Introduction
Humans are the only primates capable of maintaining an upright, totally vertical, bipedal posture. Unlike the spine of other primates, the human spine has successive opposing curves that allow the trunk to assume an erect position. Although all primates can walk bipedally, only Homo sapiens can do so for a long period. This is mainly because of the lumbar lordotic curvature. The adoption of an upright vertical posture by humans resulted in a broad, vertical pelvis and the characteristic curves of the spine [12345].
Sagittal balance and spinopelvic organization are crucial for the diagnosis and treatment of lumbago and degenerative spine disease. Even the genesis of spinal deformities has been linked to the three dimensional spatial orientation of the spine and pelvis [36].
For the treatment of many spinal deformities, analysis of the morphology of the spine in the sagittal plane is essential. The morphology of the spine can be assessed with the aid of whole spine standing sagittal radiographs, in which the beam is centered on the 12th thoracic vertebra and the radiograph is taken during inspiration. The patient stands up naturally, looking horizontally, with the hands resting on a vertical support or with the fingertips on both cheeks or clavicles, the upper limbs relaxed, and the elbows half-bent [789].
The pelvis and spine as a whole in the sagittal plane can be considered a linear linking chain that connects the head with the pelvis. The shape and orientation of each segment are closely interrelated with one another and influence one another to maintain a stable posture with minimum energy expenditure. Changes at one level will affect other levels. The morphology and spatial orientation of the spine and pelvis can be described by a few radiographic parameters that can be classified as spinal and pelvic parameters which are measured in degrees. The pelvic parameters are pelvic incidence (PI), sacral slope (SS), and pelvic tilt (PT). The spinal parameters are lumbar lordosis (LL) and thoracic kyphosis (TK) [8101112].
Spondylolisthesis is a sagittal plane deformity resulting in slipping of one vertebra over the one below. It has been proposed that a higher PI correlates with a higher incidence of spondylolisthesis. Studies have shown differences in the normative values of spinopelvic parameters in different populations and ethnic groups [6910111213]. A correlation between spinopelvic parameters and the incidence of spondylolisthesis has not been reported in the Indian ethnic population. We started our study with the hypothesis that patients with spondylolisthesis have a higher PI. We aimed to confirm the hypothesis in our subset of patients. We also aimed to determine if these parameters were significantly different in patients with low-grade and high-grade listhesis and also to determine the response to conservative treatment.
Materials and Methods
2. Study participants
The study enrolled 75 asymptomatic (control) volunteers and 79 patients with spondylolisthesis attending the orthopedic outpatient department. All controls and patients were aged >18 years. The study was conducted in Jawaharlal Institute of Postgraduate Medical Education and Research after obtaining approval from the institutional review board and ethics committee of Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER-PGRMC/140/2013). The study was conducted over a period of 2 years.
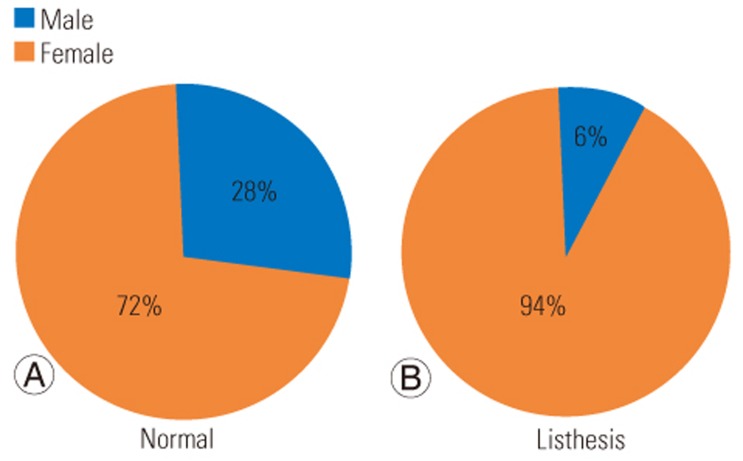
The control group comprised 75 asymptomatic volunteers without any complaints of low back, hip, or knee pain and no contraindication for radiographic exposure (Table 1). The spondylolisthesis group comprised 79 patients (five males and 74 females; mean age, 43 years) with developmental or degenerative spondylolisthesis according to the classification of Marchetti-Bartolozzi irrespective of the level [14] (Table 1, Fig. 1). For all the patients after a detailed clinical examination and relevant investigations patients with deformity of the spine (other than spondylolisthesis), spinal fracture, spinal tumor, infection of the spine, previous surgeries to the spine, contraindication to radiographic exposure, or hip or knee disorders were excluded from the study.
