Introduction
Traumatic spine fractures are common injuries that have several causes, particularly falls from a height and road traffic accidents. If not treated properly, they can cause major disabilities, and approximately 12% of the patients who presented to the trauma unit in the emergency department of the Hamad Medical Corporation are classified in this category [1].
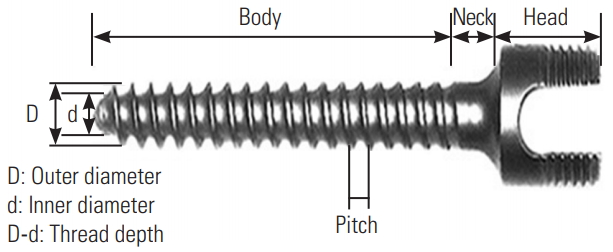
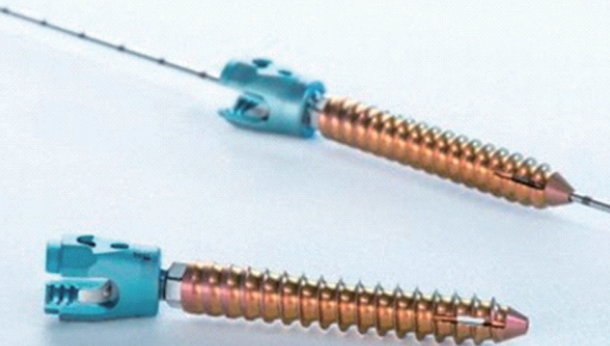
For unstable spine fractures, fixation is necessary; it is accomplished by either the open traditional technique or the minimally invasive surgery (MIS) technique that is gaining popularity among spine surgeons because of the lower risk of blood loss, decreased operation time, and lesser postoperative pain [2,3]. Cannulated (poly-axial head) pedicle screws (CS) that use a guide wire for screw insertion are considered the cornerstone of the MIS technique, while in the open technique, the use of solid core (mono-axial head) screws (SCS) remains a valid option [4-8] (Figs. 1, 2).
To our knowledge, several studies have investigated the physical characteristics of CS an SCS, such as bending performance, static and dynamic load to failure, and pullout strength, using biomechanical tests on cadaveric or constructed modules. However, few trials have assessed the radiological or clinical differences between these screws in non-English literature [4,5,9-12].
We aimed to compare the correction of the local kyphotic angle and the vertebral body height between the two types of screws and assess their effect on the superior and inferior angles of the screw with the rod.
Materials and Methods
A retrospective review of the medical charts of all patients with thoracolumbar fractures who underwent pedicle screw fixation with CS or SCS was performed, and these patients were followed up at the orthopedic spine department from January 2011 to December 2015 after obtaining approval from the medical research center.
Data regarding the general demographic characteristics (age and sex), comorbidities, injury characteristics (mode of trauma, level of injury, and fracture classification), surgery-related parameters (open versus MIS, CS versus SCS screw), and radiological parameters (superior and inferior angles between the screw and the connecting rod, local kyphotic angle, and vertebral body high) were collected at different follow-up intervals (preoperative, postoperative, and at 3, 6, and 9–12 months postoperatively).
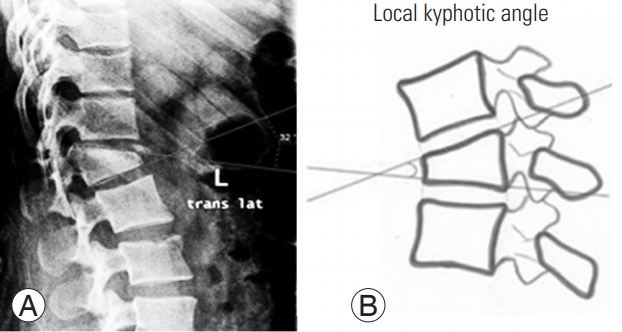
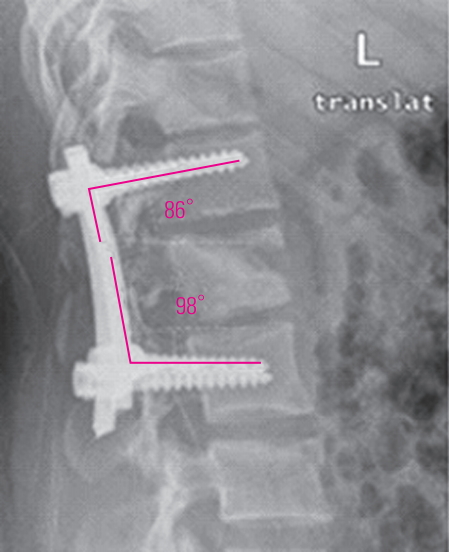
The local kyphotic angle is the angulation between the superior and inferior plates of the fractured vertebra [13] (Fig. 3). The vertebral body height (the percentage of height from the original height) was calculated by dividing the anterior wall height by the posterior wall height and then multiplying it with 100 [9] (Fig. 4). The superior angle is the angle between the rod and the superior screw, while the inferior angle is the angle between the rod and the inferior screw (two angles proposed by the research team to show the relationship between the rod and the screw) (Fig. 5).
