Introduction
The calculated global incidence of traumatic spinal injuries (TSIs) is 10.5 cases per 100,000 persons, which is approximately 79,000 cases per year [1]. The costs associated with pain alleviation, disability, social dependence, and health care are high, even in developed countries [2]. Previous studies on the epidemiology of TSI in developed countries demonstrated that proper documentation and analysis of the available data helped to formulate protocols useful for the prevention of spinal trauma and improving patient handling during transport and early care in the emergency room [3]. Oliver et al. [4] documented the changing trends in spinal injuries over a 13-year period and reported that the incidence of cord injuries due to motor vehicle accidents (MVAs) markedly decreased during the study period and identified plausible reasons for this, including improvements in road traffic safety, public health campaigns, automobile safety legislation, and strict implementation of rules.
The literature surrounding TSIs is restricted to developed countries that have existing robust healthcare systems in place, and have focused predominantly on spinal cord injuries and selective spinal regions, such as cervical spinal injuries [1]. Chiu et al. [5] reviewed global epidemiological studies of TSIs over a 20-year period and noted gross differences in the incidence, mortality rate, patients’ age, sex, causes, and severity of injury between developed and developing countries. For example, trauma due to MVAs and falls were the most common modes of spinal injury and fractures worldwide [1,5]. Injuries due to adventure sports, violence, and gunshot were not uncommon in studies in the Western literature, whereas these were absent in developing regions of the world. In developing countries, the incidence of TSI due to falls could be higher than that of MVAs since injuries sustained due to falling from trees and electric poles, construction sites, industries, and falling into wells are common occurrences. Evidently, region-specific epidemiological data on TSI is important since injuries and outcomes are often determined by civil infrastructure, transport systems, strength of health care emergency services and the socioeconomic fabric of the population. Globally, India has the highest incidence of road traffic accidents (RTAs), with a predicted incidence of 55 accidents and 17 deaths per hour [6].
It is intuitive that the information from studies originating from developed countries could be of limited use in planning patient management and health care policy decisions of countries like India, where the number of studies performed to date on the incidence of spinal trauma, causation, and risk factors are too few and inadequate to draw reliable conclusions. One recent epidemiological studied examined only 92 patients with thoracolumbar spine fractures, whereas another multicenter study involving 14 centers across India (2017) only evaluated 192 spine trauma patients to examine the basic epidemiology of spinal injuries [7,8].
Hence, an understanding of the incidence and detailed epidemiology of TSI on a large scale is essential and critical. Such studies would be beneficial to formulate protocols and policies in the management of spinal trauma.
Materials and Methods
1. Study design
This was a retrospective study of consecutive series of spinal trauma patients that were treated between January 2015 and December 2019 Ganga Medical Centre and Hospitals (GMCH), Coimbatore, India. The study was approved by the Institutional Review Board of GMCH (reference no., IRB-GMCH-17.08.19). The requirement for informed consent from individual patients was omitted because of the retrospective design of this study. All patients admitted for spinal injury at the institution were included in the study and patients with pathological fractures were excluded. The details of the patients (Table 1), including age, sex, occupation, time of injury, mode of injury, place of injury, time of hospitalization, systolic blood pressure on arrival, comorbidities, severity of spinal cord injury (SCI), associated axial and appendicular injuries, treatment modality used for spinal injury, medical insurance coverage, patients giving up treatment, and mortality were collected from patient records. Details about the level of spinal injury, number of levels injured, and fracture morphology were collected from the picture archiving and communication system.
2. Statistical analysis
Obtained data were entered into a spreadsheet and analysis was performed using IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented a numbers and percentages and continuous variables were presented as mean±standard deviation and median. Quantitative variables were compared using Mann-Whitney test between the two groups. Qualitative variables were compared using chi-square test and Fisher’s exact test. All p-values <0.05 were considered statistically significant.
Results
The incidence of TSI among all trauma patients treated during the study period was 6.2% (2,065/33,072 general trauma patients had spinal injuries in 5 years) (Table 1).