3. Procedure
At their initial visit, patients with spondylolisthesis had a standing sagittal, lateral radiograph, and the functional score was assessed by modified Oswestry questionnaire that had been converted into the patient's vernacular language. The patients were given a trial of conservative treatment according to the hospital's standard physiotherapy protocol and evaluated every 6 weeks. The functional score was assessed with the aid of the Oswestry questionnaire at 6 weeks, 3 months, and 6 months. At the end of 6 months, patients who improved were followed up with the same protocol; those who worsened a repeat radiograph was taken for comparison and were advised to have surgery [15]. The spinopelvic parameters measured were PI, SS, PT, TK, and LL [45].
4. Radiographic protocol
One standing lateral radiograph of the spine was obtained from each subject in a standardized fashion, with the patient standing up naturally, looking horizontally, with the hands resting on a vertical support, the upper limbs relaxed, and the elbows half-bent. Three cassettes of size 35.56├Ś43.18 cm (14├Ś17 inches) were used for each subject. The cassettes were placed on a vertical platform and the subject stood in front of the platform in the standard position. The subject was at a distance of 2 m from the radiographic source, and a single X-ray was taken centering around D12. The radiograph included film from C7 to the femoral heads for calculating the parameters. The parameters were calculated with the use of free Surgimap spine software ver. 2.1.2 (Nemaris, New York, NY, USA). Surgimap, a Nemaris innovation, is a stand-alone, freeware application [1617].
5. Physiotherapy protocol
The hospital's standardized physiotherapy protocol was tailored according to the patient's functional and clinical status.
6. Statistical analysis
Descriptive and inferential statistical analysis was performed. Continuous measurements are presented as means┬▒standard deviation (minŌĆōmax), and categorical measurements are presented as numbers (percentage). All data with p<0.05 were considered to indicate statistical significance. Student t-test (two-tailed, independent) was used to determine the significance of differences in study parameters on a continuous scale between the two groups (intergroup analysis) for metric parameters, and Student t-test (two-tailed, dependent) was used to determine the significance of differences in study parameters on a continuous scale within each group. The chi-square test and Fisher's exact test were used to determine the significance of differences in study parameters on a categorical scale between two or more groups.
Results
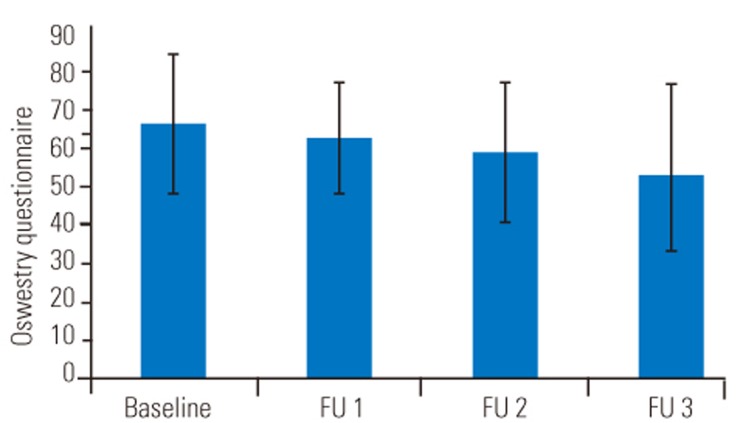
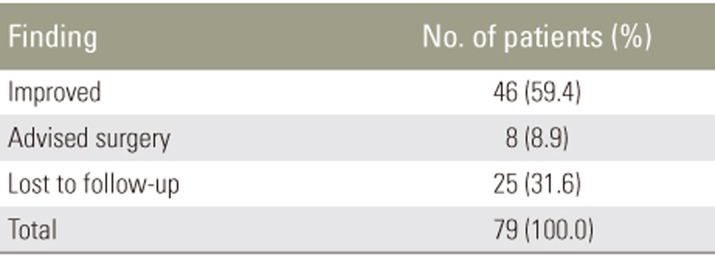
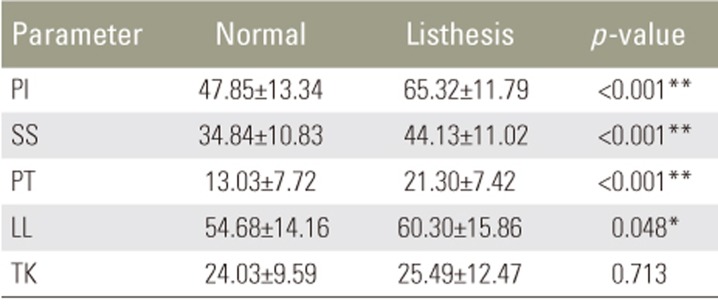
In the cohort of 75 asymptomatic volunteers, we found the following values of spinopelvic parameters: PI 47.85┬░, PT 13.03┬░, SS 34.84┬░, LL 54.68┬░, and TK 24.03┬░. A total of 79 spondylolisthesis patients were followed. Over the follow-up period, majority of patients improved in the functional assessment that was performed using the Oswestry questionnaire (Table 2, Fig. 2). Among the 79 patients, four have 2 level listhesis, so the total listhesis levels were 83. Of the 79 patients with listhesis included in the study, 25 were lost to follow-up and 54 were followed for 6 months; 46 of these patients improved and eight were advised to undergo surgery (Table 3). Repeat X-rays were taken in these eight patients for comparison (Table 4).