Indications for surgery were an increase >30° in the kyphotic angle, loss of >50% in the vertebral body height, or neurological deficit. The choice of open or MIS surgery was made by the surgeon, based on his/her preference and experience, while the choice between CS and SCS was dependent on availability.
Frequency (percentage) and mean±standard deviation or median and range values are used to represent the categorical and continuous values, as appropriate. Descriptive statistics were used to summarize the demographic characteristics, injury characteristics, surgery-related parameters, and radiological parameters. Fisher exact test and chi-square test were used to evaluate the associations among two or more qualitative variables, while unpaired t-test and Mann-Whitney U-tests were used for the quantitative data. A 2-sided p-value <0.05 was considered statistically significant. All the statistical analyses used IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) and Epi Info 2000 (Centers for Disease Control and Prevention, Atlanta, GA, USA).
All the data were collected after ethical approval (approval no., 16158/16) was obtained from the Medical Research Center, the Hamad Medical Corporation, Doha, Qatar. Waived informed consent was taken for this retrospective study.
Results
Total 178 patients (average age, 36.1±12.4 years; men, 142 [84.3%]; women, 28 [15.7%]) with thoracolumbar fractures who underwent surgery and were followed up at the Hamad Medical Corporation were analyzed. The most commonly affected level was L1 in 37.1% of the patients, followed by L2 (in 18%) and D12 (in 17.7%) (Table 1).
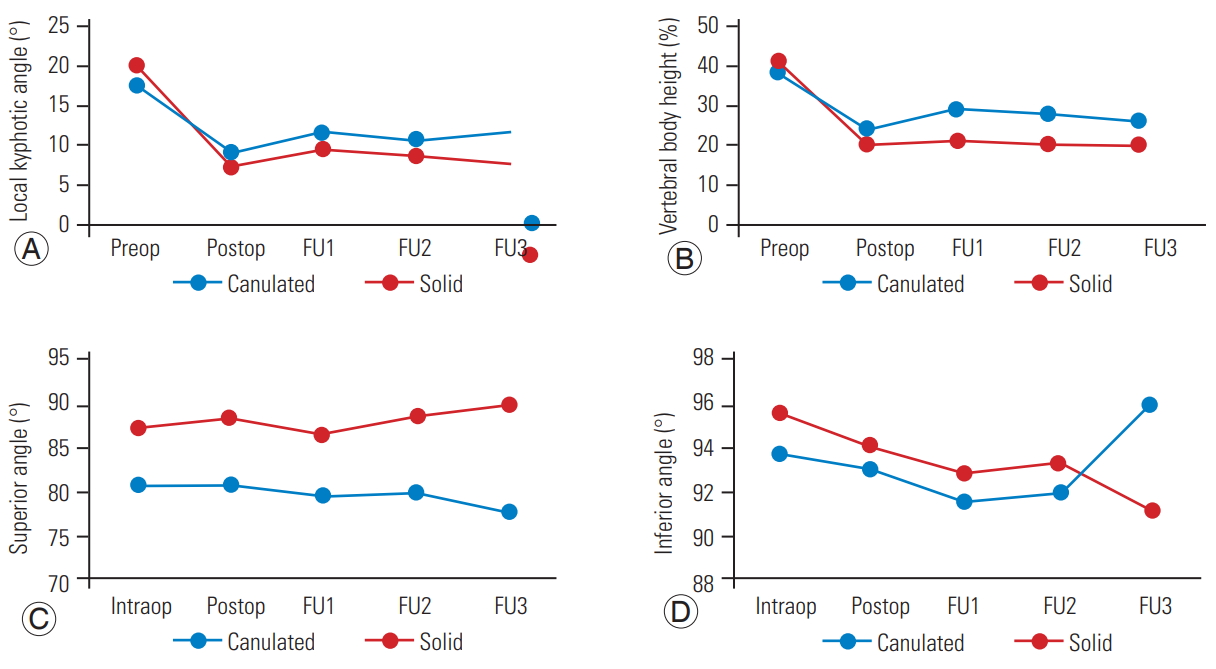
The average preoperative, postoperative, and final follow-up local kyphotic angles of the fractured vertebra were 17.4°±8.9°, 8.6°±6.9°, and 11.6°±6.4°, respectively, in the CS group, while these were 20.1°±10.7°, 7.1°±5.6°, and 7.5°±6°, respectively, in the SCS group. Surgical correction (i.e., the difference between the preoperative and postoperative local kyphotic angles) was significantly different between the CS group (8.8°±10.4°) and the SCS group (13°±11.2°, p=0.014). In contrast, the average loss of correction (i.e., the difference between the final follow-up and the postoperative local kyphotic angles) was not significantly different between the CS group (4.2°±5.9°) and the SCS group (9.5°±5.5°, p=0.117) (Table 2, Fig. 6).