1. Age and sex
The majority (82.03%, n=1,694) of patients were male and 17.97% (n=371) were female. The mean age of the patients was 43.4±16.3 years, 6.63% were children and young adults, and 16.1% were aged >60 years. A total of 77.3% of spinal trauma patients were aged 20–60 years and the median transit time of transportation of the patient to hospital was 20 hours.
2. Causes of spinal trauma
The major causes of spine trauma were falls from a height (52.1%, n=1,069), MVAs (42.0%, n=862), heavy objects landing on the spine (4.5%, n=93), and injuries caused by animals (1.2%, n=24). Only two cases of assault-related spinal trauma were documented.
Among spinal injuries caused by falls, the majority (40.6%, n=434) were falls from a height of 10–30 feet (3.048–9.144 m). Falls included injuries incurred due to a fall from high structures and those into deep wells. In 17.5% (n=187) of patients, the injury was sustained by falling from <10 feet (3.048 m) and in 9.2% (n=98), it occurred from a fall from >30 feet (9.144 m). Furthermore, 14.9% (n=159) of TSIs due to falls were attributable to slip and fall on a flat surface and predominantly involved elderly patients (>60 years). In 18.2% of patients, specific information on the altitude could not be retrieved due to various factors, including poor general condition on arrival, multiple distracting injuries, low Glasgow Coma Scale, postinjury amnesia, and alcoholism.
In patients who sustained injuries due to falls, the places the injury occurred were the workplace/industry (n=376), home (n=309), from a tree (n=151), into a well (n=77), and from an electric pole (n=57). None of the injured persons who sustained injuries due to a fall at work were wearing protective equipment or harnesses.
Among the 862 patients who sustained TSIs in MVAs, 52.2% (n=467) were riding motorcycles, 21.8% (n=188) were in a light motor vehicle (car), 6.3% (n=54) were traveling in a heavy motor vehicle (bus/lorry), and 5.2% (n=45) were pedestrians. Among the 467 motorcycle accidents, 287 (61.5%) occurred due to a self-skid without any collision, 17.9% (n=84) were due to collisions with a car, 50 (10.7%) were due to collisions with other motorcyclists, and 40 (8.6%) involved collisions with heavy vehicles.
3. Social strata of patients
Around half of all injuries (53.5%, n=1,005) occurred in people in lower socioeconomic strata who worked in agriculture, construction, and manual labor. Socially and economically dependent individuals, including students, homemakers, unemployed, and retired people were involved in 20.25% (n=418). On the other hand, 18.2% (n=386) were involved in skilled and professional jobs and were the least affected.
4. Characteristics of spinal injury
The most common injured level of spine was thoracic (37.2%, n=769), followed by cervical (33.1%, n=685), lumbar (25.6%, n=530), and sacrococcygeal (3.9%, n=81). Most patients (77.7%, n=1,604) had single-level injures, whereas 20.3% (n=419) had injuries at two levels. Injuries at three levels were seen in 1.9% (n=38) of the patients and four patients had injuries at four levels. Patients who sustained injuries due to falls had a higher incidence of multilevel fractures.
The AO classification of spine fractures was used to broadly classify the injuries. Based on this classification, 31.4% (n=643) of patients had A type injury, 33.1% (n=679) had B type injury, and 29.3% (n=601) had C type injury. Traumatic disc osteophyte compressions of the cervical spine were seen in 6.2% (n=142) of patients.
SCI was present in 1,011 patients (49.0%), among whom 682 had complete motor neurological injury and 329 had incomplete deficits. Neurological deficit was graded using the American Spinal Injury Association (ASIA) scale and revealed that 571 (27.7%) were ASIA-A, 110 (5.3%) were ASIA-B, 155 (7.5%) were ASIA-C, 172 (8.3%) were ASIA-D, and intact neurology was observed in 1,057 (51.2%). Complete neurological deficit was observed in 40.86% of patients affected by a heavy object land on them.
