-spine lateral radiograph (91.44-cm cassettes) was obtained in a natural standing upright position with the head and trunk vertical and looking straight ahead and elbows fully flexed and fists resting on clavicles.
2. Measurements
All radiographical evaluation was performed digitally by two neurosurgery residents using the picture archiving and communication system. Measured radiographic parameters included the occipitocervical (C1C2 Cobb angle, OCC2 Cobb angle), cervical (C2C7 Cobb angle, C2C7 Harrison angle, OCC7 Cobb angle, C7 slope), thoracic (thoracic inlet angle [TIA] and TK), spinopelvic (LL, sacral slope [SS], PI, and pelvic tilt [PT]), and C7 SVA. Definitions of the radiographic parameters are summarized in Table 1 [13].
All data were analyzed with the IBM SPSS ver. 24.0 software (IBM Corp., Armonk, NY, USA). DŌĆÖAgostino kurtosis and skewness normality test was used to examine whether the parameters were normally distributed. To test interobserver and intraobserver reliabilities, in 20 subjects, the parameters were measured at 2 separate times in 2-week interval and the interobserver and intraobserver intraclass correlation coefficients were analyzed by the mean measurement values of each observer. Descriptive data are given as the mean┬▒standard deviation. Correlations between parameters were analyzed with the PearsonŌĆÖs correlation coefficient test, and linear regression models were set up. A p-value of less than 0.05 was considered significant.
Results
1. Normality test
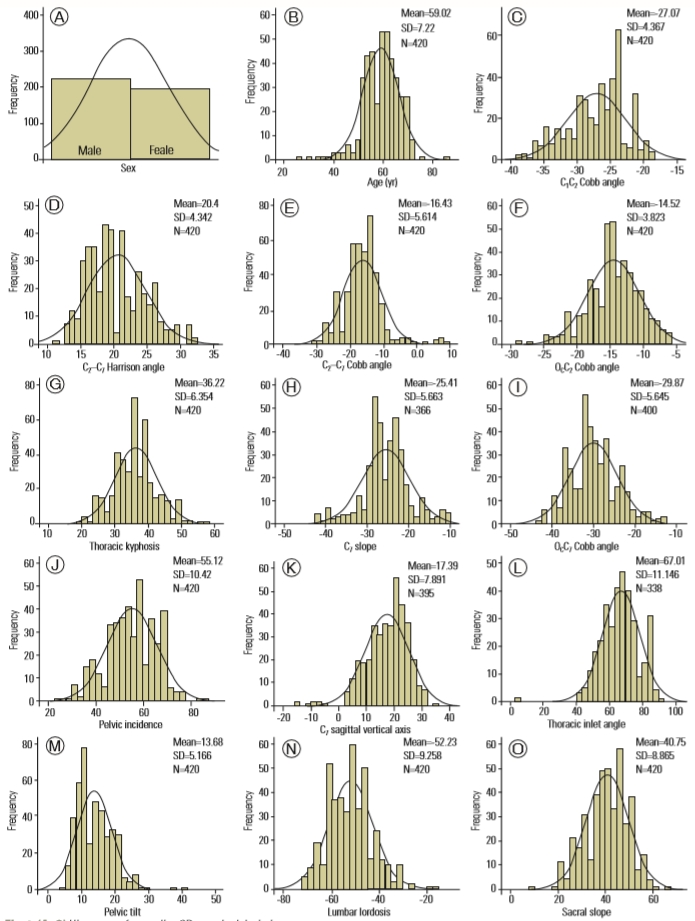
The DŌĆÖAgostino kurtosis and skewness normality test accepted the normality for all the spinal parameters, representing real-valued random variables. Histogram of normality of parameters is shown in Fig. 1.
2. Demographic data
Of the 420 subjects analyzed, 53.1% were males and 46.9% were females with a mean age of 59┬▒7.2 years. No significant differences were found between the asymptomatic, lumbar, cervical, and post-surgical groups, in terms of age and gender. Demographic parameters are given in Table 2.