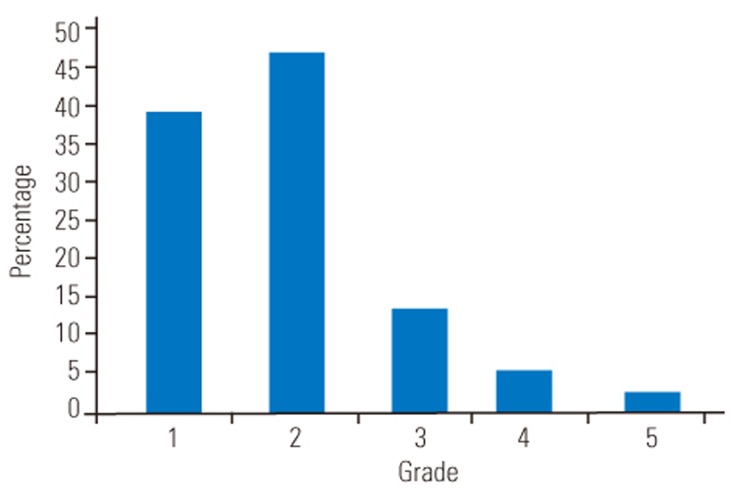
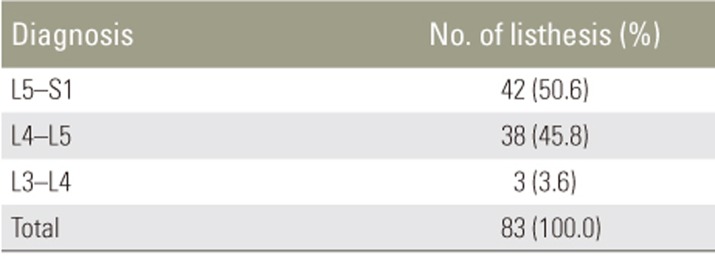
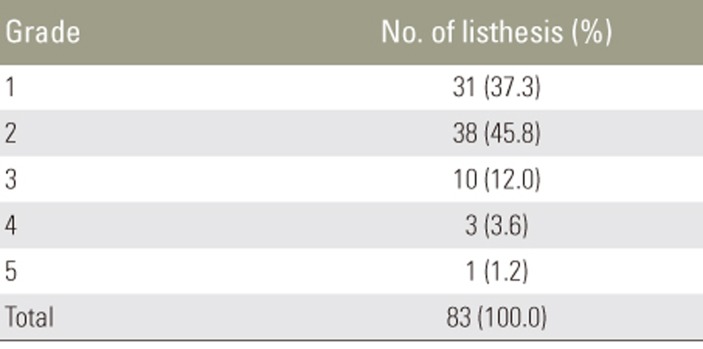
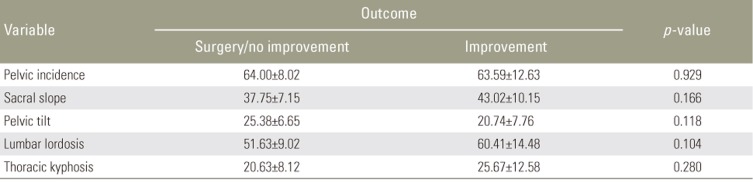
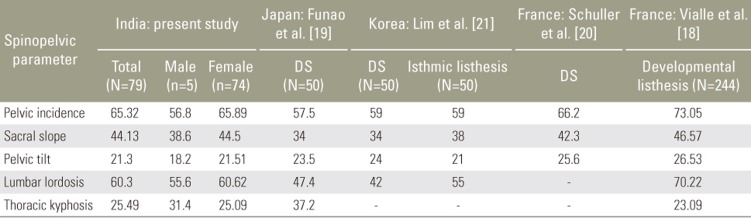
The most common level of listhesis was L5ŌĆōS1, followed by L4ŌĆōL5, and the least common was L3ŌĆōL4 (Table 5, Fig. 3). The most common grade of listhesis was grade 2, followed by grades 1, 3, 4, and 5 (Table 6, Fig. 4). Table 7 compares the spinopelvic parameters between the controls and spondylolisthesis patients. Table 8 compares the spinopelvic parameter according to grade of slip in spondylolisthesis patients. Table 9 compares the spinopelvic according to the outcome in spondylolisthesis patients. Table 10 shows the values of patients with spondylolisthesis in our study in comparison with those determined in other studies [18192021].