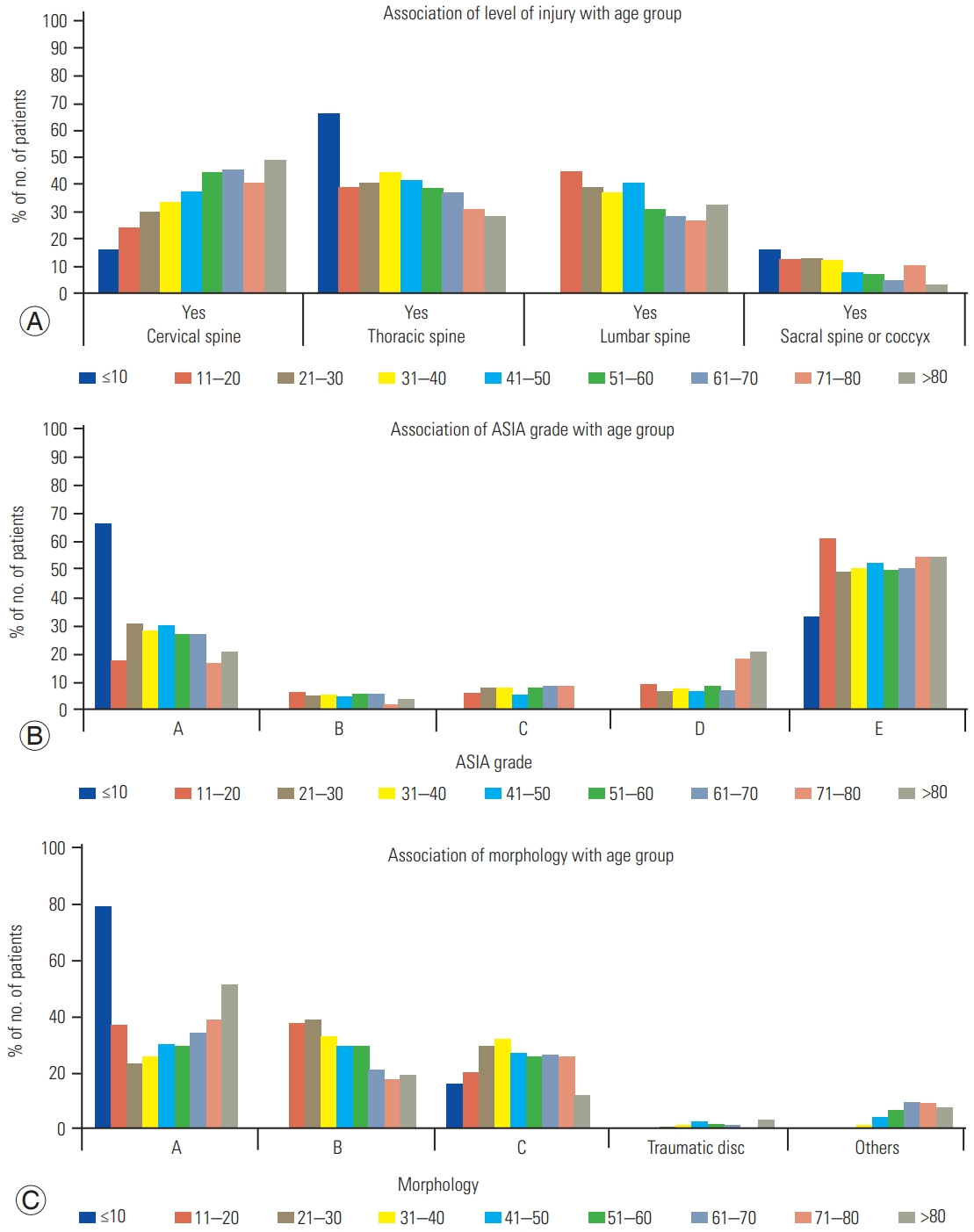
Young patients (<10 years old) had a higher incidence of thoracic injuries (66.6%), whereas older patients (>80 years old) sustained more cervical injuries (50%) (p<0.05). Similarly, the youngest and oldest (<10 years old and >80 years old) patients had a higher incidence of AO type A injuries (p<0.0001) and all types, A–C, were uniformly distributed among the rest of the age groups. There were no specific patterns of neurological deficit in the different age groups, although ASIA-A injuries were higher among younger patients (p<0.01) (Fig. 1).