3. Descriptive results of the spinopelvic parameters
The means of PI, SS, PT, and LL were 55.1┬░┬▒10.4┬░, 40.7┬░┬▒8.8┬░, 13.6┬░┬▒5.1┬░, and ŌłÆ52.2┬░┬▒9.2┬░, respectively. Table 3 summarizes the diagnostic group-stratified means and standard deviations of the performed measurements.
4. Descriptive results of the thoracic parameters
The mean TIA was 67┬░┬▒10.6┬░ (range, 41.5┬░ŌĆō91.5┬░), and the mean TK was 36.2┬░┬▒6.3┬░ (range, 19.5┬░ŌĆō56.8┬░) (Table 3).
5. Descriptive results of the cervical and occipital parameters
The average C1C2 Cobb angle was ŌłÆ27.07┬░┬▒4.3┬░, OCC2 Cobb angle was ŌłÆ14.5┬░┬▒3.8┬░, OCC7 Cobb angle was ŌłÆ29.8┬░┬▒5.6┬░, C2C7 Harrison angle was 20.4┬░┬▒4.3┬░, C2C7 Cobb angle was ŌłÆ16.4┬░┬▒5.6┬░, and C7 slope was ŌłÆ25.4┬░┬▒5.6┬░. The analysis of these parameters revealed no statistically significant difference between the four groups (Table 3).
6. The relationship between the age and cervical spine parameters
In terms of the cervical parameters, only C2C7 Cobb angle correlated with age in the cervical group (Table 4). In the other studied groups, there was no correlation between age and cervical parameters.
7. The relationship between the spinopelvic and cervical spine parameters
The subjects in the cervical group showed positive correlation between the C7 slope and SS (r=0.212, p=0.039) and a negative correlation between C2C7 Cobb angle and PT (r=ŌłÆ0.2, p=0.02). Also, the cervical group showed a statistically significant correlation between the C1C2 Cobb angle and three spinopelvic parameters (LL: r=0.2, p=0.002; PI: r=ŌłÆ0.2, p=0.02; and PT: r=ŌłÆ0.2, p=0.02) (Table 4). In the post-surgical group, PI and SS were two spinopelvic parameters that showed a significant positive correlation to OCC7 Cobb angle and C2C7 Harrison angle (r=0.2) (Table 5). Moreover, C1C2 Cobb angle correlated to PT in the post-surgical group (r=ŌłÆ0.2, p=0.01). Asymptomatic subjects and the lumbar group did not show any significant correlation between the spinopelvic and cervical parameters (Tables 6, 7, Fig. 2).
Regardless of the subgroups (n=420), there was a statistically significant correlation between the C2C7 Harrison angle and PT, C2C7 Harrison angle and PI, C1C2 Cobb angle and LL, and C7 slope and SS. However, there was no correlation between the C2C7 Cobb angle and spinopelvic parameters (Table 8).
8. The relationship between the thoracic and cervical spine parameters
There was significant correlation between C7 slope and TK in the lumbar (r=0.2, p=0.01) and cervical (r=0.2, p=0.03) groups. The TK correlated significantly with the C1C2 Cobb angle in the cervical group (r=0.2, p=0.01) and with the C2C7 Harrison angle in the post-surgical subjects (Tables 4, 5, 7). As with the spinopelvic parameters, there was no correlation between the thoracic and cervical spine parameters in the asymptomatic group (Table 6). Regardless of the subgroups, C7 slope was the only cervical parameter that was associated with TK in all the study subjects (Table 8).
9. The relationship between the occipital and cervical spine parameters
Statistically significant correlation was observed between the OCC2 Cobb angle and C1C2 Cobb angle (r=0.2, p=0.01) and between the OCC2 Cobb angle and C7 slope (r=0.283, p=0.006) in the asymptomatic subjects (Table 6). The lumbar and cervical groups did not show any significant correlation between the occipital and cervical parameters (Tables 4, 7). Regardless of the subgroups, both studied occipital parameters correlated with the C1C2 Cobb angle (OCC2 Cobb angle: r=0.173, p=0.000 and OCC7 Cobb angle: r=0.1, p=0.02) (Table 8).