The average intraoperative, postoperative, and final follow-up reductions in the vertebral body height of the fractured vertebra were 39.6%±28.2%, 23.5%±13.3%, and 26%±15.1%, respectively, in the CS group, and 41.5%±27.6%, 20.1%±12.6%, and 20.1%±15.5%, respectively, in the SCS group. The surgical correction of the reduction of the vertebral body height was significantly different between the CS (16.1%±14.9%) and SCS (21.4%±15%) groups (p=0.024). However, the average loss of correction of the reduction in the vertebral body height was 18%±13% and 20.2%±7.1% in the CS and SCS groups, respectively; this difference was not statistically significant (p=0.682) (Table 2, Fig. 6).
The difference between the postoperative and final follow-up superior and inferior angles was not statistically significant (p=0.324 and p=0.838, respectively), with an average superior angle of 4.5°±0.7° and -0.3°±6° in the CS and SCS groups, respectively, and an average inferior angle of 1.5°±4.9° and 0.8°±3.5° in the CS and SCS groups, respectively (Table 2, Fig. 6).
Discussion
Thoracolumbar fractures are common in Qatar and add a significant burden to the healthcare system. Qatar is a developing country with a rapidly growing population and infrastructure. The current data from the Hamad Medical Corporation, the main tertiary-care hospital in Qatar, show that annually, about 200 patients present with traumatic spinal injuries primarily attributed to motor vehicle accidents and falls from a height, making traumatic spinal fracture the leading cause of disability in this population [1].
A literature review showed no differences in the vertebral body height local kyphotic angle correction between the open and MIS techniques; however, the latter had a shorter operative time and less blood loss [2,3]. To our knowledge, this is the first study to compare the effect of CS and SCS on the local kyphotic angle and vertebral body height after spine fracture fixation. Many studies have compared the biomechanics of CS and SCS to show that the ultimate load, yield strength, and cycles to failure were significantly lower with the CS than with the SCS [4,5,10,11].
Another study performed biomechanical tests to compare the bending performance of the two types of screws and found that the latter has significantly poorer bending performance [9]. Other studies compared the effect of CS versus that of SCS on the stability of the construct after fixation, and they showed that incorporating a CS did not significantly decrease the construct’s stiffness [12].
The superior and inferior angles reflect the bending of the screw and impending failure and broken. Our study revealed changes in the superior angle during follow-up, with statistically significant differences between the CS and SCS in the first (p=0.001), second (p=0.001), and final follow-ups (p=0.006); however, no significant difference was observed between the postoperative and final followup (p=0.324). No statistically significant difference was detected in the inferior angle during the first, second, and final follow-ups (p=0.125, p=0.165, and p=0.092, respectively) or in the superior angle between postoperative and final follow-up (p=0.838) (Table 2).
We use both techniques in our hospital; generally, we use CS in MIS techniques and SCS for the open technique (Table 2). One of the most important limitations of the current study is the lack of correlation of the radiological findings with the functional outcome and complication rate. Another limitation is the relatively short follow-up duration; thus, long-term follow-up studies are warranted to evaluate the long-term complications and failure of both types of screws.