A total of 75.9% (n=1,567) of patients underwent surgical fixation. The majority (57.1%, n=895) of these patients underwent surgical fixation of spine within the first 24 hours of admission, followed by 26.3% (n=412) during the next 24 hours and 16.6% (n=260) of patients underwent surgery 48 hours after admission.
5. Associated injuries and comorbidities
Around half of all patients (49.7%, 1,028) had injuries associated with other organ systems, such as the head, chest, face, pelvis, and abdomen. Head injury was seen in 427 patients (20.7%), chest injury in 269 (13.0%), facial injury in 80 (3.9%), pelvic injury in 195 (9.4%), and abdominal injury in 56 (2.7%). Comorbidities were documented in 601 patients (29.1%), including diabetes mellitus (15.2%, n=313), hypertension (10.8%, n=223), ischemic heart disease (1.9%, n=40), hypothyroidism (1.1%, n=22), respiratory diseases (1.0%, n=20), ankylosing spondylitis (1.1%, n=23), diffuse idiopathic skeletal hyperostosis (0.7%, n=14), and multiple comorbidities were noted in 54 patients.
6. Hospital stay
The mean and median lengths of stay in hospital after spinal injury were 8.9 days and 7 days, respectively. The mean length of stay reduced from 8.3±2.1 to 6.2±1.7 days during the 5-year study period. Health insurance coverage was only 13.1% among all patients in the present study. A total of 15 out of 2,065 patients (0.7%) died in hospital during treatment.
Discussion
The present study involved a large-scale longitudinal assessment of spinal injuries in the developing world and uniquely encompassed injuries to the whole spine as well as injuries to the vertebral column and spinal cord, which lack data. In a recent systematic review on global epidemiology of TSI, the authors highlighted the lack of information about TSI from developing and underdeveloped countries [1,5]. They noted that the majority of manuscripts included in the review included data from high-income countries (HICs, n=50), whereas only six were from low-income countries (LICs). In their review, the incidence of TSI was higher in (LICs and middle-income countries [MICs]) (13.7 per 100,000 persons) compared with HICs (8.7 per 100,000 cases). The authors were concerned by this paradoxical situation of a lack of studies in regions of the world where the disease was prolific. Hence, the need for large-scale data on TSI and SCI from middle and LICs is clear and relevant, and our study provides important insight.
In the present study, the incidence of TSI among cases of general trauma was 6.2%. The incidence of TSI varies in literature depending on the heterogeneity of the study population. Data from single-center studies provide similar results. Oliver et al. [4] analyzed TSIs over a 13-year period in a level 1 trauma center and observed that 5.8% of all trauma patients suffered spinal fractures. Population-based studies provide an alternative perspective to disease incidence. The average incidence of hospitalized TSI was 26/100,000 in Northern Finland and a higher incidence of 64/100,000 in Canada, while Asian studies have shown incidences varying from 16–62 per 100,000 [9,10].
In developing countries, the mechanism of injury causing TSI was different from that described in the Western literature. In the present study, the majority (52.1%) of spinal trauma was due to falls from different heights, with the most common being from 10–30 feet (3.048–9.144 m). Such falls invariably occurred in construction site workers, industrial workers, tree climbers, and electric pole workers. This indicates the vulnerability of these workers to sustain injuries from such heights and a lack of knowledge about these accidents. The lack of availability of protective measures, such as harnesses and lanyards for these workers, is a serious social situation that warrants further investigation and remedial measures. Furthermore, there was a high incidence of TSI noted in low socioeconomic strata laborers in our study, with 53.5% (n=1,005) of TSIs occurring in people working in agriculture, construction, and manual labor.
