Introduction
Low back pain (LBP) is the most common cause of disability in patients younger than 45 years of age and the second-most common reason for visiting a physician. LBP is also one of the most common work-related musculoskeletal disorders (MSDs), the third-most common reason for surgery, and the fourth-most common reason for hospitalization [1].
Most people will experience back pain at some point in their life but in some occupational sectors such as industrial workers, nurses, and drivers, it is more widespread than other groups [2].
In view of occupational health, LBP is among the most important reasons for absenteeism, impairment, disability, and workers' compensation. Worldwide, LBP results in decreased productivity and imposes enormous costs upon the patient, family, society, industry, and the government [3].
We should consider that LBP is not merely a disease, but also it is a sign of several systemic, musculoskeletal, and neurological disorders [2].
Determining the main causes of LBP is often difficult, and in general there is little consensus on its etiology and even its definition [1].
LBP is a multifactorial disease and many risk factors may contribute to its development and process, including psychological, ergonomic, and physical factors [4]. Also, work environmental factors such as employment support, the number of employees, social support from colleagues, and overall job satisfaction are factors influencing LBP [2]. In spite of several articles published, there are still many unresolved, basic questions regarding the development of LBP and its prognosis.
Considering that MSDs are among the most common work-related issues in industry and lead to numerous problems in the work force, identifying casual factors may help prevent LBP development and complications. This study was done to assess the occupational and individual factors that influenced the development of LBP amongst steel industry workers in 2015.
Materials and Methods
This cross-sectional study was conducted in a steel industry in Mashhad, Iran. We selected 358 male personnel by random sampling method, and divided them into two groups: production workers (201) and administrative personnel (157). Production workers were mainly involved in lathing, welding, melting and assembling. This group was required to do heavy and very heavy physical activities, statically and dynamically for more than 70% of their working hours, including repetitive manual handling, prolonged standing, repeated bending from the waist, and repeatedly climbing stairs. A worker was considered to be exposed to prolonged standing if he spent more than 50% of the total working hours (more than 4 hours in our study) during a full work shift in a standing position. Heavy work refers to lifting up to a maximum of 45 kg with frequent lifting and/or carrying of objects weight-ing up to 23 kg. Very heavy work refers to lifting more than 45 kg with frequent lifting and/or carrying of objects weighting 23 kg or more [5]. A job was considered to be repetitive when the duration of a task or group of tasks (a cycle) was less than 30 seconds. When cycles were longer than 30 seconds, the task was considered repetitive when the worker was performing the same motion for more than 50% of the cycle. Administrative staff mainly worked in administrative sections, and were sitting monotonously for at least 70% of their working time (at least 5.5 hours). The duration of each working shift in our study was 8 hours per working day.
The inclusion criteria were the employee's willingness to participate in the study along with at least one year of working experience at this plant. The exclusion criteria were a history of pre-employment LBP, traumatic spinal injury, a history of musculoskeletal disorders, and reluctance to participate in the study.
A modified Nordic questionnaire was used for collecting data in this study. The questionnaire consisted of three parts: (1) individual and demographic characteristics, including age, duration of employment, smoking and physical activity; (2) medical history; (3) history of LBP. The questionnaire was completed by a trained occupational health professional. In order to confirm a diagnosis in individuals reporting LBP, an occupational medicine specialist examined the patient.
LBP refers to “pain and discomfort localized below the costal margin and above the inferior gluteal folds, with or without leg pain” within the most recent 12 months. Patients who suffered from back pain were divided into two groups: (1) patients with non-specific low back pain (NSLBP), (2) patients with disk herniation. This classification was based on the patients' history, examination, MRI results (if applicable) and medical records.
Disk herniation was defined as a LBP causing leg pain, along with radiographic (MRI) evidence of disc herniation at the same side and level, leading to impingement, compression, or deviation of nerve tissue (as reported by a radiologist), or a patient with a valid medical certificate for disk herniation from a neurosurgeon or orthopedic surgeon. All steps of the study, including history taking, physical examination, and recording of the data were done by an occupational physician.
Non-specific LBP is defined as LBP that cannot be related to any specific disease such as fracture, infection, osteoporosis, inflammatory or tumoral disease, or radicular syndromes.
Height was measured while the subject was standing against the wall with feet flat, his legs straight, arms at his sides, shoulders level, and looking straight ahead. Weight was measured without shoes and while wearing light clothes. Body mass index (BMI) was defined as the weight in kilograms divided by the square of the height in meters. In this study, we considered a BMI of more than 25 as overweight. Patients who smoked at least one cigarette per day were considered smokers and all others were considered non-smokers.
After collecting data, we entered the information gathered through observations, interviews, and clinical examinations into computers. Statistical analysis was done using SPSS ver. 11.5 statistical software. We used descriptive statistical methods, including central measures, measures of dispersion, and frequency distributions; and analytical statistical methods such as chi-squared test, t-test and logistic regression were used in data analysis as well. Data were considered statistically significance at p<0.05.
The protocol for this study was approved by the Ethics Committee of Mashhad University.
Results
Based on our analysis, the mean age of the subjects and the duration of employment was 38.9±6.73 years and 13.04±5.70 years, respectively.
As seen in Table 1, age, duration, and BMI were similar in production workers and administrative workers.