Discussion
Roussoly et al. [1] observed four types of spinopelvic alignment in the normal population. Types 1 and 2 are associated with low SS (<35┬░) and low PI. Type 3 is a well balanced spine with SS from 35┬░ŌĆō45┬░. Type 4 is a curved spine (SS>45┬░). The mechanical stresses acting on the spinal column in each of the four spine groups are not the same (Fig. 5). The force acting on the lumbar spine, also called the contact force (CF) is the sum of forward forces (gravity, abdominal pressure) and the force of the posterior spinal muscles. The CF is distributed between the intervertebral discs in front and the facet joints behind. In the curved spine, the CF acts on the posterior elements, and in flat back, CF acts mostly on the discs. The CF acting at each vertebral level can be split into two resultant vectors, one parallel to the end plate and the other perpendicular to it. In hypolordosis, the perpendicular vector force increases and the disc pressure increases. In the case of hyperlordosis when the vertebrae are tilted, the parallel vector has a role in increasing shear forces, resulting in anterolisthesis or retrolisthesis, depending on the tilt of the vertebrae. Hence, hypolordosis causes degenerative disk diseases, whereas hyperlordosis may cause posterior facet arthritis and listhesis [1].
In the type 1 spine, which is a combination of kyphosis and hyperextension area, there is an increased risk of degenerative changes in thoracolumbar kyphosis and a likelihood of spondylolisthesis in the lordotic lumbar segment. There is also a risk of spondylolysis in the hyperlordotic area. In the type 2 spine, which is flat back where the discs are parallel, the pressure is maximum. Hence, there is a risk of degeneration (Fig. 5). In types 3 and 4 spines, there is a risk of listhesis and posterior facet arthritis [1].
In our study, we found that the differences between spinopelvic parameters in patients with spondylolisthesis and asymptomatic controls were significant. As described by Roussouly and Pinheiro-Franco [1], the type 4 spine is associated with listhesis. The type 4 spine has high PI and high slope that is responsible for increased stress at the lumbosacral junction, and also greater force acting on posterior elements, resulting in listhesis. The same result was found in studies by Vialle et al. [18], Funao et al. [19], Schuller et al. [20], and Lim et al. [21] (Table 10). In their studies on patients with different types of listhesis, they found that high PI was associated with listhesis. However, some studies showed a correlation between slip degree and PI while others did not [18192021].
We found that high PI was associated with spondylolisthesis, but we could not find any association with the progression of spondylolisthesis. The patients were followed up for 6 months. Eight of the 54 patients followed had worsening of symptoms and were advised to have surgery; all eight of these patients in their repeat radiographs had progression of the slip.
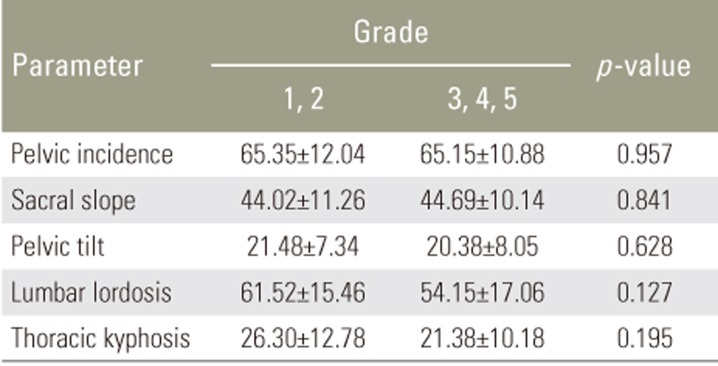
There were no significant differences in any of the measured spinopelvic parameters between those with high-grade and low-grade spondylolisthesis (Table 8) or between patients who improved and those who worsened (Table 9). Thus, we could not attribute the progression of slip to spinopelvic parameters (PI) alone. The patients whose condition worsened had a high PI, two levels of spondylolisthesis, initially compromised spine (sagittal vertical axis >50 mm), and a large slip to start with or connective tissue disorders (one of the patients had Marfans syndrome). We found that PI was associated with the slip but not with its progression. More factors come into play for progression.
Conclusions
Patients with spondylolisthesis had higher PI, SS, PT, and LL than control subjects. These differences were statistically significant. There were no statistically significant differences in the values of the measured radiographic parameters between patients with low-grade and those with high-grade spondylolisthesis. The progression of slip and the clinical and functional response to conservative treatment do not depend solely on spinopelvic parameters, which are poor predictors of the outcome in patients with spondylolisthesis.