Falls were the predominant mode of injury in recent studies; however, these were low falls (<1 m) sustained by elderly patients. In the present study, low falls were observed in 7.6% (n=159) of TSIs and predominantly occurred in people >60 years. Low fall was the most common etiology with 36% in a Finnish study, whereas low fall accounted for only 20% and 22% of injuries in studies based in Germany and China, respectively [9,11,12]. From a broader perspective, it is evident that studies quoting a higher incidence of TSIs due to low falls studied older populations and a lower incidence of unstable injuries, whereas studies documenting more TSIs due to high falls studied a younger population and high-velocity unstable injuries.
Most previous studies have reported RTAs to be the major cause of TSIs [13,14]. Studies by Oliver et al. [4], Pirouzmand [13], and Jackson et al. [14] reported MVAs as the major mechanism of spinal injuries at 54.7%, 66%, and 45.6%, respectively. However, improvements in road safety measures, civil infrastructure, and transport systems have contributed to a reduction in the incidence of TSIs due to RTAs in the Western world. In the present study, 42.1% of TSIs were related to MVAs. However, the majority of injuries were not sustained by car collisions. Interestingly, 52% of spinal trauma due to RTAs occurred in motorcyclists, which indicates the inherent danger of motorcycle riding in terms of sustaining a spinal injury. Further analysis indicated that 61.5% of TSIs in motorcyclists occurred due to a self-fall, indicating unsafe driving in this part of the world. Therefore, strict adherence to the rules of the road for driving safety could reduce this subset of trauma.
The mean age of the patients with TSI was 43.4±16.3 years, which was comparable to other studies. Notably, 77.3% of spinal trauma patients were aged 20–60 years, which is the social and economically productive age group of a society. This assumes a larger significance since we observed that SCI and neurological deficit was documented in 49% of patients.
In our study population, thoracic spinal injury was observed in 40.8%, cervical spinal injury was seen in 37.4%, lumbar spinal injury in 36.8%, and 10.5% patients had sacrococcygeal injuries. The predominant location of injury depends on the selected population subset. Population studies that describe a higher number of low falls sustained in elderly population have documented a higher incidence of lumbar and lumbosacral fractures [9,12,13]. Studies focusing on SCIs have indicated a higher number of cervical spinal injuries [15]. The present study also revealed a high (49.1%) incidence of spinal cord injuries, which was much higher than that reported in the literature. Apart from the higher incidence of high falls and motorcycle accidents, which are high-magnitude injuries that can cause vertebral translation, our center offers dedicated spinal rehabilitation services that could have led to this observation of a higher incidence of SCI. Injuries associated with other organ systems can affect the management and outcomes of patients with TSIs. The frequency of these injuries (49.1%) was similar to those reported in other studies, which showed frequencies of 38%–54% [12,16]. The average transit time of 20 hours noted in our study was much higher than a study conducted in Canada, which reported 2.5 hours [13].
The present study has some limitations. First, this was a retrospective study conducted at a single specialty center for trauma and orthopedics. Second, data maintenance was based on human data entry. Third, less serious spinal injuries could have been treated at smaller centers and more seriously injured patients who died before reaching the hospital could have been missed in the analysis.
Conclusions
Our study indicates different demographic patterns and epidemiological features of TSIs in developing countries compared with those reported in the Western literature. A preponderance of young male patients, high falls, motorcycle accidents, and a larger percentage of SCI were distinct observations in this large-scale study. Furthermore, the high number of workplace injuries indicates a lack of knowledge about safety measures of protection. TSIs currently affect a higher number of patients in lower socioeconomic strata and could be a preventable injury if improvements in awareness and public educational measures can be implemented.