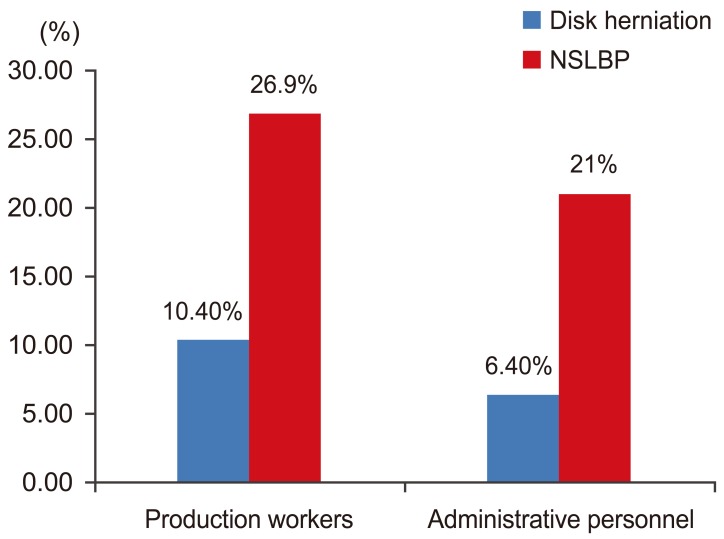
Two groups were not significantly different based on smoking status (p=0.56). Fig. 1 shows the type of LBP in production workers and administrative workers. Based on our analysis, there was a significant relationship between LBP and age, BMI, duration of employment, and leisure time physical activity (p≤0.05).
Table 2 shows the Comparison of non-occupational risk factors in patients with and without LBP.
To predict independent risk factors for LBP, the variables that showed a significant relationship with LBP (age, overweight, duration of employment and leisure time physical activity) were entered into the logistic regression model using the Backward method (R2=0.04). Only the duration of employment was statistically significant and can be considered an independent risk factor (p≤0.05). According to this analysis, each year of employment was associated with an 8% increase in the risk of LBP.
There was no relationship between LBP and known psychiatric disorders; 7.8% (9) of workers with LBP and 8.7% of workers without LBP had psychiatric disorders (p=0.7).
Discussion
Despite the young age and short employment duration of this cohort, the 1-year prevalence of LBP was high in this industry (32.4%). In a case-control study by Aghilinejad et al. [6] with 1,439 steel industry workers in Tehran, a high prevalence of musculoskeletal disorders was reported. Based on their study, the involved regions were most commonly back, knee and the neck. Also, they found a strong relationship of MSDs with BMI and the duration of employment.
In a case-control study conducted on 400 Indian steel workers in 2014, the overall prevalence of morbidities in the cohort was 60% and the highest morbidity was related to MSDs [7].
According to our findings, there is a considerable relationship between LBP and age. Similar results were obtained in previous studies [489]. The likely explanation for this association is that degenerative changes are hastened by the aging process [8]. Based on Sadeghian et al. [9], every 5-year increase in a worker's age correlates with a 1.46-fold increase in risk of LBP.
We showed that there is a negative relationship between LBP and leisure time physical activity. This was also observed in a cohort study by Mikkelsson et al. [10]. Physical activities can strengthen trunk muscles, and increase the body's endurance and movement abilities, resulting in better waist function [1011].
In our study, there was no relationship between LBP and smoking. This result is consistent with a study by Terzi and Altin [12]. However, in a meta-analysis by Shiri et al. [13], it was concluded that smoking cessation may reduce, but not completely eliminate, any excess risk; therefore they called smoking a “modest risk factor” for sciatica. However, there are other studies that reported smoking as an independent risk factor for LBP [1415].
According to the present study, there is a direct relationship between LBP and being overweight. Previous studies confirm the effects of this factor on intervertebral disc degeneration and the development of LBP [1617].
In addition, the results of our study showed that there is a significant relationship between LBP and the duration of employment. Similar results were obtained in previous studies [248].
Based on our study, there is no association between the development of LBP and current job status. According to a systematic review by Kwon et al. [18], previous studies did not support the association between occupational physical activities and LBP. This finding may be due to poor quality scientific literature and the difficulty of determining the cause of LBP. In a meta-analysis by Taylor et al. [19], the incidence of LBP was similar in the community and in the occupational setting. Based on the results of this study, there are multiple diverse physical and psychosocial risk factors for first-time LBP. In another meta-analysis, there was a moderate association between mechanical exposures and LBP, although this association was complex [20].
Eight systematic reviews, using the Bradford-Hill causation criteria, concluded that it is unlikely that occupational sitting, standing, and walking, awkward postures, pushing or pulling, manual handling, lifting, bending and twisting, or carrying are independent risk factors for LBP [21222324252627].
However, Lis et al. [28] showed that occupational sitting for more than a half workday, in combination with awkward postures, increases the likelihood of LBP develop-ment.
Our study is a cross-sectional study; therefore, it is possible that any observed relationship between LBP and risk factors are not causal relationship.
Considering that age, BMI, duration of employment, and leisure time physical activity showed a significant association with LBP but none of them, except duration of employment, were independent risk factors for LBP, it appears that there may be other risk factors of LBP, such as psychosocial factors, that were not considered in this study. According to previous studies, psychosocial factors can influence LBP development and chronicity; however, their results are somewhat challenging [2930]. Although our study didn't confirm a role of known psychiatric disorders in occupational LBP, patients were not specifically assessed according to psychosocial risk factors, which is a limitation of our study.
It seems clear that LBP is the result of the interaction of several occupational and non-occupational factors. In the future, longitudinal studies on relative importance of each individual risk factor and the effect of potential confounding variables are suggested to set a precedence for the prevention of LBP in the occupational setting.
Conclusions
We did not found any relationship between LBP and current occupational status, suggesting that the effects of general health-related factors such as weight, age, physical activity, and duration of employment are more important than occupational factors in the development of LBP. It is likely that lifestyle modification in combination with workforce education and ergonomic interventions will result in reducing the high rate of LBP and its related risk factors in this industry.