10. Multiple regression analysis and the linear regression model
Multiple linear regression analysis was used regarding C0C7 angle (CL) as a dependent variable and regarding C0C2, TK, PI, and LL as independent variables to model the relationship between C0C7 angle and potential factors by fitting a linear equation to the data. The equation for predicting the alignment of CL was as follows: C0C7 angle=0.15 (C1C2)+0.8TK+0.03PIŌłÆ0.04LLŌłÆ32.
Discussion
In the past decades, much emphasis has been placed on identifying the sagittal profile of the thoracolumbar spine. In contrast to numerous discussions about the relationship between spinopelvic parameters and global sagittal balance of the spine, the correlation between spinopelvic parameters and cervical sagittal balance is unclear. The cervical spine is a relatively complex segment, and many factors influence its alignment and balance. The identification of compensatory mechanisms can be a precious point for the appropriate reconstruction of cervical spine alignment, especially in patients who have undergone spinal surgeries.
In terms of normal values, the measured values vary widely in different studies. It seems that factors, such as age, sex, race, and method of measuring parameters, cause this disparity. Nunez-Pereira et al. [14] studied the interdependences between occipitocervical and spinopelvic parameters. They reported mean values for OCC2 and C2C7 Cobb angles as ŌłÆ12.7┬░ and ŌłÆ15.8┬░ for asymptomatic subjects, ŌłÆ10.4┬░ and 18.9┬░ for patients with cervicalrelated symptoms, and ŌłÆ11.9┬░ and ŌłÆ21.2┬░ for post-surgical patients, respectively. In our study, OCC2 angle was ŌłÆ14.7┬░ for the asymptomatic patients, ŌłÆ14.3┬░ for the patients with lumbar-related symptoms, ŌłÆ14.4┬░ for those with cervicalrelated symptoms, and ŌłÆ14.5┬░ for post-surgical patients. The C2C7 Cobb angle was ŌłÆ15.4┬░, ŌłÆ16.8┬░, ŌłÆ17.1┬░, and ŌłÆ16.34┬░ in our four study group, respectively. These results are similar to those of Nunez-Pereira et al. [14] relatively. Also, the total amount of CL (OCC7 Cobb angle) in our study was similar to that of previous studies (ŌłÆ29.8┬░┬▒5.6┬░) [14,15]. A study of Guo et al. [15] showed slight differences with regard to age in the occipitocervical alignment of healthy volunteers. In our study, age correlation was observed only with C2C7 Cobb angle and C2C7 Harrison angle for patients with cervical-related symptoms. The age-related structural changes in the spine justify this difference.
Several studies have implied that the lumbar and pelvic parameters are correlated with the cervical region values. In our study, the mean value of LL was ŌłÆ52.2┬░┬▒9.2┬░, SS was 40.7┬░┬▒8.8┬░, PI was 55.1┬░┬▒10.4┬░, and PT was 13.6┬░┬▒5.1┬░. The analysis showed no correlation between the spinopelvic and cervical parameters in asymptomatic and lumbar patients. However, C1C2 Cobb angle correlated with the three spinopelvic parameters (LL: r=0.2, p=0.002; PI: r=ŌłÆ0.2, p=0.02; PT: r=ŌłÆ0.2, p=0.02), and the C2C7 Cobb angle correlated with PT (r=0.2, p=0.02) in cervical symptomatic patients. These results are consistent with those of Nunez-Pereira et al. [14] and Lee et al. [16]. Shao et al. [17] performed measurements in asymptomatic healthy volunteers and found that CL correlated with LL (r=0.1, p<0.01) and OCC2 Cobb angle correlated with SS (r=ŌłÆ0.1, p<0.05). In our study, regardless of the patientsŌĆÖ symptoms (n=420), C1C2 Cobb angle correlated with LL (r=0.1, p=0.01) and C2C7 Harrison angle correlated with PI (r=0.1, p=0.04) and PT (r=0.12, p=0.003). It seems that pain promotes compensatory flexion to increase spinal canal volume that leads to segmental alignment changes, and this can be a factor in the change of the correlation between spinal parameters in patients with cervical pathologies compared to the asymptomatic individual.
In our study, there was no significant correlation between CL (C0C7 Cobb angle) and spinopelvic parameters in asymptomatic, cervical symptomatic, and lumbar symptomatic patients. However, regardless of the patientsŌĆÖ symptoms (n=420), there was a significant relationship between C0C7 angle and PI and LL. This will clarify the key role of sample numbers in evaluating the correlation between the parameters.
Recently, Nunez-Pereira et al. [14] proposed C7 slope as a predictor of the overall sagittal balance of the spine. They believe that if C7 slope is altered on cervical radiographs, a full-length sagittal radiograph should be taken to rule out the overall sagittal imbalance. However, we found a negative correlation between C7 slope and C7 SVA, and, in contrast to Nunez-Pereira et al. [14], this correlation was not statistically significant. Thus, we believe that further studies with higher sample sizes are needed to examine the role of C7 slope in the overall sagittal balance of the spine.
C7 SVA represents the global spinal sagittal alignment; thus, it should have a specific impact on CL to maintain sagittal balance, independent of other parameters. Subjects who had a positive SVA displayed an increase in CL, regardless of whether their SVA was within the normal range of values. This is a compensatory mechanism to maintain a horizontal gaze in response to changes in sagittal global alignment [11]. Interestingly, C7 SVA was the only parameter in our study that showed a significant correlation with the C2C7 Cobb angle in the four groups (r=ŌłÆ0.6 in asymptomatic; ŌłÆ0.8 in lumbar; ŌłÆ0.8 in cervical; and ŌłÆ0.6 in post-surgical subjects). However, there was no correlation between C7 SVA and total CL (OCC7 Cobb angle). Matsubayashi et al. [18] found a similar significant correlation (r=0.5) in normal adults. They divided the C2C7 angle into the C2ŌĆōC4 (middle cervical) and C5ŌĆōC7 (lower cervical) angles and found that C7 SVA correlated with the C5ŌĆōC7 angle but not with the C2ŌĆōC4 angle.
The cervical spine is considered as a unique segment and can be divided into two sub-segments with different roles and functions. For example, the highest level of cervical flexion and rotation is seen in the upper cervical segment (C0C1 and C1C2) whereas the lower segment (C2C7) is associated with lateral bending [19,20]. Therefore, the difference in correlation between these two cervical subsegments and the spinopelvic parameters is not surprising. According to our study results, it seems that spinopelvic parameters (such as, PI, PT, and LL) show greater correlation with the upper cervical segment (C1C2 Cobb angle) and that the total CL and the sub-axial parameters (C3ŌĆōC7) are less affected.
The prospective design and the survey of symptomatic subjects parallel to the asymptomatic individuals are the benefits of our study. This heterogeneity in patient selection facilitates the understanding of the general functions of the cervical spine, but it should be kept in mind that standard sampling and large sample size are the prerequisites of assessment of correlation in any population. Thus, the number of subjects may have underpowered our results. There are structural differences between population groups and races [19-21]. Therefore, this should be considered when comparing the results of various studies in different regions and races. We have not studied the correlation between some of the occipitocervical parameters, such as occipital incidence and occipital slope. It is therefore recommended to study their effect on cervical alignment in subsequent studies. Further study with a larger number of cases in various spinal disorders in different races should also be performed to obtain actual spinal sagittal balance.
Conclusions
Our results indicate significant interdependence between the spinopelvic and cervical alignment, especially in cervical symptomatic patients. In addition, strong correlations were found between the C7 SVA and C2C7 Cobb angle. Overall, the results of this study could help to better understand the cervical sagittal alignment and serve as preliminary data for planning surgical reconstruction procedures.